
Abstract
This retrospective study was undertaken to assess the correlation between click-evoked auditory brainstem responses and behavioral hearing tests. We recruited a total of 16646 infants born in Ditmanson Medical Foundation Chia-Yi Christian Hospital, Taiwan, from 2012 to 2018 for such assessment purpose. Their data including the click-evoked auditory brainstem response (ABR), referral, and diagnostic follow-up were collected. Spearman correlation method was employed to assess the relationship between ABR and pure-tone threshold. The correlation between the click-evoked ABR that met the National Health Administration standards and the click-evoked ABR derived from estimates before and after the 2.5 years of age effectively predicted the toddlers’ pure-tone audiometry (PTA) thresholds at 2–4 kHz.
Keywords
Introduction
The World Health Organization reported that approximately 466 million people had hearing loss in 2019, accounting for 6.1% of the world’s population. The population group included 432 million adults (93%) and 34 million children (7%).1,2 Congenital hearing loss is one of the most common diseases caused by various overlapping factors of children’s genetic susceptibility and environmental impact. The Hearing Loss Survey showed that in the general population, the prevalence of moderate and severe bilateral hearing impairments (>50 dB) is 2–3 cases per 1000 live births and 2–4 out of every 100 babies in the intensive care population.3,4 Tekin et al. 5 found the incidence of unilateral hearing loss and mild hearing loss is 4 per 1000 newborns. In Taiwan, the incidence of congenital hearing loss is approximately 2.6 per 1000 newborns. 6 In addition, Morton et al. reported that the prevalence of permanent bilateral hearing impairment is 1.33 per 1000 live births. 7
The National Institutes of Health consensus recommended universal newborn hearing screening (UNHS) to prevent sequelae of hearing loss in 1993. Several studies investigated the incidence and prevalence in accordance to the UNHS guidelines for UNHS. For example, Emma et al. reported prevalence of UNHS-detected congenital hearing loss in the screened population was 1.1 per 1000 children. 8 Therefore, the 2019 Joint Committee on Infant Hearing recommended screening before the infant is 1 month old, diagnosing hearing loss before the infant is 3 months old, and start intervention at 6 months old. 9 Screening programs for hearing impairment at birth may be either “universal” or “high risk” based on the population. No low-risk protocol exists. The high-risk population included a family history of hearing loss, craniofacial anomalies, birth weight <1500 g, hyperbilirubinemia, and congenital infections. 10 In some countries or regions, newborn hearing screening is only carried out in infants meeting the high-risk register (HRR) criteria; however, these programs only identified 50%–75% of infants with hearing loss and missed the rest.10,11 Choices of newborn screening tools can be otoacoustic transmission (OAE) or automatic auditory brainstem response (AABR). OAE can be divided into transient-evoked otoacoustic emissions (TEOAEs) and distortion-product otoacoustic emissions (DPOAEs). TEOAE is produced by the contribution distributed over a larger frequency region of the cochlea according to individual structural differences. However, analyzing specific cochlear frequencies is more difficult. DPOAEs appear to be produced in more specific areas of the cochlea, and the micromechanical properties of outer hair cells can be examined in frequency-specific areas. DPOAE can be measured in a wide frequency range, but when ≥4 kHz, their performance is better than TEOAE. 12 AABR is better than OAE, and weakness of OAE measurement is observed due to auditory neuropathy, which may result in missing lesions at the level of the inner hair cells (IHC), the auditory nerve, or the IHC/auditory nerve synapse. 13 Compared to AABR used to detect hearing impairment over 35 dB HL, click-evoked ABR could estimate the hearing threshold of patients in the frequency range of 1 k–4 kHz, especially in 2 kHz and 4 kHz. 14
The language ability of hearing-impaired children who start hearing intervention at the early stage is significantly better than those who start late. With appropriate early intervention, children with hearing loss can be mainstreamed into regular primary and secondary education classes.15,16 In addition, studies have shown that early detection of hearing loss with appropriate intervention can minimize extensive training during the school year.
17
However, auditory maturation in premature infants may affect long‐term hearing results. The auditory potential of the brainstem will not be completely mature until 2 years of age.
18
The auditory pathway shows morphological and physiological developments in the first few weeks of postpartum life. The main feature is that the synapse and myelination of nerve fibers begin to develop during the last stages of life in the uterus.
