
Abstract
Purpose
The study aimed to determine the impact of pharmacist-led interventions on diabetes management at a community pharmacy in Pakistan.
Methods
A one-month follow-up, randomized controlled trial (RCT) was carried out between December 1, 2016 and June 30, 2017. Sampling population consisted of patients diagnosed with type 2 diabetes mellitus (T2DM). The study population was randomized to a control group or an intervention group to determine the impact of a community pharmacist intervention on glycemic control fasting blood glucose (FBG) and random blood glucose (RBG), medication adherence (MMAS), and health-related quality of life (HRQoL) (EQ-5D-3L). Both non-pharmacological and pharmacological interventional tools were used that consist of array of charts and verbal communication by pharmacist. Outcomes for continuous variables were analyzed using paired sample t-test for time effect and one sample t-test to evaluate the study group effect. Independent sample t-test was used to compare each independent variable with dependent variable. A P-value of <.05 was considered statistically significant.
Results
The control and intervention groups showed significant improvement (P-value < .05) in glycemic control, medication adherence, and HRQoL. However, the difference between the control and intervention groups was not statistically significant in terms of blood glucose levels and HRQoL (time trade off, TTO). There was a clinically significant association between pharmacist intervention and predefined glycemic control among the study participants (FBG: P-value < .001 and RBG: P-value = .04). A clinically significant association was also found between pharmacist intervention and medication adherence at the end of the trial compared with baseline values (P-value < .001). Similarly, a clinically significant association was found between pharmacist intervention and predefined HRQoL [TTO: P-value = .002 and EQ-VAS: P-value = .001].
Conclusion
A significant proportion of T2DM patients in the intervention group achieved predefined glycemic control, medication adherence, and health related quality of life.
Keywords
Answer: In the developed countries, community pharmacists assist diabetes patients to effectively manage their disease and its associated complications. However, such roles of pharmacists have not been fully explored in the developing countries, for example, Pakistan.
Answer: This randomized controlled trial (RCT) is among the very few studies from the developing countries, and probably the first from Pakistan which has evidenced the value-added role of community pharmacists in diabetes management.
Answer: The findings of this RCT necessitate the mandatory presence of skilled pharmacists in community pharmacies of Pakistan. This will not only decrease the burden of communicable and non-communicable diseases on the healthcare system, but also improve the overall health of the people.
Introduction
As per the global survey conducted by the International Diabetes Federation (IDF), the prevalence of diabetes in 2017 was 425 million and is expected to rise to 629 million by 2045. Additionally, four out of five patients with diabetes live in low- and middle-income countries, and nearly half of the diabetic patients remain undiagnosed. In Pakistan, around 6.9% of the adult population suffers from diabetes, rising to 8.5% by 2045. 1 Complications are considerable in numbers which demand ongoing management of diabetic patients.
Diabetes management demands multiple self-care behaviors by patients such as dietary modification, physical activity and weight reduction, adherence to medicines, and constant monitoring of glycemic levels. 2 This disease can be alleviated by a multidisciplinary team comprising physicians, pharmacists, nurses, and dieticians who have expertise in education and management of diabetics. 3 The American Diabetes Association (ADA) highlights that registered pharmacists are integral members of the multidisciplinary team caring for diabetics. 4 Studies from Australia 5 and the United Kingdom 6 report that community pharmacist activity results in significant improvement in outcomes of type 2 diabetes mellitus (T2DM) patients. However, the literature is scarce which supports this activity in developing nations, including Pakistan.
The majority of patients in Pakistan visit public and private sector hospitals for the seeking of management of diabetes. Some of the factors responsible for delayed diagnosis and improper management of diabetes include this excessive workload of physicians, inadequate number of diagnostic centers, dearth of government-funded health care settings (relative to the population of the country), lack of personal support, limited number of specialized pharmacists and dieticians, and insufficient time given by family physicians for disease-related counseling. 7 Community pharmacists are uniquely positioned to provide diabetes care, often being “the first port of call” for managing chronic diseases such as diabetes. 8 Access to community pharmacy services is often good and people feel satisfied due to short waiting times, ease of location, free advice, and extended opening hours. 9 A study related to management of insomnia, acute respiratory tract infection, and diarrhea has been conducted in community pharmacy in Pakistan which shows the potential impact of pharmacist-led interventions. 10 However, despite the significant burden of diabetes in Pakistan, the authors are not aware of community pharmacist role in diabetes care.
Aim of the Study
The aim is to determine the impact of pharmacist-led interventions on glycemic levels, medication adherence, and quality of life for Pakistani people with diabetes attending a community pharmacy-based service.
