
Abstract
As knowledge and attitude towards performing basic life support and using an automated external defibrillator (BLS and AED) contribute equally to improving survival after out-of-hospital cardiac arrest, we aimed to develop a measuring instrument for a validated assessment of schoolchildrens' attitude towards BLS and AED. The objective was to identify, measure, and address pertinent attitude dimensions that influence the intention to actually perform BLS and AED. We conducted a BLS and AED course for seventh and ninth grade students. Students fulfilled pre- and post-course questionnaires on attitude and intention to perform BLS and AED. The measuring instrument was developed with the use of exploratory factor analysis with application of principal component analysis and confirmatory factor analysis with application of structural equation modeling. Measurement invariance across different groups (gender, grades, previous courses) was tested with Wilcoxon signed ranks test and Mann–Whitney U test. Differences in attitude pre- and post-course were evaluated by application of Mann–Whitney U test. The final attitude model consisted of 3 behavioral constructs (self-confidence, positive motivation, and amotivation). Self-confidence was the major construct directly affecting the intention to act. Positive motivation had a negligible direct effect on intention but correlated strongly with self-confidence. The effect of attitude on the intention to help is therefore less complicated than was expected, which relieves the non-professional educators of having to know the specifics of the different behavioral constructs.
Keywords
Attitude has not been explored yet with a validated instrument.
We explored school children’s attitude with a self-developed questionnaire.
Our findings help BLS and AED course developers and instructors to tailor courses according to target audience—schoolchildren.
Introduction
Efforts to improve survival after out-of-hospital cardiac arrest (OHCA) are increasingly focused on the first 3 links of the Chain of survival that describe measures leading to shortening the time to recovery of spontaneous circulation: recognition of cardiac arrest and activation of emergency services; early cardiopulmonary resuscitation (CPR); and early defibrillation. Current resuscitation guidelines 1 recommend strengthening these links through various activities, among which are effective CPR courses for adults and schoolchildren. However, research has shown that although people are trained in BLS they might still be reluctant to perform CPR in real life.2,3 It must therefore be emphasized that attitude (along with theoretical knowledge and skills) towards performing CPR could contribute significantly to improving survival after OHCA.2,4 Among the most frequent reasons for not providing bystander CPR were the impression of insufficient skills and fear of disease transmission.2,5-7 Other misperceptions include concerns about causing injury and inappropriate contact due to sexualization of women’s bodies 8 leading to women receiving CPR less frequently. 9 Proper, effective and systematic BLS training can address and attenuate hindrances on one hand 10 and effectively stimulate laypersons to act appropriately in cases of OHCA on the other. 11 Therefore, courses on BLS and AED should not be focused only on teaching theoretical knowledge and practical skills but also on changing erroneous attitudinal aspects.
CPR training in schools enables education of a wide population base and is therefore a vital part of disseminating knowledge and positive attitude towards CPR among laypersons.12-14 Such training is easy and cost-effective, especially if training is part of compulsory school activities, and is encouraged worldwide. 15 Schoolchildren are particularly susceptible and motivated for learning CPR, they can be easily and quickly taught,16-18 and even performed better and learned faster than adults in a study by Baldi et al 19 They serve as potential multipliers of CPR knowledge and positive attitude towards CPR in their environment. 20
Hence, understanding human behavior is important as human action is guided by attitude and subjective norms 21 which consist of various theoretical behavioral constructs. A combination of intrinsic and extrinsic motivation, amotivation, self-confidence, and self-efficacy (situationally specific type of self-confidence)22-24 produce behavioral intention and result in actual behavior. As the latter can not be empirically measured in models because the chances of performing BLS in a real situation are small, the construct of measurable intention serves as a proxy. To ensure meaningful inference from a theoretical construct and to justify instrument use in practice it is important to carefully design and validate the construct of schoolchildren’s attitude and intention towards BLS and AED 25 in order to help course developers and instructors to tailor courses for this specific population.
The purpose of this study was to objectively explore schoolchildren’s attitude towards BLS and AED and obtain information on the determinants that influence their intention to provide BLS and AED in a real situation.
Methods
Setting
Individual regions and schools in Slovenia voluntarily take advantage of various BLS courses offered either by the National Institute for Public Health or other local organizations and initiatives.
