
Abstract
School nurses are integral to creating safe environments in U.S. schools. Many experienced increased work burden and stress during the COVID-19 pandemic. CDC collaborated with the National Association of School Nurses and the National Association of State School Nurse Consultants to distribute a 121-item online, anonymous survey to school nurses nationwide during March 7-30, 2022. Among the 7,971 respondents, symptoms of depression, anxiety and PTSD, and suicidal ideation were measured, and prevalence ratios were used to identify associations with demographics, workplace characteristics, and support. Results found high levels of work-related stressors and indicated that employment characteristics, COVID-19-related job duties, and other workplace stressors and supports affected school nurse mental health. The survey findings underscore the mental health challenges many school nurses experienced during the 2021/2022 school year. The findings can inform supportive policies and practices to reduce workplace stressors and increase workplace supports for school nurses.
Keywords
Introduction
School nurses support student health and academic success through case finding, nursing care procedures, care coordination, leadership, health education, and emergency care (Council on School Health, 2016; Maughan et al., 2016 NASSNC, 1996) and have been integral to creating safe environments in the nation's schools during the COVID-19 pandemic. School nurses are the health care representatives on site at schools, and they serve as liaisons between school personnel, families, health care professionals, and the community (Council on School Health, 2016; Maughan et al., 2016). School nurses experienced increased work burden and stress as the COVID-19 pandemic presented unprecedented challenges to the pre-Kindergarten through grade 12 (preK-12) education system (NASEM, 2020).
In response to the pandemic, schools have implemented COVID-19 layered prevention strategies that have included necessary interventions but have also increased the workload of school staff, including nurses (Science Brief, 2021). Workplace demands and new, unfamiliar tasks, such as COVID-19 testing, caring for staff and students suspected of having COVID-19, and contacting parents/guardians about COVID-19 isolation and quarantine recommendations, coupled with concern for their own health and that of their families, students, and co-workers has the potential to increase stress, anxiety, and burnout of school nurses (Galanis et al., 2021; Golonka et al., 2019). Workplace demands and new, unfamiliar, tasks also could affect the mental health of the approximately 100,000 school nurses in the United States (Willgerodt et al., 2018) and adversely affect their job performance (CDC, 2018). These additional burdens and accompanying health impacts have the potential to interfere with school nurses’ roles providing healthcare to students, ensuring quality improvement in school health services, and acting as leaders within their schools and surrounding communities (NASN, 2016).
Data on the mental health of school nurses before and during the COVID-19 pandemic are limited. Despite the important role school nurses have in supporting the health of children and communities, this is the first nationwide effort to evaluate the impact of the COVID-19 pandemic on their mental health. Other researchers have assessed the impact of the COVID-19 pandemic on mental health among the overall U.S. population (Czeisler et al., 2020; Ettman et al., 2020; Vaharatian et al., 2021; Zhu et al., 2021), as well as some targeted populations, including healthcare (Gainer et al., 2021, Li et al., 2021), public health (Bryant-Genevier et al., 2021), and other frontline and ‘essential’ workers (Rosemberg et al., 2021). Seventy-seven percent of school nurses are funded by local school districts rather than health departments or healthcare systems (Willgerodt et al., 2018), so school nurses may not be represented in surveys about the mental health of public health workers or healthcare workers.
The purpose of the investigation was to examine associations between stressors and protective factors among school nurses during the COVID-19 pandemic and symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD), and suicidal ideation.
Methods
To assess the current mental health of school nurses and better understand their experiences during the COVID-19 pandemic, CDC collaborated with the National Association of School Nurses (NASN) and the National Association of State School Nurse Consultants (NASSNC). A 121-item, nonprobability-based, anonymous survey was developed by the authors and distributed by NASN and NASSNC to school nurses nationwide from March 7-30, 2022. The 15-min, online survey was revised from a Spring 2021 survey on the mental health of people working in state and local public health departments (Bryant-Genevier J et al., 2021). The survey included questions on demographics, experiences, stressors, coping strategies, supports, and self-reported mental health symptoms. Anyone who worked as a school nurse in a public or private school in the United States or in a U.S. tribe or territory during the 2021/2022 school year was eligible to take the survey. NASN emailed a link to the survey to their 9,478 current members, and 59% (5,592) opened the email. NASSNC distributed the survey to their 75 state/regional current and retired school nurse consultant members and requested they distribute it to school nurses in their state/region.
