
Abstract
Health professionals tend to perceive some diseases as more typical than others. If disease typicalities have implications for health professionals or health policy makers’ handling of different diseases, then it is of great social, epistemic, and ethical interest. Accordingly, it is important to find out what makes health professionals rank diseases as more or less typical. This study investigates the impact of various factors on how typical various diseases are perceived to be by health professionals. In particular, we study the influence of broad disease categories, such as somatic versus psychological/behavioral conditions, and a wide range of more specific disease characteristics, as well as the health professional’s own background. We find that professional background strongly impacted disease typicality. All professionals (MD, RN, physiotherapists and psychologists) considered somatic conditions to be more typical than psychological/behavioral. As expected, psychologists also found psychological/behavioral conditions to be more typical than did other groups. Professions of respondents could be well predicted from their individual typicality judgments, with the exception of physiotherapists and nurses who had very similar judgment profiles. We also demonstrate how various disease characteristics impact typicality for the different professionals. Typicality showed moderate to strong positive correlations with condition severity and mortality, and only non-severe conditions were rated as atypical. Hence, studying how different disease characteristics and occupational background influences health professionals’ perception of disease typicality is the first and important step toward a more general study of how typicality influences disease handling.
Keywords
Health professionals ascribe different prestige to various diseases and they consider certain diseases to be more typical than others, but little or nothing is known about why they do so.
This is the first study that investigates what makes health professionals consider some diseases to be more typical than others.
how typical professionals find diseases can influences how they treat these diseases and persons having them. Knowing what drives this differentiation is a prerequisite for handling the problem.
Highlights
Health professionals tend to perceive some diseases as more typical than others.
This is of great social, epistemic, and ethical interest in cases where disease typicalities have implications for health professionals or health policy makers’ handling of different diseases.
We find that professional background impacted disease typicality.
All professionals (MD, RN, physiotherapists and psychologists) considered somatic conditions to be more typical than psychological/behavioral ones.
Severity and mortality also influence whether professionals consider conditions to be typical diseases.
Studying how different disease characteristics and occupational background influences health professionals’ perception of disease typicality is the first and important step toward a more general study of how typicality influences disease handling.
Introduction
The concept of disease is crucial to healthcare—both theoretically and practically. It defines the goal of medicine: detecting, understanding, treating, curing, and/or palliating disease. Moreover, it has a normative function in demarcating who is entitled to attention, care and treatment. 1 Disease also directs the action of health professionals. Moreover, it decides a person’s social role and status,2–5 for example, who gets sick leave and sick pay,6,7 and it can determine a person’s moral and legal accountability.1,8–10 Hence, disease is a core concept in health care, in health policy making, and in society at large.11–13
Despite the crucial role of the concept of disease, it is notoriously difficult to define.10,11,13–19 From a theoretical point of view it can be argued that the concept of disease is defined by its constituents (according to classical concept theory), by its relation to the world (conceptual atomism), by its description (descriptivist theories), by theories (theory theory of concepts), by perceptual and motor states (neo-empiricist theories), by natural kinds (natural kind theory), 20 by actual exemplars in memory (exemplar theory),21,22 by abstract average prototypes (prototype theory),23–27 or as fuzzy sets (fuzzy theory of concepts). 28 Despite long and thorough debates, no agreements are obtained.
From an empirical perspective, diseases have been found to make up a prestige hierarchy.29,30 Organ specific, acute, and actionable conditions where you can use advanced technologies have high prestige among health professionals. Correspondingly diseases have been shown to be more or less typical.31–33 According to prototype theory our concepts are structured on the basis of their similarity to some central prototype representation.34–36
If such prestige hierarchies or disease typicalities have implications for health professionals or health policy makers’ handling of different diseases, then it is of great social, epistemic, and ethical interest.37–39 From other areas we know that typicality affects what people consider to be trustworthy and good. 40 Hence, if some diseases are considered as better or deserve more attention due to their typicality, this has implications for patients, professionals, and policy makers.
In a previous study 33 among Norwegian health professionals, it has been shown that some conditions are considered to be very typical diseases. Examples are lung cancer, leukemia, colon cancer, myocardial infarction, AIDS, diabetes, multiple sclerosis, and schizophrenia. Others score very low on how typical they are perceived to be, for example caffeine-dependency, kleptomania, and infertility. 33
The objective of this study was to investigate what makes professionals perceive some diseases as more typical than others. In particular we wanted to assess the importance of specific characteristics of the health professionals (profession) and some features of the conditions (somatic vs psychological/ behavioral; mortality; prevalence; severity; media coverage; curability; etiology).