The Course
Our BLS and AED course was organized in collaboration with the City Municipality of Maribor and was designed and intended for 7th and 9th grade students of compulsory 9-years basic school and was identical throughout the study. The structure was identical throughout the study. Average age of children in seventh and ninth grade is 12 to 13 and 14 to 15 years, respectively.
The course was divided into 2 parts. The first part was a 45-minute interactive lecture by an emergency physician on principles of BLS and AED. Children were encouraged to participate with questions and own experience. The course continued with a 45-minute practical workshop for each individual class consisting of up to 30 students. Each student practiced on their own training torso manikin (Prestan Professional Adult Manikin, Prestan, Mayfield Village, OH, USA) along with an AED prop—a cardboard sample with adhesive paper electrodes. A single real training AED (Defibtech Trainer AED, Defibtech, Guilford, CT, USA) was used for guidance and cardiac arrest simulation. Before and after the course students filled out a questionnaire described below.
Theoretical Model
The model was based on a combination of Ajzen’s theory of planned behavior and theoretical constructs rooted in Ryan and Deci’s and Bandura’s theories.21-24 The model with such combination of constructs can be regarded as a novelty in the field of public health. In a preparatory phase of the study authors were not able to find similar studies, however, similar constructs were already included in a number of behavioral studies in different fields such as sport, education and medicine.26-28
The hypothesized theoretical model of schoolchildren’s attitude consisted of factors that potentially influence the intention to perform BLS and AED and thereby indirectly indicate presumed behavior (providing BLS and AED): intrinsic motivation, extrinsic motivation, amotivation, self-efficacy, and self-confidence. We predicted that each of these latent constructs will statistically significantly influence behavioral intention to help. Additionally, it was hypothesized that these endogenous constructs correlate among themselves (Figure 1). Theoretical model of influence of attitude dimensions on schoolchildren’s intention to perform BLS and AED.
Study Design
The study was divided into 2 main parts following traditions of exploratory and confirmatory analysis (Exploratory phase and Confirmatory phase, respectively). Objectives of Exploratory phase were: to develop a theoretical model of influence of different factors on the intention to perform BLS and AED; to develop and validate an instrument to accurately measure attitude towards and intention to perform BLS and AED among schoolchildren; and to identify main theoretical constructs that compose schoolchildren’s attitude towards BLS and AED.
After exploration of the factorial structure and reliability of the model and the questionnaire the objectives of the Confirmatory phase were: to assess the change in intention to perform BLS and AED among schoolchildren after a BLS and AED course; and to identify attitude dimensions that need to be emphasized or specifically addressed in educational courses to promote prosocial behavior—intention to perform BLS and AED.
Questionnaires were handed out immediately before the lecture and immediately after the practical workshop. Individual statements on the attitude questionnaire were changed, omitted or substituted during the course of the study following a construct validity approach to yield the final version in the Confirmatory phase. The content of the pre- and post-course questionnaire was identical in individual versions in the Exploratory phase. In the Confirmatory phase, the pre-course questionnaire contained only statements on intention, whereas the post-course questionnaire contained all statements on intention and attitude as it is the post-course attitude that the students transfer into their home environment and is therefore the key. The instrument did not require the provision of a name to assure anonymity. However, students were asked to come up with codes that would be used on the pre- and post-course questionnaire for the purpose of pairing questionnaires of the same individuals for further analyses.
The following research questions were formulated: (1) What constitutes school children’s attitude towards BLS and AED? and (2) What influences the intention to act (perform BLS and AED) of schoolchildren in a real life situation of cardiac arrest?
Measuring Instrument—The Questionnaire
The instrument consisted of 3 parts.
(a) Demographic data (gender, school grade, previous attendance to any BLS, and AED course). (b) Validated knowledge test.