Symptoms of mental health conditions were evaluated by including in our survey the 9-item Patient Health Questionnaire (PHQ-9) for depression (Kroenke et al., 2001), the 2-item General Anxiety Disorder (GAD-2) for anxiety (Kroenke et al., 2007), the 6-item Impact of Event Scale (IES-6) for PTSD (Thoresen et al., 2010), and one item of the PHQ-9 for suicidal ideation. The PHQ-9, GAD-2, and IES-6 responses are based on the two weeks prior to the survey. Those who scored ≥10.0 out of 27 on the PHQ-9 were categorized as having symptoms of moderate to severe depression. Scores ≥3.0 out of 6 on the GAD-2 were categorized as having symptoms of anxiety. Scores ≥1.75 out of 4 on the IES-6 were classified as having symptoms of PTSD. Respondents who indicated on a PHQ-9 question they had been “bothered by thoughts that you would be better off dead or thought of hurting yourself” at any time in the past two weeks were categorized as experiencing suicidal ideation.
Prevalence of symptoms of mental health conditions and suicidal ideation were calculated and examined by demographic and workplace characteristics, work-related stressors and supports, and U.S. Department of Health and Human Services regions. Univariable and multivariable prevalence ratios were calculated using Poisson regression with 95% confidence intervals estimated using a robust standard error. Confidence intervals for regional prevalence rates were calculated using robust standard error. Missing responses were excluded from all frequency and prevalence calculations. Survey data were collected using REDCap (Harris et al., 2009). Analyses were completed using R (version 4.1.1; R Core Team, 2021), RStudio (version 1.4.1717; RStudio Team, 2021b18), the tidyverse packages (Wickham et al., 2019), geepack (Højsgaard et al., 2006), and gtsummary (Sjoberg et al., 2021). This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy (e.g., 45 C.F.R. part 46.102(l)(2), 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.).
Results
School nurse demographics and workplace characteristics, and associations with mental health outcomes, along with point estimates and 95% confidence intervals are presented in Table 1. The 7,971 survey respondents were from all 50 states, the District of Columbia, tribal nations, and U.S. territories. Among respondents, 98.6% percent were female, 92.0% were White, 86.8% worked at a public school, and 80.2% were Registered Nurses. More than a third (34.5%) reported working in schools where at least 76% of students qualified for free or reduced lunch programs, and more than half (56.0%) reported working more than 40 hours per week during the 2021/2022 school year. Among respondents, 44.8% reported symptoms of at least one adverse mental health condition in the two weeks prior to completing the survey. Among respondents, prevalences of symptoms of moderate to severe depression, anxiety and PTSD, and suicidal ideation were 23.9%, 22.2%, 30.4%, and 4.3% respectively. Some respondents did not respond to the full series of questions about symptoms of depression (12.4%), symptoms of anxiety (11.4%), symptoms of PTSD (14.8%), and suicidal ideation (11.3%). An analysis was conducted examining the prevalence of multiple mental health outcomes and found of the 6,687 school nurse respondents who answered the full series of questions