Methods
Study Setting
The study was conducted at a community pharmacy (Pharmacy X) located in Bahawalpur, Punjab province of Pakistan. There are almost 400 pharmacies and medical stores registered in Bahawalpur. Pharmacy X is the first community pharmacy in Bahawalpur supervised by two full time community pharmacists, with a purpose built counseling area for patients.
Study Design and Sampling
An interventional study based on RCT methodology was implemented. The sample consisted of patients diagnosed by registered medical practitioners with T2DM (ie, patients with HbA1c level of 6.5% or higher; as proposed by ADA
11
) for one year. The sample was divided into two groups (ie, control group and interventional group) to determine the impact of the community pharmacist intervention on glycemic control, medication adherence, and quality of life. The context is important to the study–the control group received routine medications and no specific intervention was applied. This is usual practice because patients often do not ask pharmacy staff to educate them as there is absence of pharmacists at most of pharmacies/medical stores. In Pakistan, pharmacists generally do not offer proactive advice. Many pharmacies do not contain a pharmacist. As such, patients in the control group were only educated based on the questions raised by them (if any). This is considered “routine care”. On the other hand, the intervention group received interventions relating to quality of life, medication adherence, and glycemic control. The process of randomization along with study inclusion and exclusion criteria is outlined in Figure 1. Sample size was determined by using an online sample size calculator. The sample size was calculated based on effect size of .5 mg/dl for FBG (SD = 1.3). Power of statistical tests was set at 80% with .05 level of significance. Based on an attrition rate of 20%, at least 80 patients were required in each study group.
12
Process of randomization along with study inclusion and exclusion criteria.
Data Collection
Data were collected from December 1, 2016 to June 30, 2017. Persons with diabetes visiting the community Pharmacy X had the study explained to them and were asked for their consent to participate. A total of 200 patients with diagnosed T2DM were registered in the trial at baseline; 100 in each group. After the initial assessment, the patients were interviewed to complete a number of questionnaires based on data required to answer the objectives of the study (Figure 2). Process of data collection for control and intervention groups.
Data Collection Tools and Outcome Variables
Glycemic control was the primary clinical outcome measure, and others included medication adherence and quality of life.
Glycemic control
Glycemic levels were considered normal when blood glucose levels were within predefined ranges as suggested by ADA [fasting blood glucose (FBG) 80–130 mg/dL and random blood glucose (RBG) <180 mg/dL]. 13 These were measured in both groups by using an Accu-Check Performa meter at baseline and after one month (a valid household point-of-care device based on a strip method with the accuracy of ±5% to ±15% dependent upon glucose concentration equal to or greater than 100 mg/dL to 600 mg/dL). 14 Glycemic levels were measured at each visit.
Medication adherence
The Morisky Medication Adherence Scale (MMAS-8), a validated tool based on eight closed-ended questions (Yes = 0, No = 1), was used to evaluate patients’ adherence to their medicine regimes. This validated tool has been used in a study focusing on medication adherence among persons with diabetes.
15
Data were collected at baseline and after completion of one month of enrollment in the study by interviewing the patients in both groups. Reverse coding was used for item number 5 in a positive direction (Yes = 0, No = 1). The last item (Item 8) was scored using a Likert-scale 0–4 (never/rarely = 4, once in a while = 3, sometimes = 2, usually = 1, and all the time = 0), and the scores were categorized as follows; • If Item 8 = 4, Item 8r = 1.00 (highest adherence). • If Item 8 = 3, Item 8r = .75 (high adherence). • If Item 8 = 2, Item 8r = .50 (moderate adherence). • If Item 8 = 1, Item 8r = .25 (low adherence). • If Item 8 = 0, Item 8r = .00 (lowest adherence).
The total score of MMAS-8 ranged from 0–8 and was categorized into three levels of adherence • Low adherence = < 6. • Medium adherence = 6 to <8. • High Adherence = 8.