29
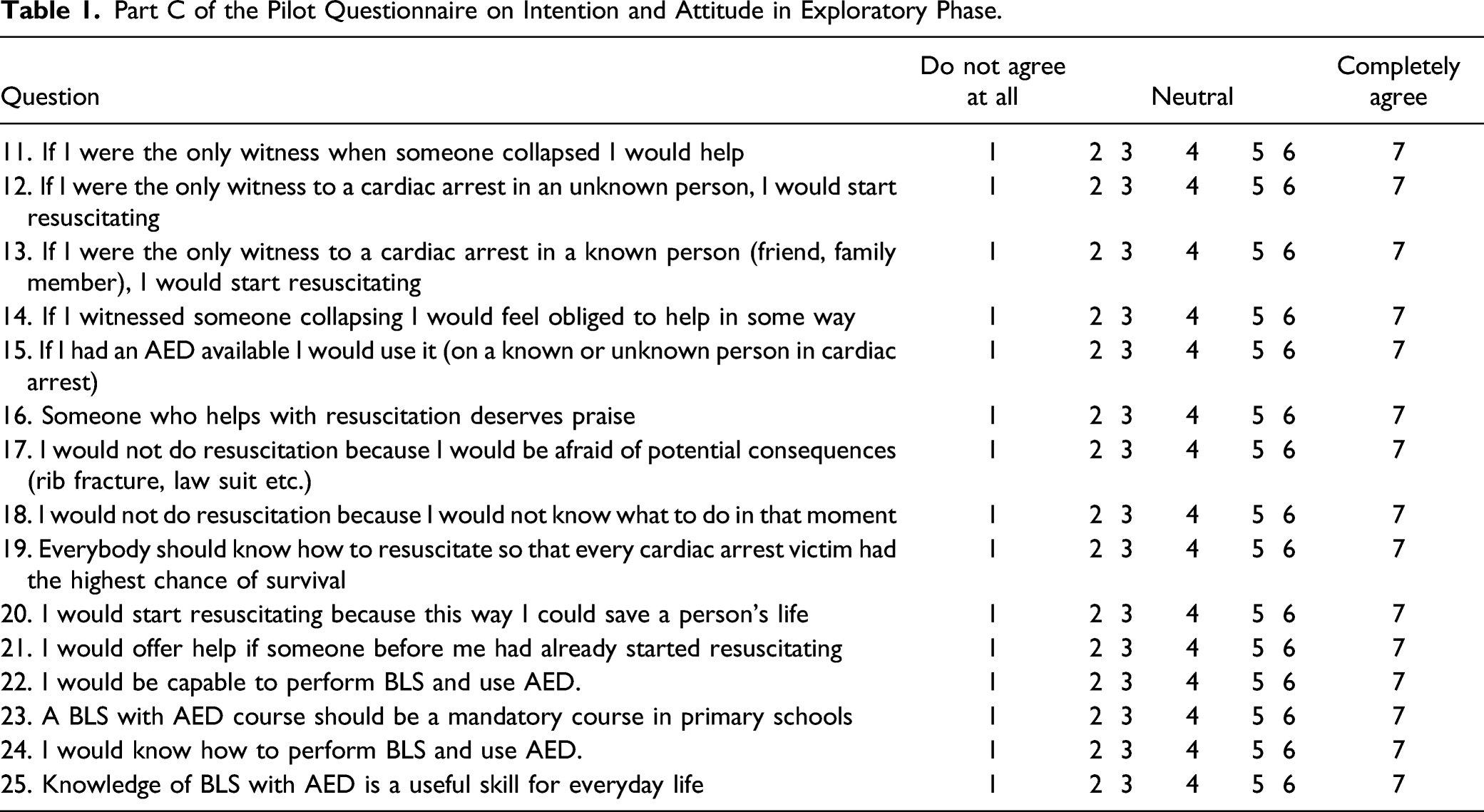
(c) Attitude questionnaire consisting of 4 statements regarding intention to act and 11 statements regarding attitude towards BLS and AED with 7 possible levels of agreement in range from 1 - “do not agree at all” to 7 - “totally agree,” and 4 regarded as neutral. Three statements were constructed in a reverse manner to force participants to read the statements carefully and prevent the tendency to respond in the same pattern throughout the questionnaire. Disagreement with these statements can therefore be regarded as wishful behavior. With this recalculation in mind someone who will disagree with all statements will collect 15 points, and someone who will completely agree with all statements will collect 105 points, respectively, with 60 as a median. This part of the instrument battery was developed with Theory of Planned Behavior,
21
Self-Determination Theory,22,23 and self-efficacy (self-confidence)
24
in mind. The pilot attitude questionnaire is presented in Table 1. Part C of the Pilot Questionnaire on Intention and Attitude in Exploratory Phase.
