
Abstract
This study aimed to investigate factors affecting blood glucose control among middle-aged and older diabetic patients taking medications or receiving insulin therapy. In 2015–2017 data obtained from the Korean National Health and Nutrition Examination Survey (KNHANES), 1257 patients with diabetes were divided into a controlled group and an uncontrolled group based on blood glucose levels (cutoff ≥126 mg/dL). After adjusting for confounding factors, the BMI, total cholesterol level, and triglycerides level of the uncontrolled group were significantly higher than the controlled group. The total amount of moderate-intensity activity in controlled patients was significantly higher than that of the controlled group. Total energy, fat, saturated fatty acids, and cholesterol intakes were found to be significantly higher in the uncontrolled than controlled group. Intakes of calcium, phosphorus, potassium, riboflavin, niacin, and vitamin C were significantly lower in the uncontrolled than controlled group. Adequate nutrition intake and physical activity of patients undergoing diabetes therapy are required for effective blood glucose management for both diabetic drug and insulin therapies.
Highlights
* What do we already know about this topic? It is important to identify factors affecting blood glucose control among middle-aged diabetic patients taking diabetes medication or insulin therapy. * How does your research contribute to the field? Our investigation provided evidence of a relationship between moderate-intensity activity time, nutrient intake, and blood glucose control in diabetes patients taking medications or receiving insulin therapy. * What are your research’s implications toward theory, practice, or policy? Clinicians should emphasize that changes in body composition affected by physical activity and adequate daily nutrient intake are crucial elements of diabetes management in middle-aged elderly patients.
Introduction
According to the 2018 Korean National Health and Nutrition Examination Survey (KNHANES), the prevalence of diabetes (adults, ≥30 years) is 12.9% in men and 7.9% in women; the diabetes cognitive rate was 71.5%, treatment rate was 66.2%, disease control rate was 31.1%, and treatment rate was 25.8% (for those over 30 years old). 1 Thus, the scale of diabetes treatment has continuously increased, but the diabetes control rate is lower than other chronic diseases in Korea. There are several possible contributors to poor glucose control among middle-aged and older adults, including misdiagnoses, inadequate treatment adherence, and lifestyle factors. 2 Glycemic control according to age group showed that optimal glycemic control was more prevalent among older individuals compared to younger individuals. 3 Another previous study demonstrated that individuals who had suffered diabetes for more than 10 years had a greater probability of glycemic control by 55% compared to those with diabetes for 10 years or less (OR = 1.55, p < .05). 4 Therefore, it is important to identify factors affecting blood glucose control among middle-aged diabetic patients.
Well-known risk factors for diabetes include unfavorable dietary intake, obesity, and biological determinants. 5 A recent study found unfavorable fat or carbohydrate intake to be associated with an increased incidence of type 2 diabetes mellitus among Korean adults. 6 The obesity rate among Koreans with diabetes is over 50%. 7 Therefore, to manage diabetes, controlling blood glucose levels using a combination of pharmacotherapy and lifestyle changes, such as weight control and diet modifications, is crucial.8,9 The American Diabetes Association now recommends that patients with type 2 diabetes engage in aerobic exercise of moderate intensity (50% to 70% of maximal heart rate) at least 3 days a week and resistance exercise at least twice a week. 10 In Korea, a study found that combined low- and moderate-intensity aerobic exercise, such as walking for 30 minutes or more five times a week, is likely to improve glycemic control (HbA1c concentration below 6.5%) and thus prevent the acute and chronic complications of type 2 diabetes mellitus among people aged 30 to 90 years. 11 Therefore, it is important to investigate the effects of physical activity of varying frequency, duration, and intensity levels on blood glucose control among middle-aged and older diabetic patients.
