
Abstract
Background
Brain metastasis is an important cause of breast cancer-related death.
Aim
We evaluated the relationships between breast cancer subtype and prognosis among patients with brain metastasis at the initial diagnosis.
Methods
The Surveillance, Epidemiology, and End Results database was searched to identify patients with brain metastasis from breast cancer between 2010 and 2015. Multivariable Cox proportional hazard models were used to identify factors that were associated with survival among patients with initial brain metastases. The Kaplan–Meier method was used to compare survival outcomes according to breast cancer subtype.
Results
Among 752 breast cancer patients with brain metastasis at diagnosis, 140 patients (18.6%) underwent primary surgery and 612 patients (81.4%) did not undergo surgery, while 460 patients (61.2%) received chemotherapy and 292 patients (38.8%) did not receive chemotherapy. Multivariable analysis revealed that, relative to HR+/HER2– breast cancer, HR–/HER2– breast cancer was associated with significantly poorer overall survival (hazard ratio: 2.52, 95% confidence interval: 1.99–3.21), independent of age, sex, race, marital status, insurance status, grade, liver involvement, lung involvement, primary surgery, radiotherapy, and chemotherapy. The median overall survival intervals were 12 months for HR+/HER2−, 19 months for HR+/HER2+, 11 months for HR−/HER2+, and 6 months for HR–/HER2– (P < .0001). Relative to HR+/HER2– breast cancer, HR–/HER2– breast cancer was associated with a significantly higher risk of mortality among patients, and the association was stronger among patients who received chemotherapy (p for interaction = .005).
Conclusions
Breast cancer subtype significantly predicted overall survival among patients with brain metastasis at diagnosis.
What do we already know about this topic? Breast cancer patients with brain metastasis at diagnosis are rare, and further research on the subtypes of breast cancer and the prognosis of this population is warranted. How does your research contribute to the field? The current study showed that breast cancer subtype significantly predicted overall survival among patients with brain metastasis at diagnosis, and that chemotherapy played an interactive role in the association between breast cancer subtype and mortality. What are your research’s implications towards theory, practice, or policy? This study can provide a basis for future research and help develop care protocols for breast cancer patients with brain metastasis at diagnosis.
Introduction
Among solid tumors, breast cancer (BC) is the second most common cause of brain metastasis (BM), 1 with a proportion of .4–4.3% at first diagnosis.2,3 Metastatic breast cancer has a poor prognosis (median overall survival [OS]: 2–25.3 months), 4 although the development of new and more effective treatment options has improved patient survival and increased the likelihood of patients developing BM.5,6 Previous studies have shown that HER2-negative and triple-negative breast cancer (TNBC) breast cancer subtypes have a higher incidence of brain metastasis (BM) at initial BC diagnosis;7,8 however, there are also studies that show that HER2-positive and TNBC subtypes have a higher incidence of BM at initial BC diagnosis. 2 Thus, additional studies are needed to affirm the characteristics of breast cancer subtypes for BC patients with BM.
Data from a single institution have indicated that surgical resection and systemic therapy are effective treatments for BM in BC patients.9,10 Although the blood-brain barrier limits delivery of systemic treatments, the combination of chemotherapy and anti-angiogenic drugs can produce a high objective response rate to metastatic brain tumors in BC patients. 11 Furthermore, retrospective cohort studies have demonstrated the survival benefit in metastatic breast cancer patients via the surgical removal of primary tumors and systemic treatments.12,13 Although previous studies have analyzed the relationship between newly diagnosed BM patients and subtypes, no further analysis of prognostic factors of breast cancer has been performed.3,7,14,15 Therefore, the present study conducted an analysis based on the Surveillance, Epidemiology, and End Results (SEER) database to evaluate the association between the mortality of BC patients with BM and the molecular phenotypes of breast cancer.