Sample and Sampling
Elementary schools that coincidentally applied for the course in the time frame of the study were included in the study, that is from November to December 2017 for Exploratory phase and October to December 2018 for Confirmatory phase. In follow up statistical analyses only data from students that fulfilled both pre- and post-course questionnaires were included.
In the Exploratory phase 459 students were included (218 boys and 241 girls; 248 7th grade and 211 9th grade) and in the Confirmatory phase there were 324 (175 boys and 148 girls; 151 7th grade and 173 9th grade).
In addition to full anonymity, each student had to state his or her agreement with fulfilling the questionnaire. General written consent of parents for such type of educational research is collected in advance at the beginning of each school year.
Statistical Analyses
Exploratory Factor Analysis (EFA) with the application of Principal Component Analysis (PCA) and Confirmatory Factor Analysis (CFA) with the application of Structural Equation Modeling (SEM) were conducted to construct and validate an instrument for measuring schoolchildren’s attitude towards BLS and AED. IBM SPSS Statistics, version 25 was used for PCA and IBM SPSS AMOS 24 for CFA and SEM (SPSS Inc, Chicago, IL, USA).
EFA was conducted on each construct and on combined sets of data in the pilot study. Spearman’s correlations among statements were examined and statements that correlated with all other statements less than 0.4 and more than 0.8 were deleted from further analysis to prevent error, unreliability, and multicollinearity. 30 Following Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy (>0.70) and Barlett’s test of sphericity (P < .05)31,32 EFA was applied to determine principal components and explain variance in terms of Eigenvalues. Initial number of components was extracted by criterium Eigenvalue >1; Statements with component loading below 0.50 were excluded from the poll. 33 Cronbach’s alpha coefficient was used to measure reliability of the entire scale and extracted components with values above 0.70 denoting acceptable internal consistency of the statements. 33
CFA was applied to explore correlations among theoretical constructs and to assess a model’s goodness-of-fit. In the Confirmatory phase, CFA was applied to the sample with no missing data (N = 265) to test the model constructed in the Exploratory phase. SEM was conducted to examine the influence of attitude dimensions on the intention to perform BLS and AED.
To estimate measurement invariance across 2 cohorts (boys and girls; 7th and 9th grade; previous attendance to BLS and AED courses) Wilcoxon signed ranks test was applied in addition to Mann–Whitney U test.
Differences in intention between pre- and post-course questionnaires were evaluated by application of Mann–Whitney U test. Effect sizes were calculated with the use of an online engine. 35
Results
Sociodemographic Characteristics of the Samples in Exploratory and Confirmatory Phase.

Exploratory Phase
Reliability of the entire attitude scale with the initial 11 statements pre- and post-course was confirmed with the value of Cronbach’s alpha of 0.84. Constructs were improved in a series of 3 cohorts of students.
Theoretical Constructs and Coded Corresponding Statements on Questionnaires in Exploratory and Confirmatory Phases.

Special attention was given to the construct of intention with its 4 corresponding statements as a possible predictor of actual behavior. Based on correlation criteria 0.40 < r < 0.80 statement INT-4 was excluded from the initial pool of the construct. Retained statements were adequate for PCA based on the results of KMO and Bartlett’s test of sphericity (0.77 and P < .001, respectively). As expected, only 1 principal component (i.e., the construct of intention) was extracted from the 3 retained statements with an Eigenvalue of 3.18, explaining 53.03% of variance.
Confirmatory Phase
Hypothesized model was tested by SEM analysis whereby several flaws were observed (e.g., correlations greater than 1; see Figure 2). Therefore, we abandoned the model regardless of acceptable fit indices and proceeded with construction of alternative models (Supplementary Material 3). SEM analysis of the hypothesized Model 1.
PCA of the entire set of statements on attitude (KMO: 0.83, Bartlett’s test of sphericity: P < .001) revealed that 13 suitable statements (component loadings of at least 0.50) formed 3 components explaining 49.71% of total variance (Supplementary Material 4). Factorial validity for the three-component structure of the 13-statement attitude questionnaire was confirmed through the use of CFA in the final model (Figure 3). SEM analysis of the final Model 2.
