
Abstract
Cancer is one of the leading causes of death globally and expenditure associated with cancer is quite high. Efficient resource allocation needs information on economic evaluations of healthcare interventions. The purposes of the study are to provide a comprehensive overview of cancer patients’ willingness to pay (WTP) for healthcare services and to investigate the influence of democracies, culture dimensions, and other factors on WTP. A meta-analysis was conducted using PubMed, Scopus, and Google Scholar to identify all studies of stated preference approach to estimate cancer patients’ WTP healthcare services. A set of criteria was constructed for selecting relevant studies. A total of 79 studies were related to selection criteria and held sufficient information for the purposes of meta-analysis. A total of 393 estimates of WTP from 79 healthcare valuation studies were pooled to identify the links between WTP and influential factors. The findings suggest that values of benefits in healthcare services are higher in more democratic nations, but they are lower in cultural traits that are stronger indulgence and uncertainty avoidance. Further, the types of cancer matter. Compared to breast cancer, WTP is higher for skin cancer, yet lower for liver cancer and lymphoma. A higher national income and public health expenditure increase WTP for healthcare services, while a higher death rate by cancer leads to lower values of healthcare benefits.
Keywords
Political institutions and culture differences influence cancer patients’ preferences and healthcare valuations.
How does your research contribute to the field?
This research is the first meta-analysis to examine the impact of democracy and culture on cancer patients’ WTP for healthcare services
What are your research’s implications toward theory, practice, or policy?
Promoting democracy is one way to improve the effectiveness and efficiency of the healthcare system and the control of cancer.
Introduction
Despite recent advances in medical technologies, changing diagnostic and treatment patterns, and continuous personnel development of healthcare professionals,1,2 cancer remains the world’s second leading cause of death 3 with an estimated over 19 million people being diagnosed and 10 million deaths from cancer in 2020. 4 Efficient resource allocation has become a major challenge for decision-makers and healthcare providers, 5 leading to increasing demand for information on economic evaluations of health and healthcare interventions.
Economic evaluation offers a means for measuring and comparing the benefits and costs of alternative healthcare intervention. 6 In recent decades, willingness to pay (WTP) derived from stated preference approach such as contingent valuation method (CVM), discrete choice experiment (DCE), and conjoint analysis (CA) has become the mainstream approach to measure health benefits in money terms. 7 This approach is also applied to set priorities for healthcare programs and predict demand and the expenditure financing for healthcare services.8-10
Recently, there is expanding literature on stated preference studies to elicit cancer patients’ preferences and their WTP for healthcare services. These studies focus on cancer screening, diagnosis, treatment, and prevention, including palliative care and hospice care. Yet these results from individual studies raise some difficulties for decision makers in handling the accumulated information to understand cancer patients’ attitudes toward healthcare services and identify the main factors determining WTP estimates. Analyzing the key drivers of WTP for cancer cares will assist in the policies and programs designed to better meet patients’ preferences.
To extract information from the expanding pool of empirical studies, this is leading to the use of meta-analysis (MA). MA is a statistical analysis of research outcomes from individual studies11,12 and integrates the findings into a single conclusion. 13 It can also clarify heterogeneity between study results. 14 Therefore, MA is ideally suited in consolidating findings from diverse studies conducted in different years and countries and using different research designs and to answer the question what are the determinants of WTP values.
However, MA-studies of cancer patients’ preferences and WTP for healthcare services are relatively scarce. One prior MA-study of chronically ill patients’ preferences and WTP for medical treatment is reported by Chaikumbung. 12 This MA-study also explore the influence of external variables (eg, economic freedom, democracy, and culture) on patients’ preferences. This prior MA study provides information about the main factors determining WTP and understanding of the role of institutions and cultures in shaping patients’ preferences. Nevertheless, much more research is necessitated to further investigate the relations between institutions and cultures prevailing within countries and the valuation of cancer care.