In the United States of America, given that the majority of persons with type 2 diabetes are overweight or obese, weight loss through nutritional therapy is often a first step in controlling the onset or progression of diabetes. 12 The appropriate consumption of daily nutrients aids in weight loss or weight management and may improve the regulation rates of therapeutic agents that are needed to control diabetes. In addition, the correct diet may help in improving psychological health such that a patient might be encouraged to effectively manage their diabetes. 13 The American Diabetes Association recommends that patients undergoing diabetic therapy follow the dietary guidelines for the general population as set out by the Dietary Guidelines for Americans. 14 A national cross-sectional study conducted between 2005 and 2010 indicated that men and women diagnosed with diabetes consumed more protein than their counterparts with undiagnosed diabetes; however, all participants consumed less fiber and more saturated fat than recommended. 15 In United States of America, according to 1988–2004 NHANES data, about two-thirds of adults with type 2 diabetes consumed more fat and saturated fat than recommended, 16 and the total energy consumption of patients aged 45–64 years increased over time. 17
In Korea, previous studies have also been performed to determine health-related lifestyles that influence glycemic control for diabetes mellitus management strategies. However, few studies have focused on the anthropometric status, physical activity, and nutritional intake of patients undergoing diabetic therapy in terms of adequate vs poor glucose control. Therefore, the present study investigated the body compositions, blood biochemistry profiles, physical activity, and nutrient intake of middle-aged and older patients on diabetes treatment and compared patients with good vs poor control of blood glucose levels.
Methods
Data Source and Subjects
This study is based on data from the 2015–2017 KNHANES (sixth–seventh), a cross-sectional, national survey conducted by the Korean Ministry of Health and Welfare. The KNHANES sixth–seventh vetted survey subjects using a stratified and multistage probability model designed to represent individuals over the age of one living in Korea. The survey comprised three parts: the collection of sociodemographic, health, and nutritional data through distinct surveys. 18 The Institutional Review Board (IRB) of the Korea Centers for Disease Control reviews and approves the KNHANES survey annually. The present study design was approved by the IRB of the Korean Ministry of Health and Welfare (IRB number: P01-202003-21-004).
The 2015–2017 KNHANES included 23 657 subjects; in the present study, subjects were excluded if they did not have diabetes or had missing data regarding diabetes or diabetes therapy. Furthermore, subjects were excluded if they were younger than 45 years, were pregnant, or had a daily calorie intake below 500 kcal or over 5000 kcal. The study cohort consisted of 1257 middle-aged and older patients who were diagnosed with diabetes. Subjects with diabetes were defined as those who responded “Yes” to the question “Have you been diagnosed with diabetes by a doctor at a hospital?” in the health interview survey; subjects who responded “No” were considered to not have diabetes, and subjects who responded “Not applicable” were excluded from the study. Moreover, subjects were excluded if they were not taking diabetes medication or insulin. Glucose control was classified according to blood glucose cutoff of 126 mg/dL; subjects with diabetes were categorized as either controlled or uncontrolled depending on whether their most recent fasting blood glucose measurement was below or above this threshold, respectively (Figure 1). Flowchart of study population.
Variables and Measurements
Sociodemographic characteristics such as age, sex, education level, and marital status were obtained from the health interview survey. Obesity was defined as a BMI (calculated as kg/m2) of ≥25 kg/m2, which is the cutoff for adults in the Asian and Pacific regions. 19 Systolic and diastolic blood pressure values were measured after a resting period. Blood samples were collected from the antecubital vein after an 8 h fast. Total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), and fasting blood glucose levels were measured using an enzymatic method (Hitachi Automatic Analyzer 7600, Hitachi, Japan).
Physical activity categories included walking, moderate-intensity exercise, and activity exerted while commuting. Physical activity indicators were taken from the KNHANES health behavior survey items. Since the study subjects were people over 45 years of age who were currently taking diabetes medication or insulin, the exercise categories were moderate-intensity physical activity (work and leisure time) and location-moving physical activity, excluding high-intensity physical activity indicators. Moderate-intensity physical activity during working hours included walking briskly while performing work activities, including paid work, unpaid work, schooling and education, household chores, farming, fishing, ranching, or job-seeking; its definition included carrying light objects, cleaning, and child-rearing (bathing, carrying a child, etc.). Moderate-intensity physical activity in leisure time included moderate-intensity sports, exercise, and leisure activities in which subjects would invariably become slightly short of breath or have a slightly raised heart rate for at least 10 minutes, such as brisk walking, light jogging (jogging), or weight training (strengthening exercises). Physical activity during commuting was defined as going to work, walking for more than 10 minutes, or using a bicycle; the definition also included the exertion involved in shopping, going to worship, among other activities.