One component was composed of statements that incorporate a sense of belief in oneself and was regarded as a construct of self-confidence in further analysis. Statements on intrinsic and extrinsic motivation that constructed the second component in essence reflected positive motivation; therefore, the second construct was named as such. The third component represented the initially predicted construct—amotivation.
Correlations between constructs were strongest between self-confidence and positive motivation (0.77). Correlations between self-confidence and amotivation; and amotivation and positive motivation were weak (0.38 and 0.21, respectively). All were lower than .85, reflecting non-redundancy among constructs measuring attitude toward BLS and AED.
The intention to perform BLS and AED was well represented only by self-confidence which had a large effect (0.87), whereas amotivation had a negligible effect (−0.01), and positive motivation had a small negative effect (−0.11). 37
Measurement Invariance of the Questionnaire
Measurement Invariance of the Questionnaire Across Different Groups.

Note. INT, statement on intention; *, in favor of 7th grade; †, in favor of girls. Text of the statements is provided in Table 3.
Change in Intention to Perform BLS and AED From Pre-to Post-Course (Both Studies).

Note. SD, standard deviation; pr, pre-course; po, post-course. Text of the statements is provided in Table 3.
The final version of the joined knowledge test and attitude questionnaire is available as Supplementary Material 1.
Discussion
In this study, we developed and validated an instrument for assessing schoolchildren’s attitude towards BLS and AED and their intention to provide it in real life situation. Based on Ajzen’s theory of planned behavior we had constructed a theoretical model of schoolchildren’s behavior consisting of 5 theoretical constructs from Ryan and Deci’s and Bandura’s theories21-24: intrinsic and extrinsic motivation, amotivation, self-efficacy, and self-confidence.
In contrast to our prediction, schoolchildren’s attitude towards BLS and AED was not strictly specified by different subtypes of motivation and self-confidence. After testing several models the best goodness-of-fit was achieved with the model that consisted of only 3 theoretical constructs that reflected concepts of positive motivation, amotivation, and self-confidence and were therefore named as such. As it turned out, schoolchildren’s motivation in regard to performing BLS and AED was not specifically differentiated into intrinsic and extrinsic, but could be more generally regarded as a single construct of positive motivation (incorporating both intrinsic and extrinsic) on one hand and negative motivation (amotivation) on the other. Furthermore, statements that constituted the third construct reflected a sense of belief in oneself and self-efficacy that is commonly understood as self-confidence. This potentially makes the educators' effort to motivate schoolchildren to perform BLS and AED easier as they need to focus on positive motivation in general regardless of its intrinsic or extrinsic nature. The same applies to self-confidence in regard to BLS and AED—educators need to focus on the commonly understood construct of self-confidence, obviating the need to understand specific forms of the construct in detail.
Results showed that attitudinal dimensions do in fact influence the intention to perform BLS and AED. However, in this particular aspect the construct of motivation may not be as important as was predicted. In the three-factor structure of our model of schoolchildren’s behavior (i.e., intention to perform BLS and AED) the construct of self-confidence had the largest direct effect on intention. Interestingly, amotivation had practically no effect and positive motivation had a negligible negative effect on intention. The major factor in children of school age that was well linked to the intention to act was the level of self-confidence. It has been previously reported that impression of insufficient skills (as indicators of low self-confidence) are among common reasons for not providing bystander CPR.2,5-7 Hence, boosting self-confidence increases intention and presumably also actual performance of BLS and AED in case of witnessing a cardiac arrest in a real life situation. Keeping in mind that self-confidence was strongly related to positive motivation, special emphasis should be placed on the latter during BLS and AED courses for schoolchildren. Interestingly, there was only little correlation between self-confidence and amotivation and amotivation and positive motivation. However, it must be emphasized that these results only reflect relations among variables as they were assessed and do not allow causality inference.