Methods
Study Design and Data Source
The SEER database was searched to identify patients with BM at the initial diagnosis of stage IV breast cancer between 2010 and 2015. The SEER database contains data regarding demographic characteristics, clinical characteristics, tumor morphology, breast cancer subtype, stage at diagnosis, marital status, insurance status, first treatment, and survival outcomes. We signed SEER data-use agreements to access the data retrieved from this data-set. The retrospective study protocol was approved by our institutional review board, which waived the requirement to obtain informed consent as the patient data were anonymized.
The exclusion criteria were (1) a post-mortem diagnosis (based on autopsy or the death certificate), (2) no brain involvement at diagnosis, and (3) missing data regarding radiotherapy and surgery. Based on the inclusion and exclusion criteria, 752 patients were included in the analysis (Supplemental Figure 1). The study variables included age at diagnosis (<60 years and ≥60 years), sex (female and male), race (white, black, other, and unknown), American Joint Committee on Cancer (AJCC) T classification (T1, T2, T3, and T4), AJCC N classification (N0, N1, N2, and N3), disease grade (I, II, III, IV, and unknown), subtype (HR+/HER2−, HR+/HER2+, HR−/HER2+, and HR−/HER2−), marital status at diagnosis (married, unmarried, and unknown), insurance status (insured, uninsured, and unknown), bone involvement at diagnosis, liver involvement at diagnosis, lung involvement at diagnosis, survival status, survival time, and type of treatment (radiotherapy, chemotherapy, and surgery) for the primary site. 16
Statistical Analysis
Demographic and biological characteristics were compared using the chi-squared test. Univariate Cox proportional hazard models were used to identify factors that were associated with mortality. Multivariable analyses were performed to identify breast subtypes associated with mortality. We also adjusted for factors that, when added to the model, changed and matched hazard ratios by at least 10% and were clinically significant variables. Both non-adjusted and multivariate-adjusted models were used. The results were reported as hazard ratio (HR) and 95% confidence interval (CI). Subgroup analyses were performed according to age, liver involvement, lung involvement, surgery, radiotherapy, and chemotherapy. The Kaplan–Meier method and log-rank test were used to compare survival estimates. Landmark survival percentages at 12, 24, 36, and 60 months and median OS (95% CI) were reported by subtype. 17 We constructed nomograms incorporating factors that may influence the prognosis of BC patients with BM. All statistical analyses were performed using R software (version 3.3.2; http://www.R-project.org) and Free Statistics software (version 1.1). Differences were considered statistically significant at P-values of <.05.
Results
Baseline Characteristics According to Breast Cancer Subtype
Demographic and clinical characteristics de novo IV patients with brain metastasis grouped by subtypes.

Abbreviations: AJCC, American Joint Committee on Cancer; HR, hormone receptor; HER2, human epidermal growth factor 2
*P < .05; **P < .01; ***P < .001.
Notes: data presented are N (%). HR+/HER2-,(Luminal A); HR+/HER2+, (Luminal B); HR-/HER2+,(HER2 enriched); HR-/HER2-,(Triple Negative).(1)including American Indian/AK Native, Asian/Pacific Islander; (2)including Divorced/Separated/Single (never married)/Unmarried or Domestic Partner/Widowed; (3)including Any Medicaid/Insured(No specifics).
Univariable and Multivariable Analyses
Association between breast subtypes and mortality.

Abbreviations: CI, confidence interval;ORs, Hazard ratios, Ref.: reference.
*P < .05; ***P < .001.
Notes: data presented are HRs and 95% CIs. Adjust I model adjusts for Age, Sex and Insurance status; adjust II model adjusts for adjust I+ Grade, Marital status; adjust III model adjusts for adjust II+ Liver involvement, Lung involvement, Surgery, Radiation, and Chemotherapy.
Subgroup Analyses
Subgroup analyses of the association breast subtypes and mortality.