Our specific research questions were:
What is the impact of broad disease category on perceived typicality among different professional groups?
Can different respondent professions be discriminated based on their perceived typicality of diseases?
What are the individual and combined effects of disease characteristics (such as mortality; prevalence; severity; media coverage; curability; etiology) on perceived typicality?
Methods
To answer our research questions, we used the dataset from an earlier study investigating how typical health professionals considered various conditions to be, 33 and we compiled a data set with information about each condition. Conditions were included partly based on a study of health professionals’ conceptions of prestige related to diseases 30 where diseases were selected to represent a broad range of conditions handled by a variety of specialities. The respondents were asked to rate whether they found the diseases more or less typical.
Typicality was explained in terms of how people would find different birds, such as sparrows versus ostriches, more or less typical of birds. Answers were given from 0 to 10, where 0 was atypical, and 10 was very typical. The final survey, which was in Norwegian, was printed on white paper (1 page, 2-sided). More background details are available in Hofmann. 33 The diseases used may also be seen displayed in Figure 1.

Scatterplot of mean typicality of diseases by severity, grouped by mortality (in Norway), and category (somatic, psychological/behavioral, ambiguous).
One of the authors (BH) designed the survey and distributed it to 254 health related professionals while they were attending university courses or seminars at the Faculty of Medicine, University of Oslo, during the spring terms of 2010 to 2014. The respondents were categorized as MD (42), RN (67), physiotherapists (22), psychologists (13), and others (52). The latter category encompassed dentists, biologists, epidemiologists, social scientists, philosophers, and professionals with backgrounds from other humanities. Forty-seven respondents had missing information on professional background, and their data were only included in the average scores. The respondents either had education at Masters (135) or Bachelors (119) level.
The data were registered manually in Microsoft Excel 2010. Statistical analyses were performed with R version 3.6.3, 41 and IBM-SPSS, and plots were created with ggplot2 3.2.1 42 and sjPlot. 43 Minor misprints in the data were corrected and 11 respondents with more than 20% missing responses were removed, in addition to one disease (neurasthenia) with 26% missing data.
To investigate the importance of type of disease, we categorized the diseases based on the presence or absence of predominantly psychological/behavioral components. While all internal, psychological states and conditions are likely to show some form of external correlate in the body, such as altered brain waves or heightened blood pressure, the following taxonomies were based on what is emphasized in the current understanding of the etiology. Similarly, the diseases we categorized as somatic may well involve a change in individual behavior and psychological well-being, but neither of them is assumed to originate in the psyche. This left us with a handful of diseases/conditions that are less easily confined under these two labels, and they made out the ambiguous class.
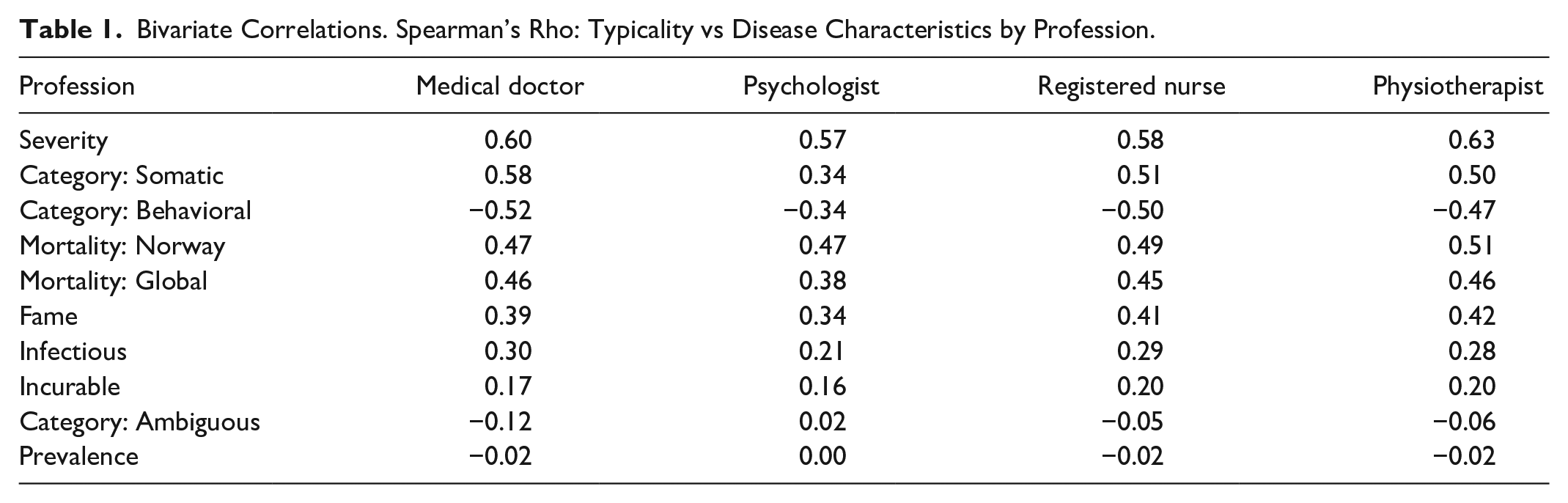
Given non-normal distributions, we report Spearman’s rank order correlation coefficients. Correlations between perceived typicality for each respondent and disease characteristics were transformed using Fisher’s Z transformation for the purpose of averaging across respondents. Table 1 displays the inverted Z-transformed average correlations.