19
Delayed maturation of immature auditory pathways may be an important reason for referral after hearing screening in preterm infants. Hearing thresholds of preterm infants with hearing loss can change during the first year of corrected age, and normalization in 47% of newborns referred from UNHS was observed.
20
Besides preterm infants, hearing thresholds of full-term infants can change during the first year of life; therefore, the importance of administering follow-up hearing tests is emphasized.
21
• In the past decade, universal newborn hearing screening (UNHS) has been widely adopted in order to detect congenital hearing loss, and those newborns who do not pass the screening will be referred for further examinations. • In Taiwan’s hospitals, confirmatory tests for congenital hearing loss often use click-evoked ABR and otoacoustic emission (OAE) in 0–6-month-old infants. • Newborns with hearing loss confirmed by click-evoked ABR undergo regular behavioral audiometry and follow-up tests.
• The corresponding pure-tone audiometry thresholds in children referred from the universal newborn hearing screening (UNHS) were estimated. • A high linear positive correlation was observed between ABR threshold at 3 months and 6 months, behavioral thresholds at 2 kHz and 4 kHz, the average of 2 kHz and 4 kHz after 2.5 years old, and low to moderate correlations at 500 Hz and 1kHz.
• Click-evoked ABR may overestimate or underestimate the threshold of behavioral hearing tests. • Cautiously using ABR to estimate PTA in children referred from universal newborn hearing screening is important.
Therefore, this study aimed to investigate the current status of UNHS in Ditmanson Medical Foundation Chia-Yi Christian Hospital, Taiwan, and long-term follow-up of these children to determine the correlation between click-evoked ABR thresholds and behavioral PTA thresholds of hearing loss in children from the UNHS program.
Materials and Methods
Participants and Protocol for Universal Newborn Hearing Screening
In this retrospective study, a total of 16646 infants who were born in Ditmanson Medical Foundation Chia-Yi Christian Hospital, Taiwan, from 2012 to 2018 were included. All data including hearing screening, referral, and diagnostic follow-up rates were collected. We followed up these hearing loss newborns referred from UNHS until 2020. The following types of condition were excluded: (1) children with fluctuating hearing impairment and (2) conductive hearing loss (e.g., middle-ear diseases). Finally, a total of 60 newborns were included in this analysis. Among those newborns, there were 19 newborns with regular behavioral hearing assessment follow-up. Patients underwent behavioral hearing tests who were aged 1 to 5 years, using visual reinforcement audiometry (VRA) or conditional play audiometry (CPA).
Patients who failed the initial automatic ABR (AABR) neonatal hearing screening were referred to the otolaryngology department for follow-up click-evoked ABR objective hearing tests. Newborns with the click-evoked ABR threshold higher than 25 dB nHL were defined as failed hearing screening. All patients underwent AABR (AABR, Biologic ABaer) as the screening tool. Data including sex, sibling or twins, birth weight, and preterm birth or not (37 weeks) were obtained. Click-evoked ABR obtained at 1, 3, and 6 months old; VRA at <2.5 years old and CPA at >2.5 years old were recorded.
Audiometric Evaluation
Objective Tests Procedures
Auditory brainstem response was performed using Biologic Navigator Pro AEP (Natus Medical Inc., San Carlos, California, USA). We used ABR, ASSR, or both for diagnostic testing. The ABR test was performed using the Biologic Navigator Pro system (Natus Medical), and the click-type auditory stimulation was performed at a stimulation rate of 27.7 pulses/sec. The stimulation step is 10 dB with a contralateral mask. The EAR 3A dual earphone assembly is used as a transducer. The stimulation step is 10 dB with a contralateral mask. For air conduction, if absolute latencies of waves I and V are normal, masking is not required, whereas if they are abnormal, masking is needed. The following formula is used: The level of masking noise = the level click sound–interaural attenuation (IA) (insert earphone, 65 dB) + 10 dB.
Click-evoked ABR was obtained at 1, 3, and 6 months old. In ABR tests, an electrode is placed on each earlobe, 1 on the forehead and 1 on the top of the head. The skin is prepped with rubbing alcohol and a mild abrasive agent before placing the electrode. Sound is introduced into the ears using foam insert earphones placed in the ear canals. Electrical activity generated by the hearing nerve and brainstem pathways in response to a click sound is recorded with electrodes and fed into a computer where it is recorded. Then, audiologists will estimate the degree of hearing loss by finding the lowest intensity level where wave V is present and can be replicated.