Institutions i and cultures ii can potentially affect cancer patients’ preference and their WTP for health services. Due to the information asymmetries iii in healthcare market,17-19 patients need information related to their illness, particular types of medical cares, course of medication, and the quality and cost of medical services thus before accessing appropriate cares where they should be diagnosed and treated for cancer, they may incur substantial costs of acquiring and processing the information required and cost of bargaining and enforcement of contracts.iv,20,21 Under such circumstances, patients cannot make the best judgment about their welfare, 12 if without support of institutions or social processes. 15 North 22 emphasizes that institutions are external rules and invented to simplify coordination and reduce uncertainties and transaction costs. Good institutions like democratic governance enable to facilitate accessibility and exchange of information 23 on health services particularly types, quality, and locations of the available medical cares. Better information can change attitudes and preferences toward healthcare services. 24
Furthermore, using healthcare services is related to uncertainty and risk, since recovery from sickness is unpredictable and patients may make a wrong decision in choosing treatment options which can cause risk of death.19,25 Actually, in times of illness particularly diagnosis of cancer toward the end of life, individuals cannot make a rational choice to maximize their welfare, as perhaps they don’t understand information about a medical decision and suffer from cognitive bias. 26 In essence, patients need the support of institutions/social processes to cope with this circumstance by shaping appropriate emotional and behavioral responses to cancer 27 and simplifying life and complexity to act rationally. 28 Strong institutions influence the implementation and formulation of effective health policies to improve health care quality including accessible healthcare services and health insurance. 12 Indisputably institutions possibly impact on patients’ decision to use cancer care services. Nonetheless, the different ways that individuals deal with the course of illness highly depend on their cultural background. 29 Therefore, differences in institutions and cultures across countries may express variation in preferences and WTP for cancer care.
Given the need to extend the line of inquiry by exploring the links between institutions and cultures and the valuations of healthcare services and identifying the key determinants of WTP values, the aims of the study are to (1) provide a comprehensive overview of cancer patients’ WTP for healthcare services, (2) to explore the influence of institutions, and culture dimensions on WTP estimation, and (3) to identify the main drivers of WTP values.
This present MA focuses on the effects of political institution (democracy), culture dimensions (Individualism, indulgence, power distance, long-term orientation, uncertainty avoidance, and masculinity) on WTP estimates, using an assembled dataset of 79 studies of WTP for cancer care. Information on the relation between institutions and cultures and the valuations of healthcare delivery and the key determinants of WTP values may help guide policy decision makers and healthcare providers in understanding the environment in which nations improve the performance of healthcare services.
The following section describes the construction of the meta-dataset and methodology. Section 3 reports the results of MA and discussion is presented in section 4. Section 5 concludes the paper.
Materials and Methods
Data
This article was conducted in line with the Meta-Analysis of Economics Research Network (MAER-Net) protocols 30 and PRISMA Statements 31 for search strategies, eligibility criteria, study identification selection, and coding strategies. The summary of study selection process is presented in Figure 1.

Flow diagram of study selection.
Search strategy
To collect relevant studies, using 3 search engines (PubMed, Scopus, and Google Scholar) searches all the primary studies. The search was conducted between January 2018 and July 2019. Several keywords were employed to conduct the search strategies, such as “patient preferences,” “willingness to pay,” “discrete choice experiment,” “conjoint analysis,” “contingent valuation,” “economic valuation,” and “healthcare valuation” in combination with each of the following words: (1) cancer care, (2) cancer screening, (3) cancer diagnosis, (4) cancer treatment, (5) cancer prevention. In total, 3676 studies were identified in this search process.
Eligibility criteria
To be included in the MA-dataset, a set of criteria was constructed for selecting studies. Purposely, a study had to:
Study types: The focus of the MA was on empirical WTP studies estimated by stated preference approach (CVM, DCE, CA)
Types of diseases: only studies estimating WTP focused on cancer
Types of healthcare services: The studies had to estimate WTP for treatment, screening, diagnosis, and prevention (including HVP vaccination).
Issues on the WTP values: The studies reported WTP in terms of monetary values.
Publication sources: WTP studies from book chapters, journal articles, theses, dissertations, working papers, and proceedings papers were included.