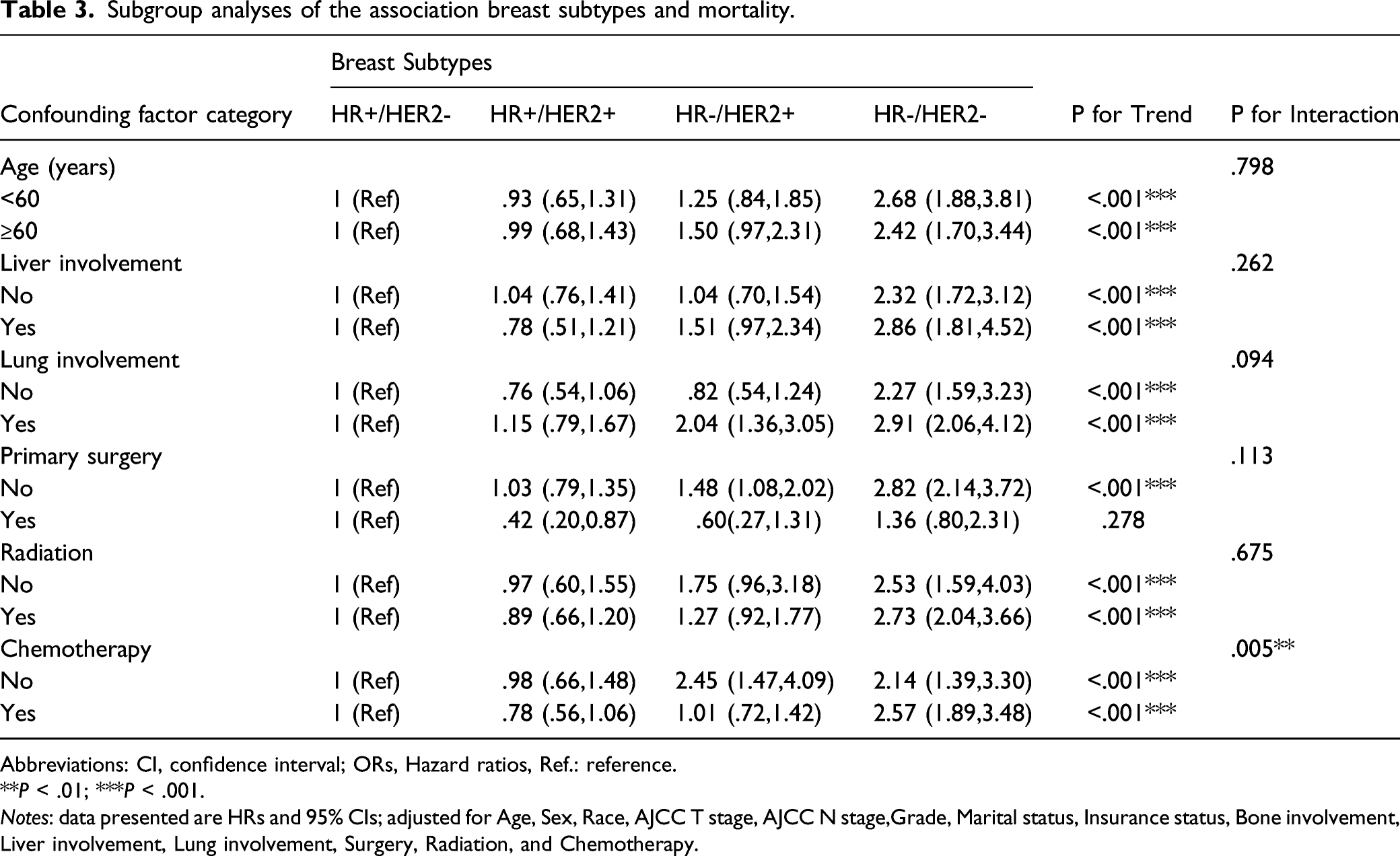
Abbreviations: CI, confidence interval; ORs, Hazard ratios, Ref.: reference.
**P < .01; ***P < .001.
Notes: data presented are HRs and 95% CIs; adjusted for Age, Sex, Race, AJCC T stage, AJCC N stage,Grade, Marital status, Insurance status, Bone involvement, Liver involvement, Lung involvement, Surgery, Radiation, and Chemotherapy.