Diet and food intake were assessed using a one-day 24 h recall method in the KNHANES. The dietary questionnaire was administered during face-to-face interviews in which information concerning the type, amount, and frequency of foods and drinks consumed during the previous day was solicited.
Statistical Analysis
Korean National Health and Nutrition Examination Survey data from the Korea National Statistical Office were used to define the standard population. We used the presets of stratified random sampling (kstrata), population sampling (psu), weighted samples (wt_itvex), and performed complex sample analysis in SPSS Statistics for Windows, version 23.0 (IBM Corp, Armonk, NY, USA). Descriptive statistics for the health interview survey, health examination survey, and nutrition survey were generated in which frequencies and percentages were calculated for categorical variables, and means and standard errors were calculated for continuous variables. To determine whether differences in general characteristics, physical activity levels, anthropometric data, biochemical data, and nutrient intake existed between the controlled and uncontrolled blood glucose groups, we used the chi-square test for categorical variables (general characteristics and physical activity type) and linear regression modeling for continuous variables (physical activity time, anthropometric data, biochemical data, and nutrient intake). General linear models in complex sample analysis were used to compare the two groups (controlled and uncontrolled) according to the anthropometric and biochemical parameters, and physical activities and nutrient intake among the diabetic patients that used diabetes drugs or insulin therapy were measured after adjusting for model 1: adjusted for gender and age and model 2: adjusted for gender, age, residential area, educational level, household income level, employment status, smoking status, current alcohol consumption, obesity, hypertension, dyslipidemia, and total energy intake. Statistical significance for all analyses was set at p < .05.
Results
General characteristics of diabetes patients.
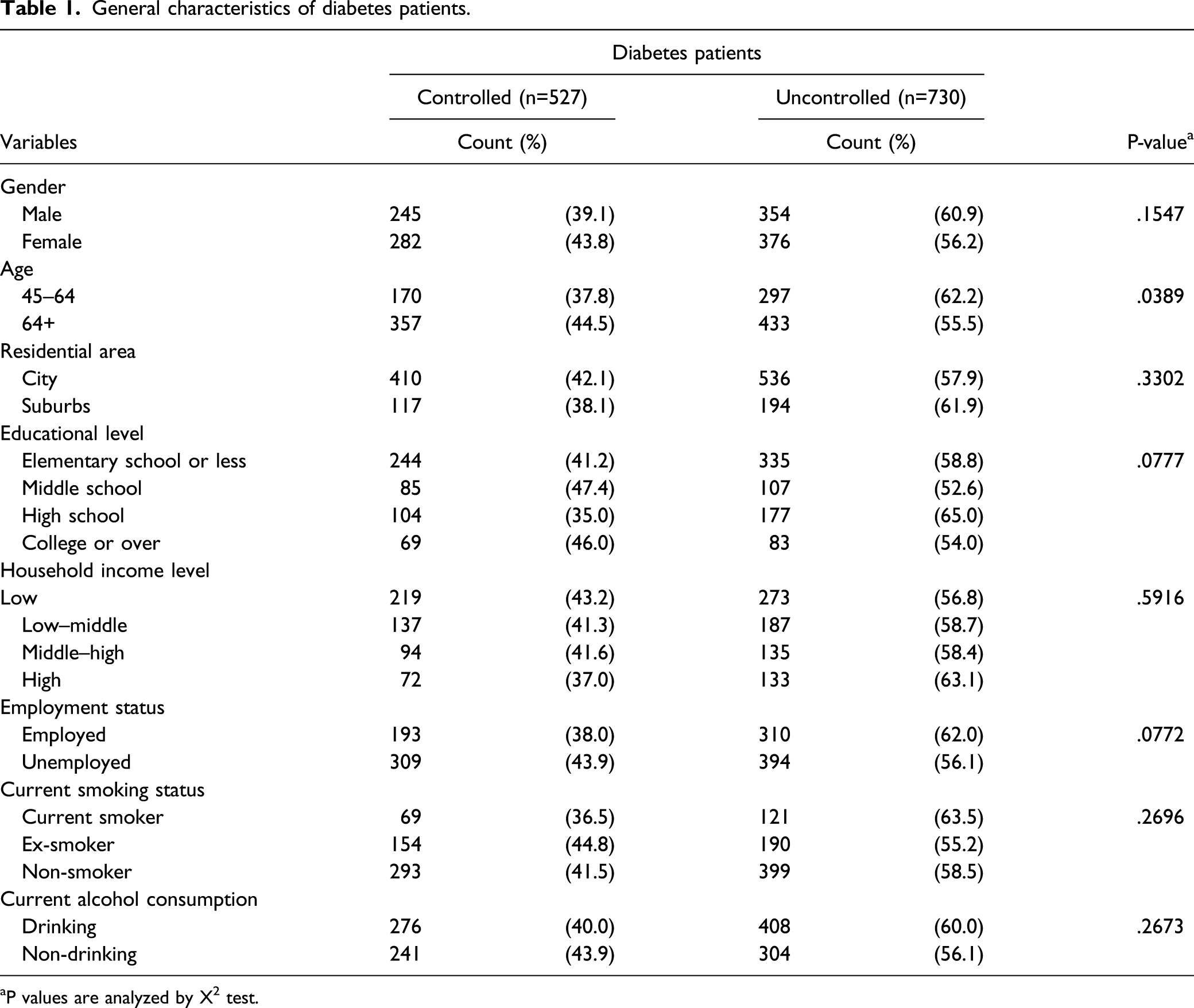
aP values are analyzed by X 2 test.
Blood control status according to body composition and blood indicators in diabetes patients.
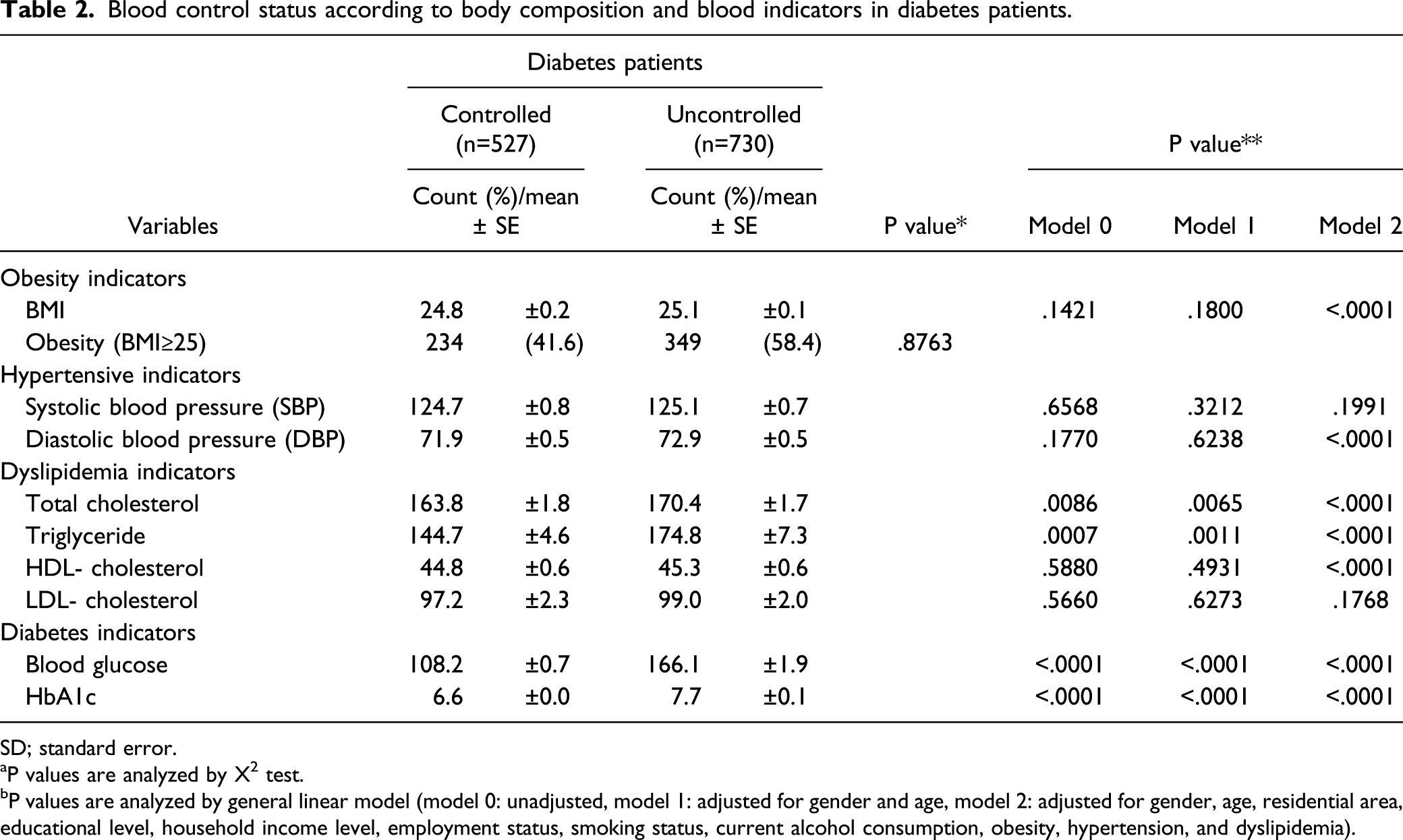
SD; standard error.