Study identification and selection
At end of the search process, there were 111 studies related to the search criteria. However, only
External information
To examine the effect of political institution and culture on WTP estimates, some data were collected from external sources. First, democracy degrees were collected from Polity Index Project. Second, culture was collected from Geert Hofstede. Third, GDP per capita, public health expenditure, life expectancy, death rate by cancer, birth rate, and compulsory education data were collected from the World Bank. Forth, religious data were collected from the World Population Review.
Data description
In total, 393 observations from 79 WTP studies published between 1997 and 2019 are from 20 countries. vii The largest number of observations is from United States (USA), followed by United Kingdom (UK), Canada, and Australia, respectively. The average WTP for healthcare services is US$ 187.77 person per month. Average WTP values are highest in Germany, followed by Canada, UK, and USA, respectively, with the lowest WTP recorded for China.
In total 20 countries included in the MA-dataset, the degrees of democracy vary between countries. As expected democracy index may affect WTP estimates. Figure 2 plots the natural logarithm WTP per person per month against democracy degree. The lowess-smoothed curves suggest that democracy seems to have a positive relationship with WTP.

WTP plotted against democracy (US$2011 per person per month; log scale).
Meta-analysis Models
MA is a regression analysis of research outcomes from prior original studies. For this paper, Meta-analysis involves regressing the WTP estimates reported from several individual studies against various covariates that relate to attributes associated with each type of cancer and research design. The dependent variable is a vector of monetary values representing cancer patients’ preferences for healthcare services, labeled Yij. The subscripts i and j are the ith estimate from the jth study. The explanatory variables fall into 4 groups: (i) a matrix of institutions and cultures, XD; (ii) a matrix of cancer types, XC; (iii) a matrix of socio-economic characteristics Xs, and (iv) a matrix of valuation methods, Xm.
Following most prior MA-studies of non-market valuation, this present paper uses the base semi-logarithmic model. The estimated MA model is:

Where α is the constant term, β D , β c , β s , and β m are estimated parameters associated with the respective groups of independent variables, and ε is the error term.
The MA model, equation (1), is used to explain the heterogeneity in reported WTP values. Purposely, this model is applied to:
(1). Identify differences in valuations by the quality of institutions and culture differences within a country: Do cross-country difference in institutions and cultures express variation in preferences and WTP for healthcare services?
(2). Identify differences in valuations by types of healthcare services: Are some healthcare services more valuable than others?
(3). Identify country differences in WTP values: How different are preferences for healthcare services between different countries?
Estimation
Ideally equation (1) is estimated by using weighted least squares (WLS) and employing the inverse variance as weights. However, in the case of WTP studies Stanley and Rosenberge 32 recommend that should use the inverse of the square root of the sample size as the standard error.
The 79 studies included in this dataset report multiple estimates per study hanging on whether they use different model estimations, payment vehicles, and sample groups. To handle data holding multiple estimates per study, this paper treat the datasets as panel datasets and adjusts the standard errors for clustering of estimates within studies which this approach is widely used in prior MA-studies such as Oczkowski and Doucouliagos, 33 Chaikumbung et al,34,35 and Chaikumbung. 36
Establishing causality
The main purpose of this study is to examine the links between democracy and healthcare valuation and identify the main drivers of WTP for healthcare services. Nevertheless, perhaps it is not the case that democracy and control variables affect WTP values. Perhaps these are caused by something else. It’s not a direct causal relationship. For example, perhaps people living in a society are more likely to want democracy and healthcare services. In this case, it is not democracy that drives healthcare valuations, rather its citizens’ preferences for both democracy and healthcare services. Also it could be that high public health spending may manifest in both higher WTP and greater public health expenditure.
To mitigate the risk of reverse causality, this study follows Chaikumbung et al 35 and Chaikumbung 36 by using three 3-year lags in democracy and also public health expenditure variables. Lagged values are based on the idea that even if democracy and public health spending today are correlated with WTP for healthcare services but not causing them, then lagged values in democracy and public health expenditure are more likely to cause valuations. That is, democracy and public health expenditure from 3 years ago are more likely to be a causal factor in WTP for healthcare services today. Nonetheless, the use of lags may be insufficient to alleviate reverse causality. Hence, this result should be interpreted as correlated rather than causal.