Subjective Test Procedures
In the follow-up hearing tests, VRA was performed at the age of 1–2.5 years old. Audiometry (Grason-Stadler GSI61) was used to deliver sounds with insert earphones (foam tips) or sound-field speakers. Visual reinforcers, such as video animations or lighted toys, are placed 45° to each side of the patient to train the child to look toward the direction of the sound. A minimal response level was obtained. Alternating the high- and low-frequency sounds while starting with a higher frequency will yield an audiogram that provides information necessary to predict the contour of the hearing loss. The 2 kHz would be the starting frequency, followed by 500, 4 k, and then 1 kHz.
Conditional play audiometry was recorded at the age of 2.5–5 years old. CPA also used audiometry (Grason-Stadler GSI61) to test children’s hearing thresholds through headphones (TDH-50P). CPA is a “Listen and Drop” game that children are trained to perform an activity each time when they hear a sound. A 3- and 6-month follow-up is suggested for children with HL.
Statistical Analysis
Statistical analysis was performed using SPSS software (SPSS System version 21 for Windows) (version 21.0; IBM Corporation, Somers, NY, USA). The characteristic of babies who failed the screening are presented as number and percentage. The Spearman correlation was used to analyze the relationship between click ABR and behavioral PTA thresholds. P‐value < .05 was considered significant.
Results
Characteristics of Babies who Failed the Screening
Implementation Status of Universal Newborn Hearing Screening from 2012 to 2018.

Note. Data are presented as n.
Among the 97 failed newborns, one newborn with Down syndrome, 20 newborns who passed the hearing test 1 or 3 months after the examination, and 16 patients who were lost to follow-up were excluded. Finally, 60 newborns who failed UNHS are referred to ENT for comprehensive hearing test batteries, and 19 newborns (total 38 ears) with hearing loss confirmed by the click-evoked ABR test received behavioral auditory evaluation and follow-up (Figure1). Subject selection protocol.
Characteristics of the Subjects who Failed Screening (n = 80).
Characteristics of 19 Newborns (Total 38 Ears) With Hearing Loss Confirmed by the Click-Evoked ABR Test who Underwent Behavioral Auditory Evaluation.

Hearing Screening Rate, Referral, and Diagnosis Follow-Up Rate
Hearing Assessment Data for Chia-yi Christian Hospital from 2012 to 2018.

Relationship Between Click-Evoked Auditory Brainstem Response and Behavioral Thresholds
Relationship Between Click-Evoked Auditory Brainstem Response Thresholds and Behavioral Pure-Tone Average Thresholds.