Bivariate Correlations. Spearman’s Rho: Typicality vs Disease Characteristics by Profession.
In order to assess the combined impact of disease characteristics on typicality we conducted mixed effects multilevel regression analyses 47 using the lme4 package. 48 We estimated several models with varying intercepts for each respondent and disease. This was done in order to account for dependency in the data, since each typicality score can be considered to be nested within diseases and respondents. The regression coefficients for the disease characteristics are assumed to be the same across respondents and diseases. Models were fitted using restricted maximum likelihood, and model diagnostics were checked using the performance package. 49 Some variables were strongly right skewed (mortality, prevalence, fame), and these were log transformed prior to running the regressions.
Finally, in order to inspect non-linear relationships among the strongest predictors, we plotted mean typicality scores (separately for each profession) versus severity, by disease category and mortality.
Results
The role of occupational background and disease category
Table 2 shows the impact of disease category on perceived typicality among different professional groups (research question 1). All professionals considered somatic conditions to be more typical as diseases than psychological/behavioral conditions, with the ambiguous category in between. There was also evidence of an interaction effect, such that different professions rated different categories of disease as most typical. On average MDs considered somatic conditions to be more typical diseases than any other professions. Psychologists on the other hand considered both the psychological/behavioral conditions, as well as those falling in the ambiguous category, to be more typical than any other profession. Figure 2 shows a graphical illustration of perceived typicality according to category and profession.
Mean Typicality of Diseases and Standard Deviation by Profession and Broad Disease Category.


Mean typicality of diseases by profession and category.
To test whether different professions consider different broad categories of disease to be more or less typical, a two-way ANOVA was run with factors of Profession (4 levels, between-subjects) and Disease Category (3 levels, somatic, psychological/behavioral, and ambiguous, within-subjects). The main effect of Profession was not significant (F(3,140) = 2.05, P = .11, ηp2 = .042). The effect of Disease Category was strong (F(2,280) = 464.4, P < .001, ηp2 = .768), with somatic diseases (M = 7.84, SD = .95) more typical than ambiguous (M = 5.79, SD = 1.51) which in turn were more typical than psychological/behavioral conditions (M = 3.66, SD = 1.30).
Interestingly, the interaction between the factors was significant (F(6,280) = 5.97, P < .001, ηp2 = .113), as seen in Figure 2. The source of the interaction was the group of psychologists, who judged the psychological/behavioral and ambiguous disease categories to be clearly more typical than did the other groups. In confirmation, a rerun of the ANOVA without the psychologist group led to the interaction ceasing to be significant (F(4, 258) = 2.19, P = .071, ηp2 = .033).
Differences between professions across different individual diseases
Research question 2 asked whether, given the difference between professions in how typical broad categories of disease were seen (see above), is it possible to look in more detail at where the professional groups differed most strongly?
A MANOVA analysis with the four professions (MD, RN, Psychologist, and Physiotherapist) as the Independent factor and the rated typicalities of the 61 diseases within each profession as dependent variables confirmed a significant effect of Profession, with partial η2 (similar to R2) of .58 using Wilks Lambda. Over half the diseases (about 38) showed significant univariate effects of profession (P < .05). It thus appears that respondents generally agree on which diseases are typical vs non-typical, but disagree on how typical the psychological/behavioral diseases should be understood. Profession seems to explain parts of this variation.