The permission to use the Urdu version of MMAS was obtained from its developers. 16
Health-Related Quality of Life
The health-related quality of life (HRQoL) was assessed by using EuroQol 5-D three levels (EQ-5D-3L) scale. 17 This validated tool has been used widely in multiple studies focusing on HRQoL among diabetics.5,6 It consists of two components; one of which is a descriptive scale that includes five dimensions (mobility, self-care, usual activities, pain, and anxiety) with each having three levels of assessment (no problems, some problems, and extreme problems). The second component is based on an EQ visual analogue scale (EQ VAS) that records the self-rated quality of life of patients on a visual analogue scale (0–1) and is useful for measuring patient responses to their health status. Data were collected through interviews using the Urdu version (national language of Pakistan) of the EQ-5D-3L scale. The permission to use the Urdu version of EQ-5D-3L was obtained from its developers. 18
Intervention Tools
Both non-pharmacological and pharmacological interventional tools were used by the community pharmacist to help patients understand the appropriate management of their diabetes. These interventions were based on an array of charts (with pictorial representation) and verbal communication. Charts included diet, foot care, symptoms of hypoglycemia and hyperglycemia, and how to administer insulin (see the appendix in the electronic supplementary material). All of these charts were supplied by the Novo Nordisk (pharmaceutical company) and approved by the Ministry of National Health Services Regulation & Coordination of Pakistan. 19 Importance of exercise, time to take medications, frequency of medication dosage, and other medicines-related information were imparted. The intervention was delivered to individual patients at their baseline visit. Cross questioning was undertaken with patients during the consultation to ensure that they fully understood the meaning, as posed. The pharmacological intervention was based on adjustment of dose frequency of insulin and oral diabetic medicines only in the case when it was not according to standard 20 and method of insulin administration. These pharmacological interventions are sanctioned as a role of the community pharmacist in accordance with the DRAP Act 2012. 21
Statistical Analysis
The data were analyzed by using Statistical Package for Social Sciences (IBM, SPSS Statistics for windows, version 20). In order to summarize data, descriptive statistics (mean and standard deviation/standard error (SD/SE) or median (IQR) for continuous data and frequency and percentage for categorical data) were applied. Outcomes for continuous variables were analyzed using paired sample t-test to study the effect within each study group at Tone month vs T baseline (time effect) and one sample t-test to evaluate the study group effect (ie, mean change from baseline in the intervention group vs mean change from baseline in the control group [intervention effect]). Chi-square test was used for analysis of categorical variables for investigating the intervention effect. Independent sample t-test was used to compare each independent variable with dependent variable. A P-value of <.05 was considered statistically significant.
Ethics Approval
Ethics approval was obtained from the Pharmacy Research Ethics Committee (PREC) at Islamia University of Bahawalpur (Reference number of 43-2016/PREC). The purpose of study was explained to each participant before gaining consent and conducting the study. A de-identifying code number was assigned to each participant to keep their identity confidential. Participation in the study was voluntary, and patients were informed that they could withdraw at any time. This study is registered under clinical trial protocol number ISRCTN10671625 with ISRCTN registry.