Survival Curve Analysis and Prognostic Score
The median OS intervals were 12 months for HR+/HER2−, 19 months for HR+/HER2+, 11 months for HR−/HER2+, and 6 months for HR–/HER2– (P < .0001, Supplemental Figure 2A, Supplemental Table 2). The median OS intervals were 6 months for patients who did not receive chemotherapy and 15 months for patients who did receive chemotherapy (P < .0001, Supplemental Figure 2B). Furthermore, the score of each variable was determined according to the regression coefficient of each variable in the multivariate Cox model, so as to construct the overall prognosis score integrating these 6 parameters (Supplemental Figure 3). The nomogram showed medium accuracy in predicting the OS, with a C-index of .63 (95% CI = .60-.66) (Supplemental Figure 4).
Discussion
In breast cancer cases, BM is a type of distant metastasis that is associated with a poor prognosis. 3 In the US, 12% of women will be diagnosed with breast cancer during their lifetime. 18 In addition, the mortality outcomes vary according to breast cancer subtype in patients with BM, despite the use of various active treatments. 19 Therefore, the present study aimed to evaluate whether mortality varied according to subtype in patients from the SEER database who were diagnosed with stage IV breast cancer and BM, as well as the potential effects of different treatment strategies.
The HR+ and TNBC subtypes reportedly have the highest rates of BM, 20 and the subtype distributions in our study were similar to previously reported results. 21 The present study revealed that patients with the HR+/HER2– subtype had the highest incidences of bone metastasis, liver metastasis, and lung metastasis. Furthermore, bone metastasis was the most common location among all patients, which suggests that this group of patients may have special molecular/biological characteristics and require careful screening and follow-up. Further studies are needed to determine whether the T classification, N classification, and pathological grade are related to the incidence of BM.
We found that, among patients who were diagnosed with BM and breast cancer, poor OS was significantly associated with older age, black race, grade III disease, unmarried status, uninsured and unknown insurance status, liver and lung involvement, no primary surgery, no radiotherapy, and no chemotherapy. Similarly, a previous study of US patients with stage IV breast cancer revealed that OS was significantly associated with age, hormone receptor status, insured status, breast subtype, and stage at diagnosis.14,22 Our multivariable model also revealed that, relative to patients with the HR+/HER2– subtype, higher mortality was observed for patients with the HR–/HER2+ subtype (HR: 1.33) and the HR–/HER2– subtype (HR: 2.52, p for trend < .0001). Another previous study has indicated that the breast cancer subtype influenced survival after the development of distant metastasis.23,24
Among patients in the US, the median OS values for the 4 breast cancer subtypes ranged from 6 months to 19 months, which is shorter than in the Chinese population, based on a review of 2087 patients with metastatic breast cancer who had a median OS of 23.7 months after the diagnosis of BM. 2 Breast cancer-specific outcomes reflect the disease-free interval and OS interval. 25 Therefore, we analyzed OS according to breast cancer subtype among patients with BM, which revealed that the HR+/HER2+ subtype was associated with the longest median OS (19 months), while the HR–/HER2– subtype was associated with the shortest median OS (6 months). Patients with BM might benefit from increased surveillance and radiotherapy.26,27 That population-based cohort study detected a significant difference in mortality among patients with BM, although it lacked data regarding number of BMs, site, and radiotherapy. 14 We also built a prediction model in the collection of newly diagnosed patients with BMs to better predict the relationship between subtypes and mortality, and the accuracy and specificity of prediction needs to be further verified.
Surgery for the primary tumor was associated with significantly improved survival among patients with a single distant metastasis from metastatic TNBC. 28 Real-world data also indicate that neoadjuvant systemic therapy and surgery provide better survival than surgery alone. 29 The present study provides population-based estimates of the proportion of patients who underwent surgery as primary treatment, which may be beneficial for improving their OS outcomes.