The measuring instrument is suitable for both girls and boys, 7th and 9th grades and regardless of previous BLS and AED course attendance. Significant differences were noted between boys and girls and different grades but the effect sizes were small, possibly indicating that differences were generic due to inherent differences between genders and age rather than an indicator of the test’s measurement discrimation. Measurement invariance of the developed instrument across gender and 2 different grades can therefore intuitively be applied. This is another welcome news for educators as they need not discriminate between boys and girls, different grades or their baseline knowledge as they all respond in a similar manner.
There was a clear positive shift in the intention to perform BLS and AED after the course compared to baseline intention. The attitude at the end of the course was also very favorable and this should be the goal of all courses. We can speculate that the change was a result of multiple factors, among which was boosting self-confidence during the course which was shown to be the major influencing factor for the intention to provide BLS and AED in a real life situation of cardiac arrest. We empowered children with knowledge through an interactive lecture tailored to their level of understanding and thereby resolved potential erroneous perceptions and other prejudice regarding BLS and AED. Also, all instructors could speak from their own practical experience and address numerous questions and doubts that students exposed. Even though superiority of health care workers as educators has not been shown by previous research12,38 speaking from own experience seemed to impress the students. On the other hand, teaching schoolchildren in BLS may help different teacher (educator) profiles improve their teaching skills and support implementation of the “Kids save lives” statement as was suggested by Beck et al 39 in case of medical students as teachers. Additionally, with practical individual hands-on training on manikins children were able to recognize their skills and capabilities which further enhanced their self-confidence. Different authors have emphasized the benefits of early onset of such courses and of practical training on a regular basis.2,40,41 Identifying and understanding the attitudinal dimensions that influence the intention to provide BLS and AED aids in formation of effective “user-oriented” courses that encourage motivating factors and alleviate negative erroneous perceptions.
Limitations of the Study
Courses were led by 3 different instructors. The content of the course was predetermined and based strictly on the latest resuscitation guidelines with which the instructors, all of which are emergency physicians—and their paramedic assistants are perfectly familiar with as per their profession. Therefore, there could not be any inter-instructor variability in this respect. The authors have acquired all reasonable measures to alleviate possible bias. However, the sole process of educating and training includes a variety of uncontrollable factors, such as personal attractiveness, assertiveness, communication skills of the instructor on 1 hand, and students' momentary and general attentiveness on the other. Furthermore, methodology used in development and validation of the questionnaire was unique in the medical community and was applied only locally in schools in Maribor which could potentially present a limitation. Further studies in other regions would be necessary to ensure replicability of the results. Also, other factors (such as knowledge) that potentially influence self-confidence and intention need to be explored.
Conclusions
According to our validated questionnaire schoolchildren’s attitude towards BLS and AED appears to be less complicated than was expected. Self-confidence is the major construct directly affecting the intention to act, whereas positive motivation and amotivation play only minor roles. However, positive motivation is closely related to self-confidence and thereby indirectly affects the intention to act which is welcome news for non-professional educators as it obviates the need to differentiate among the different and complex theoretical constructs.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211056223 – Supplemental Material for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211056223 for Balneotherapy for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use by Vesna Borovnik Lesjak, Andrej Šorgo and Matej Strnad in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580211056223 – Supplemental Material for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use
Supplemental Material, sj-pdf-2-inq-10.1177_00469580211056223 for Balneotherapy for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use by Vesna Borovnik Lesjak, Andrej Šorgo and Matej Strnad in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-3-inq-10.1177_00469580211056223 – Supplemental Material for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use
Supplemental Material, sj-pdf-3-inq-10.1177_00469580211056223 for Balneotherapy for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use by Vesna Borovnik Lesjak, Andrej Šorgo and Matej Strnad in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-4-inq-10.1177_00469580211056223 – Supplemental Material for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use
Supplemental Material, sj-pdf-4-inq-10.1177_00469580211056223 for Balneotherapy for Validated Assessment of Schoolchildren’s Attitude Towards Basic Life Support and Automated External Defibrillator Use by Vesna Borovnik Lesjak, Andrej Šorgo and Matej Strnad in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
We would like to thank all participating elementary schools in Maribor and the instructors for making this study possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Approval from the National Medical Ethics Committee (Ministry of Health of republic of Slovenia) has been granted (dated October 23, 2018; filed under 0120-549/2017/9).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.