Linear discriminant analysis (LDA) takes a set of measures (in this case the rated typicality of diseases for each respondent) and aims to construct a set of dimensions (as linear functions of the measures) that will enable one to predict which profession a person belongs to, based on their judgments. In the case of our professional groups, three independent functions were created, placing each individual in a 3D space, with clusters in the space corresponding to each of the four professions. The functions were optimal in maximizing the distance between members of different groups and minimizing distance within groups. The aim was to see how well the analysis would be able to separate the professions. This was done by leaving each respondent out of the analysis in turn and predicting their professional group based on functions calculated from the remaining data (a cross-validation, or jack-knife procedure). A fully successful analysis would predict the correct professional group for each individual, just based on their judgments of typicality.
To avoid over-fitting of the model, a stepwise procedure was employed, adding in diseases to the analysis one at a time until no significant improvement in fit was seen. Two functions were significant and captured 97% of the variance. Figure 3 shows how the individual respondents were clustered on these functions. Function 1 distinguished between the psychologists and doctors to the right and the other professional groups to the left. Function 2 then differentiated psychologists from the rest. The cross-validated classifications showed that 62% of doctors, 84% of nurses and 58% of psychologists were correctly predicted to fall in their respective groups. In contrast, none of the physiotherapists were correctly classified as such, with 86% predicted to be nurses, and 14% to be doctors.

Plot showing individual professionals mapped on the first two functions of the linear discriminant analysis.
Disease characteristics associated with typicality
Research question 3 concerned how disease characteristics correlate with perceived typicality. Table 1 shows how various characteristics of the diseases correlated with perceived typicality for the different professions. In general, the correlations in Table 1 differed little between professions, with correlations among psychologists somewhat lower on most of the characteristics.
We observed a moderate to strong positive correlation between the typicality scores and severity, category of disease, and mortality (national and global). There was also a low to moderate positive correlation between typicality and fame and infectiousness. There was no correlation between typicality and prevalence, and only a small positive correlation with respect to whether the condition is incurable. Finally, typicality scores showed a strong negative correlation with whether the condition is categorized as psychological/behavioral.
Figure 4 shows plotted coefficients from the full hierarchical model (see Appendix B for coefficients). The plot shows the standardized regression coefficients for comparison between predictors and confirms the strong effect of severity and mortality on typicality.

Plotted coefficients from hierarchical linear model.
Table 1 and Figure 4 show that severity was the strongest predictor of disease typicality, with correlations of around 0.6 within each profession. To understand this effect, Figure 1 shows a scatter plot of average typicality vs severity, grouped by disease category and mortality. The colors differ by disease category and display the patterns clearly. Somatic diseases, in black are seen to be more typical than ambiguous diseases, in yellow, which were more typical than psychological/behavioral ones in blue. All categories of disease showed a similar relation between severity and typicality. Above a severity of 0.2 on the scale, typicality was not correlated with severity. Below this level of severity, there was a wide range of typicalities, and almost all diseases with lower typicality (<5) were at the least severe end of the scale. Virtually all of these atypical diseases are either psychological/behavioral, or are related to sex or reproducibility: pregnancy, menopause, PMS, miscarriage and infertility.
The effect of severity on typicality can be captured by noting the absence of any diseases in the lower right quadrant. Typical diseases could vary in severity across the whole scale, but there were no atypical severe diseases. If a disease was severe, it scored at least 4.5 on the typicality scale, and if a disease was atypical it scored less than 0.2 on the severity scale.
Discussion
In this study we considered three research questions. First, we considered how the four groups of MD, RN, physiotherapists and psychologists differed in their perceptions of disease typicality. Here we found that while there was a high level of consensus across groups, there were many diseases where differences appeared. In an overall analysis, we identified the key difference as relating to either fully or ambiguously psychological/behavioral conditions, which were rated as more typical by the psychologists in comparison to the other groups.
One explanation for the fact that psychologists consider psychological diseases to be far more typical than other professions, while medical doctors are more likely to perceive somatic conditions as more typical, is that members of these professions are more frequently exposed to individuals exhibiting these problems, both from clinical experience and from the literature. Regardless of explanation, the difference is striking and could influence the way patients with various diseases are met and treated, depending on the profession of the therapist. However, there were only 13 psychologists in the sample, which urges cautiousness with making strong claims of an effect that is generalizable beyond the sample. Moreover, the generally lower typicality of psychological/behavioral diseases for other professions may also be related to the low prestige of these diseases among professionals.29,30
The second research question concerned whether the profile of a professional’s typicality judgments was sufficient to identify their professional background. Using LDA we were able to show that a substantial majority of the MD, RN and psychologist groups could be differentiated on the basis of their typicality judgments. RNs were a particularly well-clustered group. However, physiotherapists were almost completely contained within the RN group cluster. It is interesting how MDs had a very distinct view of disease typicality compared to the RN and physiotherapist groups, which themselves did not differ.