There is a lack of consensus regarding the efficacy of chemoradiotherapy for BM from breast cancer, although the combined treatment appears to be safe.30-32 A single-arm phase IIIb clinical trial also indicated that HER2-targeted therapy and chemotherapy were well tolerated. 33 The blood-brain barrier can make brain tumors difficult to treat using pharmacological agents, although some monoclonal antibodies and chemotherapy drugs are reasonable options for patients with BM.7,34-36 Subgroup analysis in the present study revealed that the association between breast subtypes and mortality stably existed except in the case of primary surgery. Besides, the association was more significant in the chemotherapy group than non-chemotherapy participants (p for trend = .005). We hypothesized that a higher number of patients with multiple site metastases were included for HR–/HER2– subtype, and the risk of death due to side effects after chemotherapy was increased.
The present study has several strengths, including the relatively large population-based cohort, adjustment of the analyses for potential confounding factors, the subtype-specific analyses, and the finding that chemotherapy provided an OS benefit for patients with initial BM. However, the present study also has several limitations that must be considered when interpreting the results. First, the chemotherapy data were retrieved from the SEER database, which provides limited information regarding the specific chemotherapy regimen and its ability to cross the blood-brain barrier. Second, detailed information regarding radiotherapy could not be retrieved from the SEER database. Third, data regarding endocrine therapy could not be retrieved from the SEER database, and this treatment might attenuate the HR values for OS because it is positively correlated with OS. 37 Fourth, it is not possible to obtain information regarding the treatment of patients with BM, and the SEER database also has various other potential limitations that should be considered.
Conclusion
The present study evaluated SEER data regarding patients with BM at the initial diagnosis of breast cancer and indicates that the breast cancer subtype independently predicted the mortality of patients with brain metastasis at the initial diagnosis.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211055636 – Supplemental Material for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211055636 for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study by Dong-Jie He, De-Quan Yu, Qi-Ming Wang, Zong-Yan Yu, Yu-Hong Qi, Qiu-Ju Shao and Hao Chang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580211055636 – Supplemental Material for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study
Supplemental Material, sj-pdf-2-inq-10.1177_00469580211055636 for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study by Dong-Jie He, De-Quan Yu, Qi-Ming Wang, Zong-Yan Yu, Yu-Hong Qi, Qiu-Ju Shao and Hao Chang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-1-inq-10.1177_00469580211055636 – Supplemental Material for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study
Supplemental Material, sj-jpg-1-inq-10.1177_00469580211055636 for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study by Dong-Jie He, De-Quan Yu, Qi-Ming Wang, Zong-Yan Yu, Yu-Hong Qi, Qiu-Ju Shao and Hao Chang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-2-inq-10.1177_00469580211055636 – Supplemental Material for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study
Supplemental Material, sj-jpg-2-inq-10.1177_00469580211055636 for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study by Dong-Jie He, De-Quan Yu, Qi-Ming Wang, Zong-Yan Yu, Yu-Hong Qi, Qiu-Ju Shao and Hao Chang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-3-inq-10.1177_00469580211055636 – Supplemental Material for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study
Supplemental Material, sj-jpg-3-inq-10.1177_00469580211055636 for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study by Dong-Jie He, De-Quan Yu, Qi-Ming Wang, Zong-Yan Yu, Yu-Hong Qi, Qiu-Ju Shao and Hao Chang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-4-inq-10.1177_00469580211055636 – Supplemental Material for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study
Supplemental Material, sj-jpg-4-inq-10.1177_00469580211055636 for Breast Cancer Subtypes and Mortality of Breast Cancer Patients With Brain Metastasis at Diagnosis: A Population-Based Study by Dong-Jie He, De-Quan Yu, Qi-Ming Wang, Zong-Yan Yu, Yu-Hong Qi, Qiu-Ju Shao and Hao Chang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
Author Contributions
DJH and DQY analyzed the data and drafted the paper. QMW and ZYY collected the data, QMW and YHQ analyzed the data. QJS and HC conceived and designed the idea to this paper. All authors approved the final version for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
We signed SEER data-use agreements to access the data retrieved from this data-set. The retrospective study protocol was approved by the institutional review board at the Second Affiliated Hospital of Air Force Medical University (TDLL-KY-202103-02), which waived the requirement for informed consent based on the analysis of de-identified patient data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.