Spearman correlation between click-evoked ABR thresholds (3 months) and behavioral audiometry thresholds at 500, 1 k, 2 k and 4 kHz before 2.5 years old.
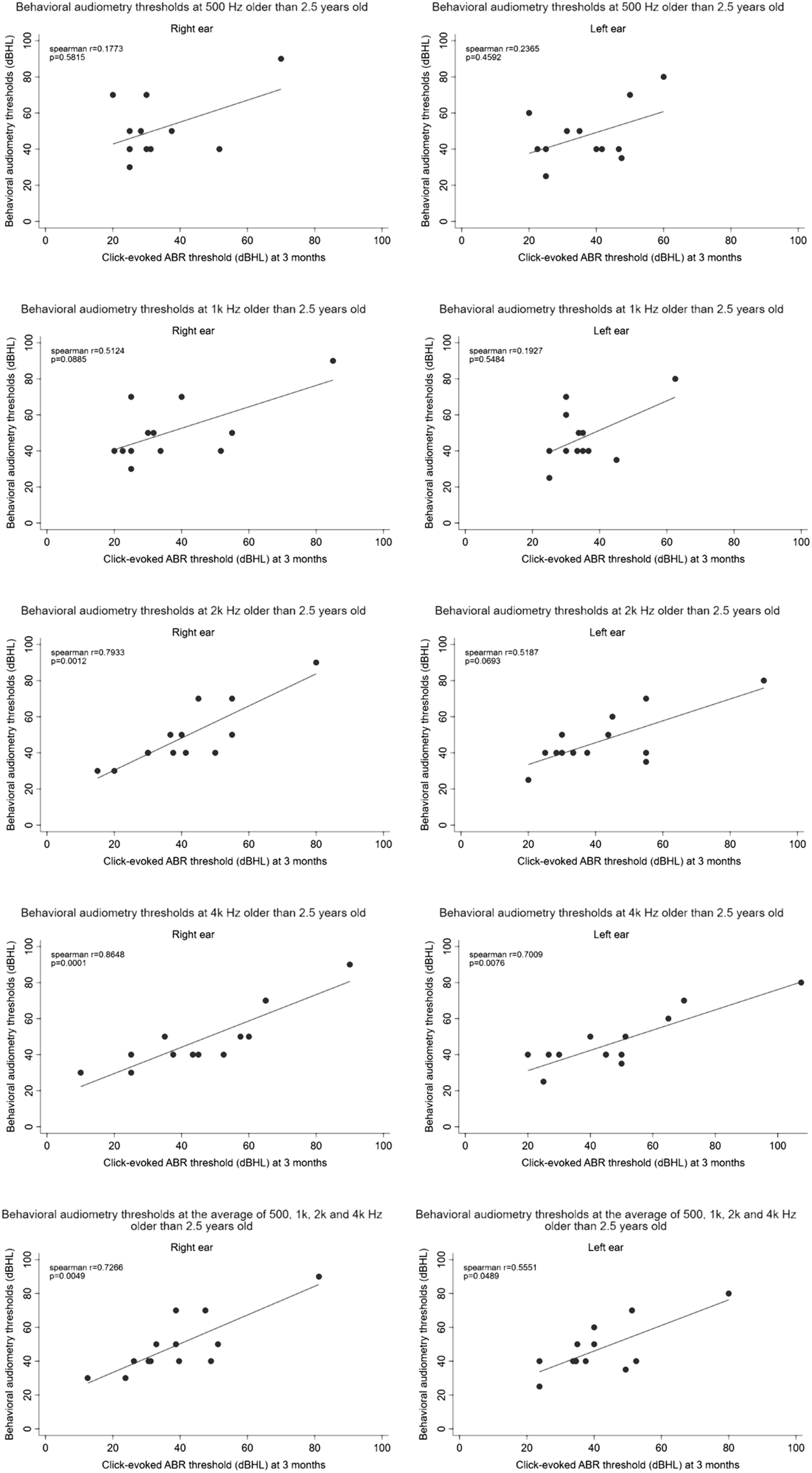
Spearman correlation between click-evoked ABR thresholds (3 months) and behavioral audiometry thresholds at 500, 1 k, 2 k and 4 kHz older than 2.5 years old.

Spearman correlation between click-evoked ABR thresholds (6 months) and behavioral audiometry thresholds at 500, 1 k, 2 k and 4 kHz before 2.5 years old.

Spearman correlation between click-evoked ABR thresholds (6 months) and behavioral audiometry thresholds at 500, 1 k, 2 k and 4 kHz older than 2.5 years old. Percentage of dB differences between click-evoked ABR and behavioral thresholds.
The similar patterns are also observed with moderate to high correlations between click-evoked ABR threshold at 6 months and behavioral thresholds at 500, 1 k, 2 k, and 4 kHz and the average of these 4 frequencies before 2.5 years old (Spearman r=.8154–.9856) (Figure 4). Moderate to high correlations (Spearman r = .6379–.8224) were observed at 2 kHz and 4 kHz after the age of 2.5 years, whereas low to moderate correlations (Spearman r = .2276–.5066) were observed at 500 Hz and 1 kHz after the age of 2.5 years (Figure 5).
The percentage of dB differences between click-evoked ABR at 3 months and behavioral thresholds at frequencies of 500, 1 k, 2 k, and 4 kHz and the average of these 4 frequencies was analyzed and plotted in Figures 6 and 7. In the right ear, percentages of mean accuracies between click-evoked ABR threshold at 3 months and behavioral thresholds at 500, 1 k, 2 k, and 4 kHz and the average of these 4 frequencies before 2.5 years old are 30.0% (±0–10 dB), 51.7% (±11–20 dB), and 18.3% (>20 dB), and the percentages of mean accuracies after 2.5 years old are 50.1% (±0–10 dB), 35.3% (±11–20 dB), and 14.6% (>20 dB), respectively. In the left ear, the percentage of mean accuracies between click-evoked ABR threshold at 3 months and behavioral thresholds at 500, 1 k, 2 k, and 4 kHz and the average of these 4 frequencies before 2.5 years old are 46.6% (±0–10 dB), 24.7% (±11–20 dB), and 29.0% (>20 dB), and percentages of mean accuracies after 2.5 years old are 50.5% (±0–10 dB), 42.9% (±11–20 dB), and 6.5% (>20 dB), respectively (Figure 6). Percentage differences in decibel levels between click-evoked auditory brainstem response thresholds at 3 months and behavioral thresholds at 500, 1 k, 2 k, and 4 kHz and their mean value. Percentage differences in decibel levels between click-evoked auditory brainstem response thresholds at 6 months and behavioral thresholds at 500, 1 k, 2 k, and 4 kHz and their mean value.