Results
Patient Characteristics
Socio-demographic and clinical characteristics and adherence level of the respondents in control and intervention groups.

Over sixty percent of the patients in the control (n = 50, 62.5%) and intervention groups (n = 48, 60%) had a negative family history of diabetes. Over three-quarters of the patients in the control (n = 57, 76.3%) and intervention groups (n = 63, 78.8%) had diabetes for a period of less than 10 years (Table 1).
Glycemic Control
Glycemic control, medication adherence, and health-related quality of life in control and intervention groups.
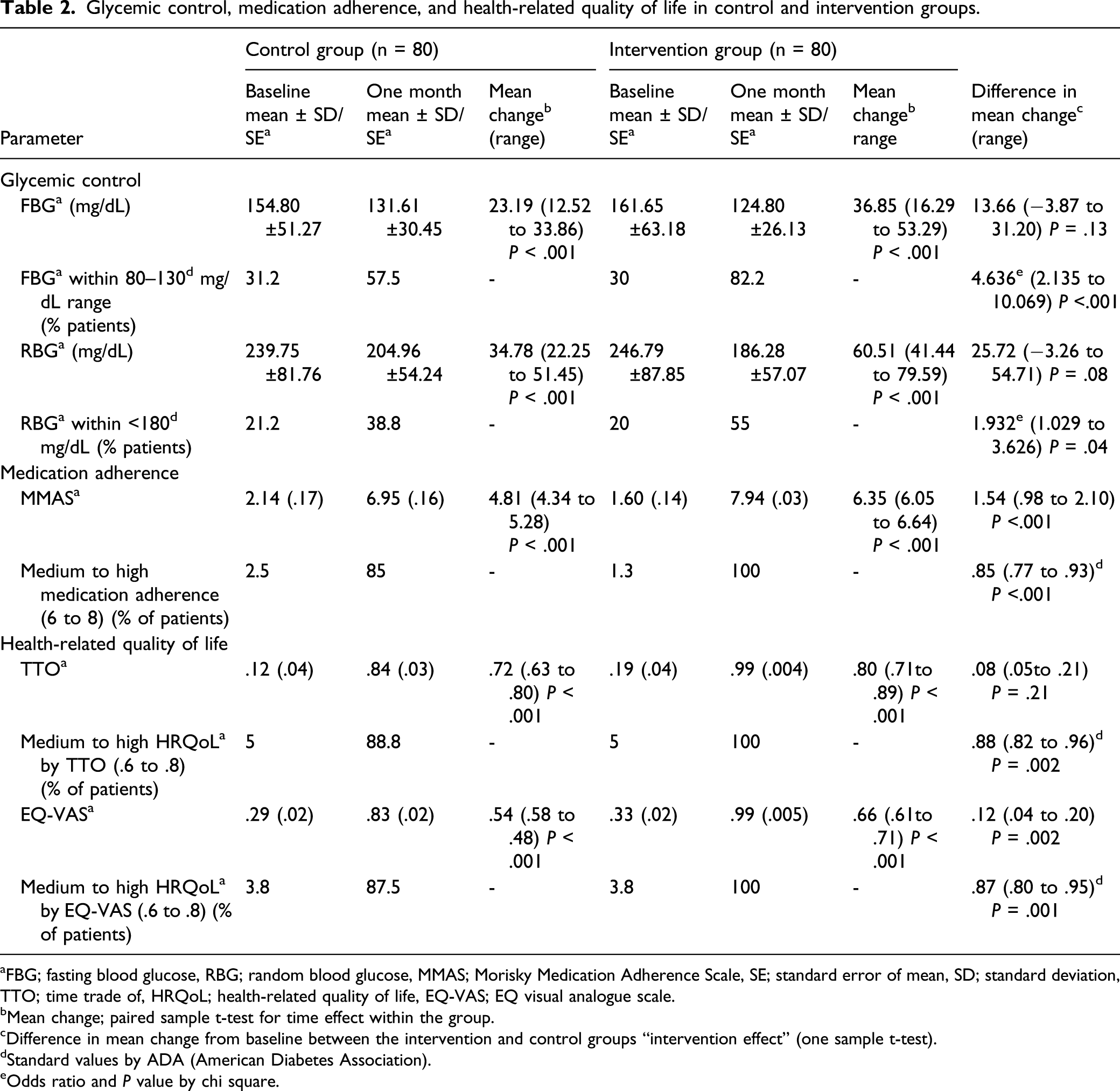
aFBG; fasting blood glucose, RBG; random blood glucose, MMAS; Morisky Medication Adherence Scale, SE; standard error of mean, SD; standard deviation, TTO; time trade of, HRQoL; health-related quality of life, EQ-VAS; EQ visual analogue scale.
bMean change; paired sample t-test for time effect within the group.
cDifference in mean change from baseline between the intervention and control groups “intervention effect” (one sample t-test).
dStandard values by ADA (American Diabetes Association).
eOdds ratio and P value by chi square.
Medication Adherence
MMAS was administered to both groups at baseline and after one month (Table 2). The response to medication adherence questions in the control and intervention groups is presented in Supplementary Table S3 (supplementary file).
A high level of self-reported medication adherence was seen in the intervention group (95%) as compared to the control group (46%) after the completion of one month of the trial (Table 1). Most of the patients showed significant improvement in medication adherence in both groups of the study (Supplementary Table S4 in the electronic supplementary material for details).
Both study groups demonstrate significant improvement (P-value < .0001) in medication adherence at the end of the study period as compared with baseline (time effect). A clinically significant association (percentage of patients who have medium to high medication adherence scores, that is, 6 to 8) was also found between the pharmacist intervention and medication adherence at the end of the trial from baseline values (control group 4.8 [P-value < .001] and the intervention group 6.35 [P-value < .001]) (Table 2).
Health-Related Quality of Life
Health-related quality of life was assessed through time trade off (TTO) score and EQ-VAS score in both study groups at baseline and after one month. Response of the participants to health-related quality of life items in the control and intervention groups is provided in Supplementary Table S5 (supplementary file).
Similar patterns of improvement were seen in health-related quality of life across all study variables in both groups. Comparison of TTO with each independent variable in both groups at baseline and after one month is outlined in Supplementary Table S6 in the electronic supplementary material. A comparison of EQ-VAS with each independent variable in both groups at baseline and after one month is outlined in Supplementary Table S7 in the electronic supplementary material. Both study groups showed significant improvement in TTO and EQ-VAS scores after one month. A clinically significant association (percentage of patients who have medium to high HRQoL by TTO, that is, from .6 to .8, and who have medium to high HRQoL by EQ-VAS, that is,, from .6 to .8) was found between the pharmacist intervention and predefined health-related quality of life (TTO: P-value .002 and EQ-VAS: P-value = .001) (Table 2).