Publication selection bias
Publication selection bias may potentially distort statistical inferences. Publication bias in body of the literature may occur when selection criteria prefer statistically significant results. 37 To detect publication bias in the literature, Stanley and Doucouliagos 38 recommend construction of the funnel plots. The funnel plot can identify the shape/distribution of reported estimations. A funnel plot should be symmetric based on the underlying data assumptions—if the data are normally distributed, then symmetry is maintained. 39
Variables
The variable names and definitions in this MA dataset are presented in Table 1.
Description of Meta-Analysis Variables.

The dependent variable
The dependent variable is the WTP for healthcare services. Both mean WTP and marginal WTP are included in MA-dataset. Mean WTP values are estimated from CVM, DCE, and CA. However, some DCE and CA studies report marginal WTP rather than mean values. Following Ma et al, 40 the marginal WTP could be treated as the mean WTP, since WTP values of CE and CA studies included this dataset are derived from linear utility functions.
WTP estimates are reported in different currencies, years, and metrics (eg, WTP per individual per year, WTP per household per annum, WTP per household per month, WTP per person per visit, viii WTP per individual per 3 weeks, ix and WTP per individual per 5 years x ). To ensure comparability, all WTP values were converted into WTP per person per month using purchasing power indices, expressed in US$ 2011.
The explanatory variables
Institutional and cultural variables
The institutional variables are democracy and culture. The democracy index was collected from the Polity Project by using the Polity II data. In this dataset, the index of democracy ranges from −7 to 10.
Culture determines the different ways that individuals understand diseases. Six dimensions of culture: individualism, indulgence, power distance, long-term orientation, uncertainty avoidance, and masculinity were included in MA model.
Healthcare types and types of cancer
Healthcare types considered to include in this dataset are screening, diagnosis, treatment, and protection. Types of cancers were grouped into 12 types of cancer xi : (1) Breast cancer, (2) Prostate cancer, (3) Cervical cancer, (4) Lung cancer, (5) Colorectal cancer, (6) Skin cancer, (7) Pancreas cancer, (8) Lymphoma, (9) Leukemia, (10) Liver cancer, (11) Ovarian cancer, (12) Other cancers. The largest observation is Breast cancer followed by Colorectal cancer, Lung cancer, and Prostate cancer, respectively. Hence, Breast cancer is chosen to be the baseline category.
Socio-economic variables
Various socio-economic variables are included in the MA model: GDP per capita (PPP) expressed in 2011 US$, public health expenditure, life expectancy, death rate by cancer, birth rate, population density, and locations. Empirical valuation studies from 20 countries were grouped into 7 locations: USA with 152 observations, UK with 72 observations, Canada with 36 observations, Europe with 20 observations, Australia with 27 observations, Asia with 83 observations, and Africa with 3 observations.
Valuation method variables
The years of survey, publication status, and survey administration were included in the MA model. Survey administration was classified into 4 groups: face-to-face interviews with 179 observations, mail with 91 observations, telephone with 34 observations, and online with 102 observations.
Results
Publication bias
Figure 3 presents a funnel plot of 393 estimates. The figure plots WTP against precision. This study employs the square root of the sample size to construct a proxy for precision. A funnel plot seems to be asymmetric. Therefore, it is possible that there is sign of publication selection bias in this literature.