aP values are analyzed by X 2 test.
bP values are analyzed by general linear model (model 0: unadjusted, model 1: adjusted for gender and age, model 2: adjusted for gender, age, residential area, educational level, household income level, employment status, smoking status, current alcohol consumption, obesity, hypertension, and dyslipidemia).
Blood control status according to physical activities in diabetes patients.

SD; standard deviation.
aP values are analyzed by X 2 test.
bP values are analyzed by general linear model (model 0: unadjusted, model 1: adjusted for gender and age, model 2: adjusted for gender, age, residential area, educational level, household income level, employment status, smoking status, current alcohol consumption, obesity, hypertension, and dyslipidemia).
Macronutrient intakes of diabetes patients.

aP values are analyzed by general linear model (model1: adjusted for gender and age, model2: adjusted for gender, age, residential area, educational level, household income level, employment status, smoking status, current alcohol consumption, obesity, hypertension, dyslipidemia, and total energy intake).
Micronutrient intakes of diabetes patients.

aP values are analyzed by general linear model (model1: adjusted for gender and age, model2: adjusted for gender, age, residential area, educational level, household income level, employment status, smoking status, current alcohol consumption, obesity, hypertension, dyslipidemia, and total energy intake).
Discussion
Controlling blood glucose levels using a combination of pharmacotherapy and lifestyle changes, such as weight control and diet modifications such as low-carbohydrate, fiber-rich, and high-protein diet, is crucial for diabetes management.20-22 The present study evaluated anthropometric data, blood lipid concentrations, physical activity, and nutrient intake of patients undergoing diabetic therapy and compared their controlled and uncontrolled blood glucose levels by using data from the 2015–2017 KNHANES.
In this study, among 1257 subjects undergoing diabetic therapy, 527 (41.9%) patients controlled their blood glucose levels. This rate was higher than the 25.8% control rate published in the KNHANES for patients aged over 30 years from 2016 to 2018. 1 The difference is that in the KNHANES, the measurement of controlled glucose levels in diabetic patients was based on glycated hemoglobin (less than 6.5%), and blood glucose was the standard in this study. In the patients undergoing diabetic therapy, there was a significant difference in the control rate of blood glucose between middle-aged and elderly subjects, whereby 44.5% of elderly patients controlled glucose levels, which was higher than the 6.7% of middle-aged who controlled their glucose levels. Similar results have been reported in prior studies on glycemic control according to age group. Glycemic control according to age group showed optimal glycemic control was more prevalent among older individuals compared to younger individuals. 3 In other previous studies, individuals who had suffered diabetes for more than 10 years had a greater probability of glycemic control by 55% compared to those with diabetes for 10 years or less (OR = 1.55, p < .05). 4 These results show that middle-aged patients with early diagnosis of diabetes do not fully understand or practice self-management rules for glycemic control.