The third and final research question asked what characteristics of diseases lead them to being considered typical. The professional groups hardly differed in which characteristics were most predictive. In addition to the already described effect of somatic versus non-somatic diseases, the most important aspect of a disease driving typicality was its severity, followed by mortality and infectiousness. Curability turned out to have only a low correlation with typicality.
A closer look at how severity affected typicality revealed that the only diseases considered atypical tended to have low severity. Put another way, any disease that was above a certain threshold of severity was considered more or less typical. This pattern suggests that, logically, severity is a sufficient (but not necessary) condition for a disease to be considered typical.
Another characteristic—fame—was poorly correlated with typicality. This fact may in part be due to the inclusion of concepts such as pregnancy, homosexuality and nostalgia, which are not typically considered diseases, but often show up in the media. The search terms used for measuring this variable required the inclusion of additional terms like disease, sickness or illness. Still they are likely to include articles where the terms are not understood as diseases.
There are of course many ways to categorize diseases. For example, whether they are chronic is, no doubt, an important characteristic. While we had included chronicity as a characteristic, we abandoned it in the end. One reason was that it overlapped with incurability. Moreover, there exist many definitions of chronicity that are quite different in scope.
It is also noteworthy that conditions related to female reproduction, such as infertility, miscarriage, pregnancy, PMS, and menopause came out low in typicality although most of them are characterized as somatic. Hence, there may be a gender issue to address in further research.
Measures of disease characteristics such as mortality and prevalence were collected in July 2019 and represent global numbers for 2010. Clearly, updated estimates are likely to become available later. However, our ambition was to identify general trends in correlations, rather than specific magnitude, so minor deviations are not likely to have a significant impact.
It is also very important to acknowledge that this study was performed in a specific cultural setting. The results are by no means generalizable to an Asian or African setting. Here we can only encourage other researchers to supplement our study. In a similar vein, it would be interesting and informative to learn how the typicality of diseases is understood by people who are not health professionals.
Conclusion
The conclusions of the research were, first, that while different health professions agreed well on which diseases are typical, their judgments could also be clearly differentiated. Psychologists, naturally, considered psychological/behavioral conditions to be more typical, but in addition, MDs could be distinguished from RN and physiotherapists by their profile of disease typicality judgments. The second conclusion was that looking at a number of disease characteristics that may influence typicality, there were two that stood out. The involvement of somatic disease clearly raised typicality over either partly or fully psychological/behavioral conditions, and there was a strong relation between severity and typicality, such that any severe disease would necessarily be considered typical, while any atypical disease would necessarily be non-severe. Hence, studying how different disease characteristics and occupational background influences health professionals’ perception of disease typicality is the first and crucial step toward a more general study of how typicality influences disease handling.
Supplemental Material
sj-docx-2-inq-10.1177_0046958020972813 – Supplemental material for What Makes Some Diseases More Typical than Others? A Survey on the Impact of Disease Characteristics and Professional Background on Disease Typicality
Supplemental material, sj-docx-2-inq-10.1177_0046958020972813 for What Makes Some Diseases More Typical than Others? A Survey on the Impact of Disease Characteristics and Professional Background on Disease Typicality by Tore Hofstad, James A. Hampton and Bjørn Hofmann in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-1-inq-10.1177_0046958020972813 – Supplemental material for What Makes Some Diseases More Typical than Others? A Survey on the Impact of Disease Characteristics and Professional Background on Disease Typicality
Supplemental material, sj-xlsx-1-inq-10.1177_0046958020972813 for What Makes Some Diseases More Typical than Others? A Survey on the Impact of Disease Characteristics and Professional Background on Disease Typicality by Tore Hofstad, James A. Hampton and Bjørn Hofmann in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Authors’ Note
Data are available in appendixes and further information on request. No patients were involved in this study and no patient consent was applied. All data are anonymous, and no ethics approval was necessary for collecting anonymous data in Norway. Participants were informed about the study and consented by filling in the questionnaire.
Author Contributions
BH designed the questionnaire and collected the data. TH and BH designed this study and TH gathered data for analysis parameters. TH designed the data analysis and performed these in collaboration with JH. BH made the first draft of the manuscript. TH, JH and BH revised the manuscript in several rounds. All authors have approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TH and BH received no financial support for the research, authorship, and/or publication of this article. JH has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme grant agreement Nos. 681422 and 742204.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.