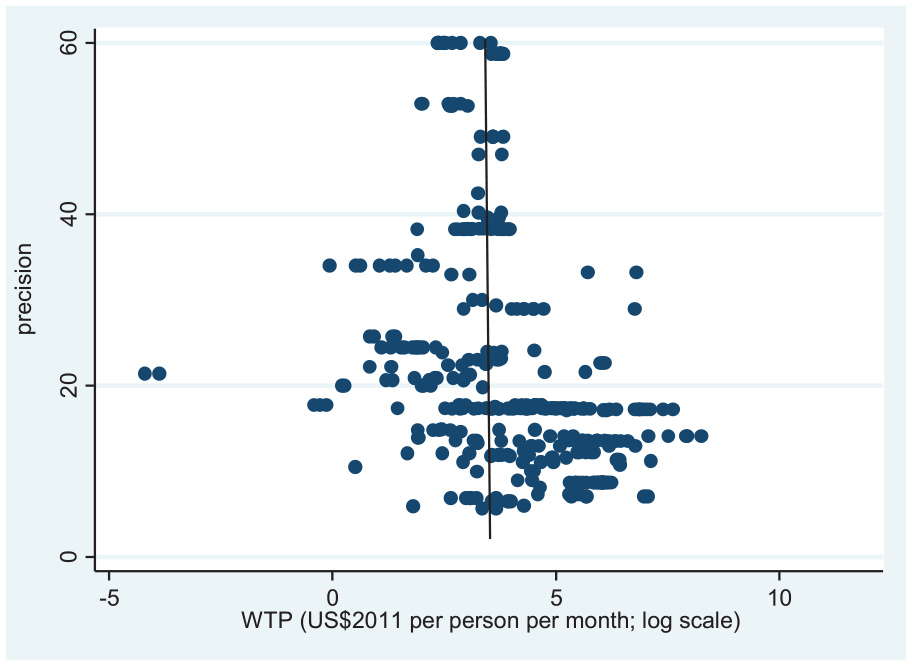
Funnel plot for WTP for healthcare services.
MA results
Table 2 presents the results of MA models. Model 1 considers merely at the partial relationship with institutional and cultural variables. Control variables are added in Model 2 and Model 3 is a general-to-specific model. The presence of multicollinearity is problematic to MA models, thus this paper applies a general-to-specific modeling strategy, as recommend by Stanley and Doucouliagos 44 to gain greater clarity in results. Model 1, Model 2, and model 3 present the baseline results. Model 4 reports a general-to-specific model with the year of survey fixed effect. This fixed effect controls for factors changing each year. The result of a general-to-specific model with the country fixed effect is presented in Model 5. This model controls for country characteristics that remain constant over time. 3-year-lags in democracy and public health expenditure are introduced in Model 6. The results of Model 6 are even less probable to be afflicted with reverse causality. The adjusted R2 value of Model 1 is 0.114 suggesting that only democracy and culture can explain more than 11% of the variation within WTP for healthcare services. The addition of control variables in Model 2 to 6 significantly improves the model, reflected in higher adjusted R2 value: 70% to 74%.
MA of WTP for Healthcare Services.

Note. Figures in brackets are standard errors. *Statistical significance at 10%. **Statistical significance at 5%. ***Statistical significance at 1%.
Regarding the influence of institutions on WTP estimates, democracy is robust having a positive impact on WTP for healthcare services. Culture traits appear to influence on WTP values. Uncertainty avoidance and indulgence are significantly negatively correlated with WTP.
The types of healthcare services affect respondents’ WTP. The coefficients on cancer screening is consistently negative and statistically significant across all models. Also coefficients on diagnosis test and prevention are negative. The types of cancer influence WTP values. Significant positive correlation is found for skin cancer. Additionally, coefficients on cervical cancer, prostate cancer, colorectal cancer, pancreas cancer, and ovarian cancer xii are positive but these findings are insignificant. In contrast, liver cancer and lymphoma have a robust negative effect on WTP. Besides, lung cancer and leukemia xiii have a negative coefficient.
In terms of the effect of socio-economic characteristics on cancer patients’ preferences, Per capita income is positively and significantly related to values of healthcare benefits. Public health expenditure is positively and significantly associated with WTP, while life expectancy has a negative impact on WTP estimates. Death rates by cancer are robust in having a negative effect on WTP estimates. Buddhism is statistically significant with having a positive impact on WTP values. Canada, UK, and Australia are positively significant variables. Contrastingly, Africa has a negative coefficient, yet this result not robust due to based on 3 observations.