Figure 7 showed the percentage of dB differences between click-evoked ABR at 6 months and behavioral thresholds at frequencies of 500, 1 k, 2 k, and 4 kHz, and the average of these 4 frequencies.
Percentages of mean accuracies in the right ear before 2.5 years old are 76.0% (±0–10 dB), 16.7% (±11–20 dB), and 7.3% (>20 dB), and percentages of mean accuracies after 2.5 years old are 58.3% (±0–10 dB), 35.0% (±11–20 dB), and 6.7% (>20 dB). The percentage of mean accuracies in the left ear before 2.5 years old are 72.4% (±0–10 dB), 24.3% (±11–20 dB), and 3.3% (>20 dB), and percentages of mean accuracies after 2.5 years old are 65.0 (±0–10 dB), 23.3% (±11–20 dB), and 11.7% (>20 dB), respectively (Figure 7).
Discussion
In our study, the hearing screening rate was only 72% in 2012. After implementing the national government-funded UNHS program, the hearing screening rate reached 94% in 2013. Chang et al. reviewed that the hearing screening coverage rate reached 98.2%, the referral rate was 1.13%, the return rate of OPD referral was 86.10%, and the incidence of congenital deafness was approximately .445% in 2016. 22
Our result found that behavioral hearing tests of the right ear and the left ear at 500, 1 k, 2 k, and 4 kHz were highly correlated with click ABR at 3 and 6 months before 2.5 years of age. These results do not correspond with previous studies. In previous studies, they showed that click-evoked ABR thresholds and behavioral PTA thresholds showed a higher correlation at high frequencies than at low frequencies. The relationship between click-evoked ABR thresholds and behavioral PTA thresholds at frequencies of 500 and 1 kHz showed a moderate correlation, whereas that between click-evoked ABR thresholds and behavioral PTA thresholds at frequencies of 2 k and 4 kHz showed a high correlation. 23 Van et al. reported that the pure-tone threshold in the 2 k–4 kHz region has a one-on-one relationship with the ABR threshold. 24
Our results also showed the moderate to high correlation between behavioral hearing tests and click-evoked ABR at 3 months and 6 months at 2 k and 4 kHz (R range, .5187–.8648) after 2.5 years old. Similar data also published in previous studies showed the relationship between click-evoked ABR and behavioral hearing tests after growing up. 25 Several studies reported the correlation between click-evoked ABR and PTA (2 k–4 kHz) thresholds. Gorga et al. reported that there is a high correlation between evoked ABR and future behavioral threshold of 2–4 kHz on average (.94). 26 However, Bishara et al. reported a correlation coefficient of .68 27 and Stapells et al. reported a slope of .55. 28 These 2 studies revealed lower correlations than that observed in our results.
The percentages of mean accuracies between click-evoked ABR at 3 months and behavioral thresholds at 2.5 years old revealed similar results, that is, 50.1% (±0-10 dB), 35.3% (±11-20 dB), and 14.6% (>20 dB) in the right ears and 50.5% (±0–10 dB), 42.9% (±11–20 dB), and 6.5% (>20 dB) in left ears, respectively. Moreover, the percentages of mean accuracies between click-evoked ABR at 6 months and behavioral thresholds after 2.5 years old showed 58.3% (±0–10 dB), 35.0% (±11–20 dB), and 6.7% (>20 dB) in the right ear and 65.0 (±0–10 dB), 23.3% (±11–20 dB), and 11.7% (>20 dB) in the left ear. These results are similar to that of other studies. The percentage of differences between click-evoked ABR and PTA thresholds within 0–10 or 0–20 dB was 48.8% and 72.6%. 23 These results also reflected that behavioral PTA thresholds estimated from click-evoked ABR thresholds can be more likely an overestimation. Overestimation can be explained as the cochlea has matured before birth, but the auditory nervous system inside the cochlea is still developing; this may affect the interpretation of ABR waves, leading to overestimation of the ABR threshold induced by clicks. 29 Consequently, our study indicated that the cross-check principle would be necessary to improve hearing accuracy.