The majority of persons with type 2 diabetes are overweight or obese; weight loss through physical activity and nutritional therapy is often a first step to control diabetes worldwide.12,23,24 However, approximately 50% of diabetic patients being treated in this study were obese; the mean BMI of the uncontrolled patients (25.1) was significantly higher than that of the controlled patients (24.8) after adjusting for confounding factors. Besides, the total cholesterol and triglyceride levels of the uncontrolled group were significantly higher than those of the controlled group. The results of this study are consistent with the results that the BMI of the glycemic control group (25.0) was significantly lower than the non-glycemic control group (25.5) in Korean diabetic patients. 7 Therefore, appropriate daily habits, such as physical activity, and appropriate nutrient intake to aid in weight management may affect the insulin and antihyperglycemic medication doses required to control glucose levels. 13
The American Diabetes Association now recommends that patients with type 2 diabetes engage in moderate aerobic exercise. 10 In Korea, a study demonstrated that combined low- and moderate-intensity aerobic exercise improves HbA1c concentrations among people with type 2 diabetes mellitus between the age of 30 and 90 years. 11 In the present study, the total amount of moderate-intensity exercise during work, leisure, and commuting among controlled patients was significantly higher than that among uncontrolled patients, and the control rate among patients engaging in moderate-intensity exercise during work, leisure, and commuting for over 240 minutes per week was significantly higher than that among patients with less than 240 minutes of such activity per week. These findings demonstrate the importance of investigating the effects of exercise according to intensity levels, frequency, and duration on blood glucose control among middle-aged and older diabetic patients.
The American Diabetes Association also recommends that patients undergoing diabetic therapy follow the dietary guidelines for the general population. 14 However, in the present study, the total energy, fat, saturated fatty acid, and cholesterol consumption in the uncontrolled group was significantly higher than that in the controlled group after adjusting for confounding factors and energy intake. A national cross-sectional study revealed that diabetes patients consumed more saturated fat than recommended. 15 About two-thirds of type 2 diabetes patients consume more fat and saturated fat than recommended. 16 Several micronutrients are known to be important in the management of diabetes.25-27 For example, there are meta-analyses demonstrating that low calcium levels may negatively affect glycemic levels. 28 Potassium and vitamin C are found in a variety of fruits and vegetables, and potassium may influence insulin secretion. 29 In this study, the consumption of calcium, phosphorus, potassium, riboflavin, niacin, and vitamin C in the uncontrolled group was found to be significantly lower than that in the controlled group after adjusting for confounding factors and energy intake. The intake of water-soluble vitamins in the uncontrolled group was significantly lower than that in the controlled group. These results show that the intake of some micronutrients and water-soluble vitamins may be beneficial for blood sugar control.
The current study had several strengths. First, our investigation provided evidence of a relationship between moderate-intensity activity time and blood glucose control in diabetes patients taking medications or receiving insulin therapy. Second, this study focused on the association of macro and micronutrient intake with blood glucose control in diabetes patients. Finally, our study was a national population-based analysis using KNHANES data, which strengthens the statistical reliability of the results and data. However, the present study has some limitations, which should be researched by further investigation. First, this cross-sectional study design did not allow us to make conclusions regarding the causal relationships between blood glucose control and physical activities or nutrient intakes. Second, this study identified only one blood glucose as an indicator of glycemic control. Future studies should investigate using various glycemic control parameters including hemoglobin A1c, glycated albumin, and fructosamine.
In summary, the findings of the present study support recommendations for patients with diabetes to engage in moderate-intensity physical activity while going about their daily routines (work, leisure, and commuting). The findings also emphasize the importance of certain micronutrients for blood glucose management among middle-aged and older patients on diabetes treatment. The results indicate that changes in body composition effected by physical activity and adequate daily nutrient intake are crucial elements of diabetes management. Clinicians should emphasize the importance of appropriate physical activity and nutrient intake to their patients in addition to providing education on diabetes therapeutics.
Footnotes
Acknowledgments
This work was conducted in collaboration with researchers from Shezline Medical Center and Research Institute of A&P Lab, Inc. The authors and researchers thank the two institutions.
Author Disclosure
The present study design was approved by the Institutional Review Board of the Korean Ministry of Health and Welfare (IRB number: P01-202003-21-004). Consent for publication: Not applicable.
Authors’ contributions
YM Kim:
Contributions: undertook data collection, analysis, interpretation, and manuscript writing.
JD Kim:
Contribution: undertook data collection analysis, interpretation, and manuscript writing.
HN Jung:
Contribution: conceived the study question and contributed to the study design, supervised data collection, analysis, interpretation, and manuscript writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.