Valuation methods can affect cancer patients’ WTP. Out-of-pocket variable is positive and significant. Mail survey and online survey tends to have a negative effect on WTP while telephone is negatively related to WTP. A survey including socio-economic information has a significant positive effect on WTP, while information about cancer knowledge is negatively correlated with WTP. The pilot survey is statistically significant with having a positive impact on WTP, whereas the focus group is negatively associated with WTP. Further, the quality of studies impacts on WTP values. Published articles have significantly negative effect on WTP, whilst impact factor is negatively related to WTP.
Discussion
The MA results confirm that democracy matter. Individuals in more democratic nations spend more on their health, conforming to the finding of Chaikumbung. 12 A plausible explanation for this might be that democratic governments adopt policies favorable to their re-election, so they use feedback from a broader range of interest groups through open public debate, free media, and discussion to improve the quality of healthcare services45-48 such as more accurate diagnosis, more broadly accessible medical care, and more effective treatment and prevention. 49 In addition, citizens in democracies are better informed, especially 46 about types, quality, and locations of the available medical cares, a new therapy, options of a new medication, and progress in cancer screening and early detection. These can result in a higher WTP for healthcare services.
The MA controls for 6 dimensions of culture. Of these, respondents from a stronger uncertainty avoidance and indulgence culture background place on a lower value of benefits in health cares. Uncertainty avoidance reflects the level society’s tolerance for uncertainty and ambiguity. A high score means that societies have a low tolerance for ambiguity and uncertainty. Patients from a stronger uncertainty avoidance culture have more need for a definitive prognosis and outcomes expectations.16,50 Yet uncertainty pervades medical diagnosis and treatment, 51 particularly cancer treatment outcome is unpredictable. Indulgence refers to the extent to which individuals attempt to control natural desires and impulses. 16 More indulgence societies stand for a relatively weaker constrain of feelings and basic human desires related to enjoying life, such as consumption, spending money, and recreation.52-54 However, the utilization of healthcare services is closely related to anxiety and requires follow-up screening and diagnostic tests, and adhering treatment plans. Therefore, the MA results suggest that societies categorized by greater uncertainty avoidance and indulgence invest less in their health.
The types of healthcare services also matter. WTP for cancer screening and diagnosis are significantly lower than cancer treatment. One explanation for this might be that respondents may have more information and experience about the full costs of cancer screening, diagnosis, and treatments. Compared to breast cancer, WTP estimates are significantly higher for skin cancer but lower for liver cancer and lymphoma. A plausible explanation is that WTP values seemingly are related to 5-year cancer survival rate. Of these, according to Allemani et al, 55 the cancers with the highest 5-year survival estimates are skin cancer, breast cancer and lymphoma, respectively while liver cancer is the lowest survival. Nevertheless, survival rates may depend on system is in detecting the disease and whether patients have rapid access to effective treatment. 56 Therefore, it could be implied that the effectiveness of services is important in determining the willingness to fund healthcare services.
Per capita income has a positive impact on WTP estimates, consistent with economic theory that WTP should vary with ability to pay or wealthier people certainly have a greater WTP for goods and services.39,57-59 Also this is the common findings in the economic valuation literature of health benefit (eg, Whynes et al 60 and Milligan et al 61 ) and meta-analysis literature of health benefit valuation (Chaikumbung 12 and Vassanadumrongdee et al 62 ). In the current study, the ranges of income elasticity take from 2.15 to 4.07. That is, cancer care services are luxury goods and values of these services are income elastic.
Greater public health expenditure leads to a higher WTP estimates. An explanation for this finding might be that larger public health expenditure reflects increasing investment in medical technology innovations. 63 This can potentially result in higher-quality care and greater efficiency in healthcare delivery, thus patients are more likely willing to fund healthcare services. An alternative explanation is that there is correlation between WTP and lags in public health spending. That is, a large public health expense might manifest in both higher WTP and greater public health expenditure in a nation. In contrast, the longer lifespan decrease WTP values suggesting that if patients expect to live longer, then will invest less in their health. 12 A possible explains for this is that longer lifespans in a country where most population are old 64 which elderly individuals may face with choosing between spending for health care or daily living expenses. 65 An another alternative explanation for these findings might be that there are results that larger public health expenditure increase life expectancy66,67 and longer lifespans generates higher public health expenditure because older individuals tend to use healthcare services more often than younger persons. 63 Therefore, it could be that there is a correlation between public health expenditure and life expectancy (see for example: Jaba et al, 68 and Bein et al 69 ).