All newborns who fail the UNHS are referred to an otolaryngologist for complete further audiologic examinations including ABR, OAE, and 1000-Hz tympanogram. Hearing loss conducted binaurally and establishing its underlying cause might guide the therapeutic decision-making. Management options depend on the pathogenesis of hearing loss including surgical treatment of craniofacial abnormalities, specific antimicrobial therapies, and implantable or non-implantable hearing devices. 30 Many procedures have been performed to diagnose hearing-impaired infants. Various diagnostic tools, such as click ABR, tone burst ABR, OAE, and 1000-Hz tympanogram are used to diagnose hearing loss. Behavioral hearing tests include observation audiometry and VRA. Various tests such as auditory reflex examination, auditory steady-state-evoked response examination, and bone conduction ABR examination (bone conduction ABR) are used. 31
A biologic AABR as a screening instrument was used a 35 dB near hearing level click. AABR screener is a dedicated hearing screening device, which not only provides information about the outer/middle ear and cochlea but also provides the auditory pathway to the brainstem. Although OAEs are convenient and fast and instruments and consumables are cheaper than AABR, they are easily affected by the fetal fat of the external auditory canal of the newborn, which is likely to cause false positives. If the first hearing screening test fails, 80% of newborns will pass after the rescreening. The false-positive rate of the first hearing screening is <4%. During the second hearing screening, the false-positive rate is reduced from 3.9% to .8%. 32 AABR can detect the lesion of auditory brainstem. OAE may miss cases of auditory neuropathy.
The difference in related levels may be caused and explained by some limitations in this study. First, the correlation between click-evoked ABR and the type of hearing loss was not discussed in this study. Click-evoked ABR may overestimate the threshold of behavioral hearing tests and underestimate the threshold of sloping and progressive hearing loss and cannot effectively predict the threshold of U-shaped audiograms (medium-frequency impairment) or irregular audiograms. Therefore, some studies suggest that both click and tone burst ABRs should be used in children. 26 Second, although the screening rate reached 97%–98% in recent years, the diagnostic follow-up rate remained low because infants (1) are transferred to another hospital and (2) parents are unresponsive to treatment, (3) cannot be contacted, and (4) declined services. Our UNHS plan did not follow-up a few newborns, leading to potential selection bias. Third, the sample size of ear-specific thresholds is still small before 2.5 years old. When testing VRA, the audiologist replaces the headphones with earphones (usually with foam tips) or sound-field speakers. Insert earphones may be still uncomfortable for infants and toddlers. In some patients, the audiologist only relied on sound-field testing, which is not ear-specific. In this study, thresholds tested by sound-field speakers were not included and analyzed because this might lead to error values. For infants with unilateral hearing loss, the sound-field response is normal. However, it does not mean that the hearing in both ears is normal because the better ear helps to listen to the sound. A similar example also occurs in asymmetric hearing loss. The results also affected by children’s concentration because of low stability before 2.5 years old. The attention span in preschool children is 6–10 min for 2-year-olds; 9–15 min for 3-year-olds; 12–20 min for 4-year-olds; and 14 min for 5-year-olds. 33 Generally, the period of testing VRA is usually longer than 10–15 min, depending on children’s age in our research; therefore, the recorded threshold is often higher than the actual threshold. After 2.5 years of age, the stability of children becomes higher; thus, the test results will be closer to the results of click-evoked ABR.
Conclusion
In general, click-evoked ABR should be carefully used in predicting future thresholds. Although most studies point out that 2–4 kHz can be used to predict future behavioral examination results, only about half of our study population underwent click-evoked ABR and behavior testing showing dB number within 10 dB, and the other half is greater than 10 dB or even >20 dB. In this study, 500 and 1 kHz have lower correlations with click-evoked ABR in this group after 2.5 years of age. Thus, during UNHS follow-ups, frequency-specific tone burst ABR must be included in the infant hearing assessment to obtain a confirmatory diagnosis and to provide useful hearing threshold information for hearing aid fitting and auditory rehabilitation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was granted by Ditmanson Medical Foundation Chia-Yi Christian Hospital Institutional Review Board; protocol number: IRB2019094