Discussion
This study set out to understand the impact of pharmacist-led interventions on diabetes management in a community pharmacy in Punjab province, Pakistan. Our findings indicate that the control and intervention groups showed significant improvements in glycemic control, medication adherence, and HRQoL. However, statistically a non-significant difference was found between the control and intervention groups in terms of blood glucose level and HRQoL (TTO). There was however a clinically significant association between pharmacist interventions and predefined glycemic control, medication adherence, as well as predefined health-related quality of life scores.
The initial step for managing diabetes is to understand the relationship between the disease and study patient characteristics. In line with another study, participants were male and >50 years. 5 A study has reported that sedentary lifestyle, genetic factors, and poor eating behaviors among males make them more prone to diabetes. 22 In the current study, the majority of patients were married and unemployed and study conducted in Jordan aligns with this. 23
Treating hyperglycemia is one of the major goals for T2DM since effective glycemic control reduces complication risk. In this study, a clinically significant association was found between pharmacist intervention and predefined glycemic control (FBG and RBG). This finding is not surprising since pharmacist interventions included both non-pharmacological diabetes education and pharmacological interventions. It cannot be determined which components of the intervention result in improved glycemic control; however, it is assumed that the combinations of non-pharmacological and pharmacological components yield an additive effect on glycemic control. The study has shown a significant reduction in FBG levels in patients who receive a care plan from a pharmacist, compared to usual care. 24 The majority of independent variables showed similar patterns of reduction in FBG and RBG levels between the two groups. This is in line with the findings of a Spanish study which also demonstrated a lack of statistical difference across the independent variables. 25 However, future studies must be conducted to validate the relationship between independent variables and glycemic control. Improvement in glycemic levels in the control group may be attributed to the increased vigilance toward self-care after being enrolled in the study and thus better outcomes.
Optimal medication adherence is crucial for achieving the clinical outcomes desired in diabetics. Effective adherence demands the scheduling of management processes, refinement according to medication schedule changes, planning to ensure the availability of medicines, considering past events, and solving problems pertaining to missed/late doses. 26 A study highlights that assessing medication adherence is a core responsibility of pharmacists, 27 and the current study demonstrates a clinically significant association between the pharmacist intervention and medication adherence between start and end of the trial. A study has found that pharmacist interventions lead to improved medication adherence among patients. 23 Although a relatively new concept in Pakistan, considerable literature from the developed world suggests that pharmacists are uniquely positioned to educate patients on the importance of medication adherence. 28 In line with the findings of Tabasi et al, 29 the current study demonstrates increased medication adherence among married patients. Family support leads to decreased stress, more positive health behaviors, and increased adherence to medicines resulting in improved clinical outcomes. 29
The EuroQol EQ-5D scale has been utilized for the assessment of HRQoL among persons with diabetes, and assessment of HRQoL comes under the scope of pharmacy practice. 30 Involvements of the community pharmacist in this domain lead to positive effects on patients’ HRQoL across all five domains in all patients in the intervention group. This finding aligns with a Danish study. 31 Imparting diseased state knowledge, modification in lifestyle, and increased adherence with medicines through community pharmacist activity lead to improved HRQoL, which in turn is positively related to improved glycemic control.5,6 Despite this current practice is limited, this study further supports the opportunities pharmacists have in Pakistan.
As with any study, there are limitations to this one. First, the study is of short duration using random and fasting blood glucose testing, whereas it demands long-term follow-up taking up to three months to stabilize post intervention, as suggested by HBA1c testing. It is possible that a longer follow-up period with HBA1c testing would have resulted in larger detectable differences between the groups. However, time restraints and funds did not allow for a larger patient population or follow-up period. Second, the role of community pharmacist as a drug therapy manager, medication reviewer, and provider of information related to ADRs and DDIs was not explored. Moreover, the impact of pharmacist–physician relationship on the management of the diabetes was not included. These aspects could be addressed in future studies.
This study concluded that interventions by community pharmacists resulted in better management of diabetes and involvement of community pharmacists could help to manage diabetes, thus simultaneously sharing the burden on physicians while improving outcomes for patients.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-2-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-3-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-3-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-4-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-4-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-5-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-5-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-6-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-6-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-7-inq-10.1177_00469580211036283 – Supplemental Material for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial
Supplemental Material, sj-pdf-7-inq-10.1177_00469580211036283 for Impact of Pharmacist-Led Interventions on Diabetes Management at a Community Pharmacy in Pakistan: A Randomized Controlled Trial by Muhammad Abubakar and Muhammad Atif in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
This study was conducted at the Islamia University of Bahawalpur by the MPhil research candidate (Muhammad Abubakar). We would like to thank the proprietor of the community pharmacy in Bahawalpur for providing adequate space and facilities to conduct this study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.