Higher death rates by cancer decrease WTP estimates. It is possible that higher cancer mortality rate can potentially reduce trust in the quality of healthcare services. That is paying more do not warrant better outcome. This MA finding has an implication that higher death rates by cancer can decrease access to care and the utilization of health cares among cancer survivors and individuals without cancer. Religious beliefs influence cancer patients’ preferences. Buddhist society assigns a higher value of healthcare services. One explanation may be that Buddhist belief provides better understanding and coping with a life-threatening disease particularly the knowledge of the impermanence of all things, being present with compassion, and meditation practice. 70 Thus Buddhist belief and practice may help patients to live with hope for cure and survival.
Survey designs and the quality of studies significantly influences on WTP estimates. The survey using out-of-pocket costs as payment vehicle generates a higher WTP than income taxes and health insurance. The MA result suggests that WTP in DCE, CA and CVM studies could be sensitive to how payment vehicle is made. Published articles report lower values than non-published sources. This is a general finding in MA literature (eg, and Chaikumbung et al, 34 Enjolras and Boisson 71 and Camacho-Valdez et al 72 ). Estimated WTP published in journal papers may be subject to peer review and this process may introduce more conservative valuations. Yet, high impact factor journals prefer higher values of healthcare services.
However, this MA study faces some limitations that should be considered. First, the MA-dataset includes empirical studies with quite small sample sizes. This potentially leads to sampling error/publication bias in MA. 73 Second, the MA focuses on pooling values for different healthcare services and different valuation methods, although a MA study requires commodity consistency.34,74 Third, one potential limitation is that this MA may omit important variables (symptom severity, psychosocial factor, ethnicity, etc.) in explaining variation in WTP estimates. Hence, cautions are suggested in interpreting these findings. Further MA research should focus only on specific healthcare services (eg, cancer screening, or cancer diagnosis, or cancer treatment) and include important variables influencing WTP. Meanwhile, there is a need for new primary WTP studies of cancer cares, since a larger number of studies in MA research offer more precision of estimates.75,76
Conclusions
This article provides a synthesis of estimates of cancer patients’ WTP for healthcare services and an identification of the main determinants of the WTP values through MA. An interesting finding is the importance of democracy, GDP per capita, public health expenditure, death rate by cancer, culture, and religion variables in explaining variation in WTP estimates.
Democracy, GDP per capita, and public health expenditure have a positive impact on WTP estimates suggesting that individuals in a nation with more democracy, higher income, and greater public health expenditure invest more in their health. Contrarily, death rate by cancer is negatively correlated with WTP estimates inferring that higher death rate by cancer has a potential to decrease access care and the use of healthcare services. Societies categorized by greater uncertainty avoidance and indulgence assign lower values for healthcare benefits, while Buddhist societies place on a higher value of care services.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211024894 – Supplemental material for Democracy, Culture and Cancer Patients’ Willingness to Pay for Healthcare Services: A Meta-analysis
Supplemental material, sj-pdf-1-inq-10.1177_00469580211024894 for Democracy, Culture and Cancer Patients’ Willingness to Pay for Healthcare Services: A Meta-analysis by Mayula Chaikumbung in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Author would like to thank seminar participants at the 2018 Melbourne MAER-net Colloquium, and Prof. Helen Scarborough, Prof. Chris Doucouliagos, Prof. Samonpon Suttubak and Waraphorn Phuangbut for valuable comments on this work.
Grant Disclosures
This research receives grant from the Research and Development Institute, Kasetsart University, Sakon Nakhon Province Campus, Thailand.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
The dataset for this analysis are available in the (MA-cancer-Mayula.xlsx) and (MA-cancer Mayula.dta), repository. https://zenodo.org/deposit/4399500# or ![]()
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.