for all mental health outcomes for this study, 23.1% reported symptoms of two or more mental health outcomes (data not shown). Respondents working over 40 hours per week reported a greater prevalence of symptoms of depression, anxiety and PTSD, and suicidal ideation. Nurses of Hispanic or Other race/ethnicity (defined in Table 1), those who indicated they were assigned 750 students or more, and those who worked in schools where more than 75% of students qualified for free or reduced lunch programs were more likely to report symptoms of depression.
Demographics and Workplace Characteristics and Prevalence of Symptoms of Depression, Anxiety and PTSD, and Suicidal Ideation among PreK-12 School Nurses in the United States During the 2021/2022 School Year (n = 7,971)
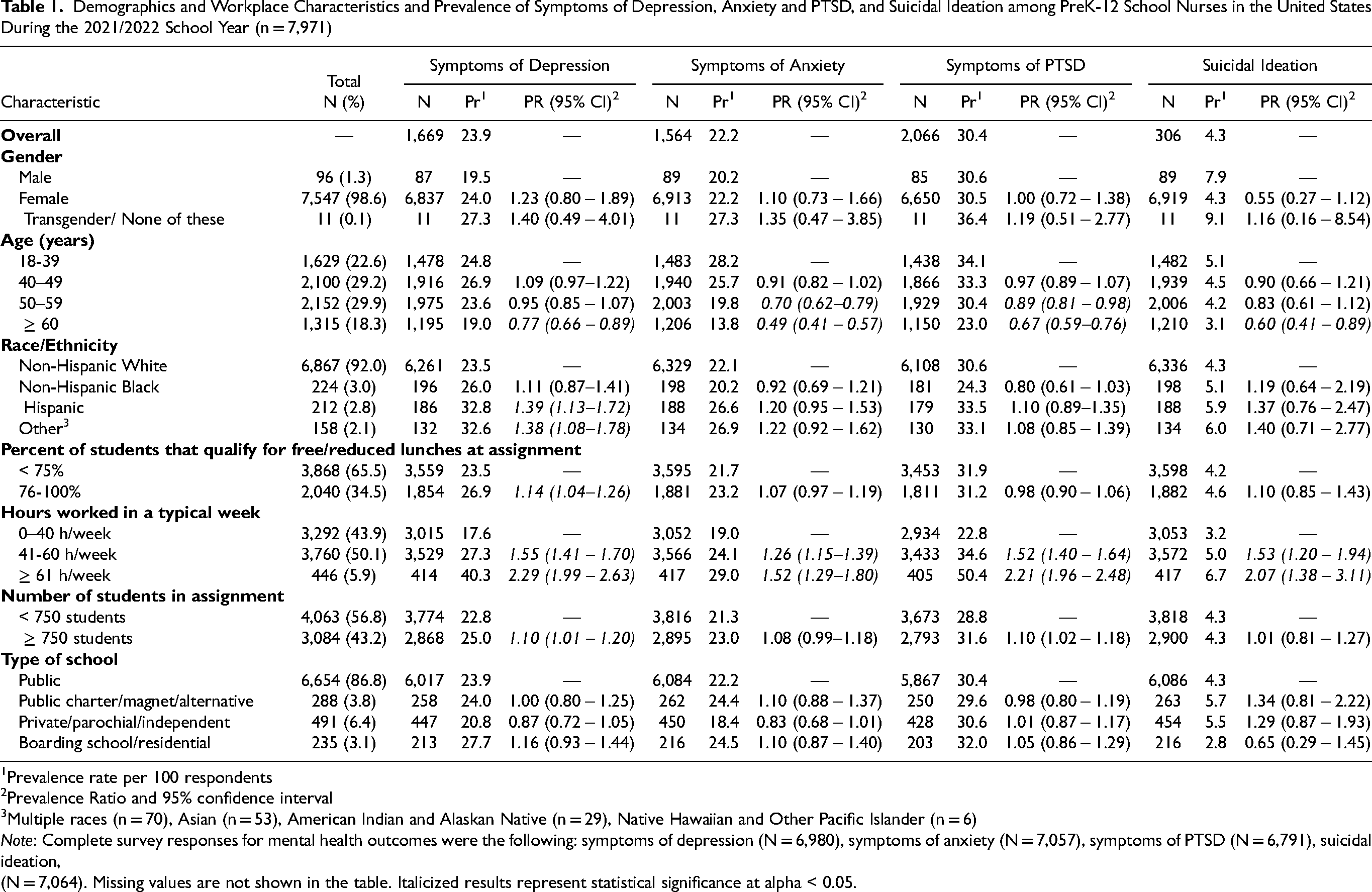
Prevalence rate per 100 respondents
Prevalence Ratio and 95% confidence interval
Multiple races (n = 70), Asian (n = 53), American Indian and Alaskan Native (n = 29), Native Hawaiian and Other Pacific Islander (n = 6)
Note: Complete survey responses for mental health outcomes were the following: symptoms of depression (N = 6,980), symptoms of anxiety (N = 7,057), symptoms of PTSD (N = 6,791), suicidal ideation, (N = 7,064). Missing values are not shown in the table. Italicized results represent statistical significance at alpha < 0.05.
Table 2 presents school nurses’ workplace stressors and associations with the prevalence of mental health outcomes, along with prevalence ratios and 95% confidence intervals. During the 2021/2022 school year, 93.2% of school nurses reported having notified parents about children's COVID-19 positive test results and close-contact exposures, 83.0% cared for students, teachers, and staff who were suspected of having COVID-19, and 48.0% administered COVID-19 tests. Since the beginning of the COVID-19 pandemic in March 2020, 82.4% of nurses felt inadequately compensated for their work, 64.0% felt unappreciated at work, 72.7% worried about workplace exposure to COVID-19, 38.6% reported experiencing stigma or discrimination due to their work, 23.8% reported receiving job-related threats, and 48.3% reported having felt bullied, threatened, or harassed due to their work. Respondents who reported they felt inadequately compensated for their work, felt unappreciated at work, or worried about workplace exposure to COVID-19 were more likely to report symptoms of depression, anxiety, PTSD, or suicidal ideation than those who did not. Lastly, nurses who reported stigma or discrimination, received job-related threats, or felt bullied, threatened and/or harassed due to their work were more likely to report symptoms of depression, anxiety, PTSD, or suicidal ideation than those who did not. Nurses who notified parents/guardians about positive COVID-19 tests or close-contact exposures and isolation or quarantine guidelines, and who cared for students, teachers and staff who were suspected of having COVID-19 were significantly more likely to report symptoms of depression, anxiety and PTSD. Nurses who reported administering COVID-19 tests reported a greater likelihood of symptoms of anxiety and PTSD.
Workplace Stressors and Prevalence of Symptoms of Depression, Anxiety and PTSD, and Suicidal Ideation PreK-12 School Nurses in the United States During the COVID-19 Pandemic (n = 7,971)
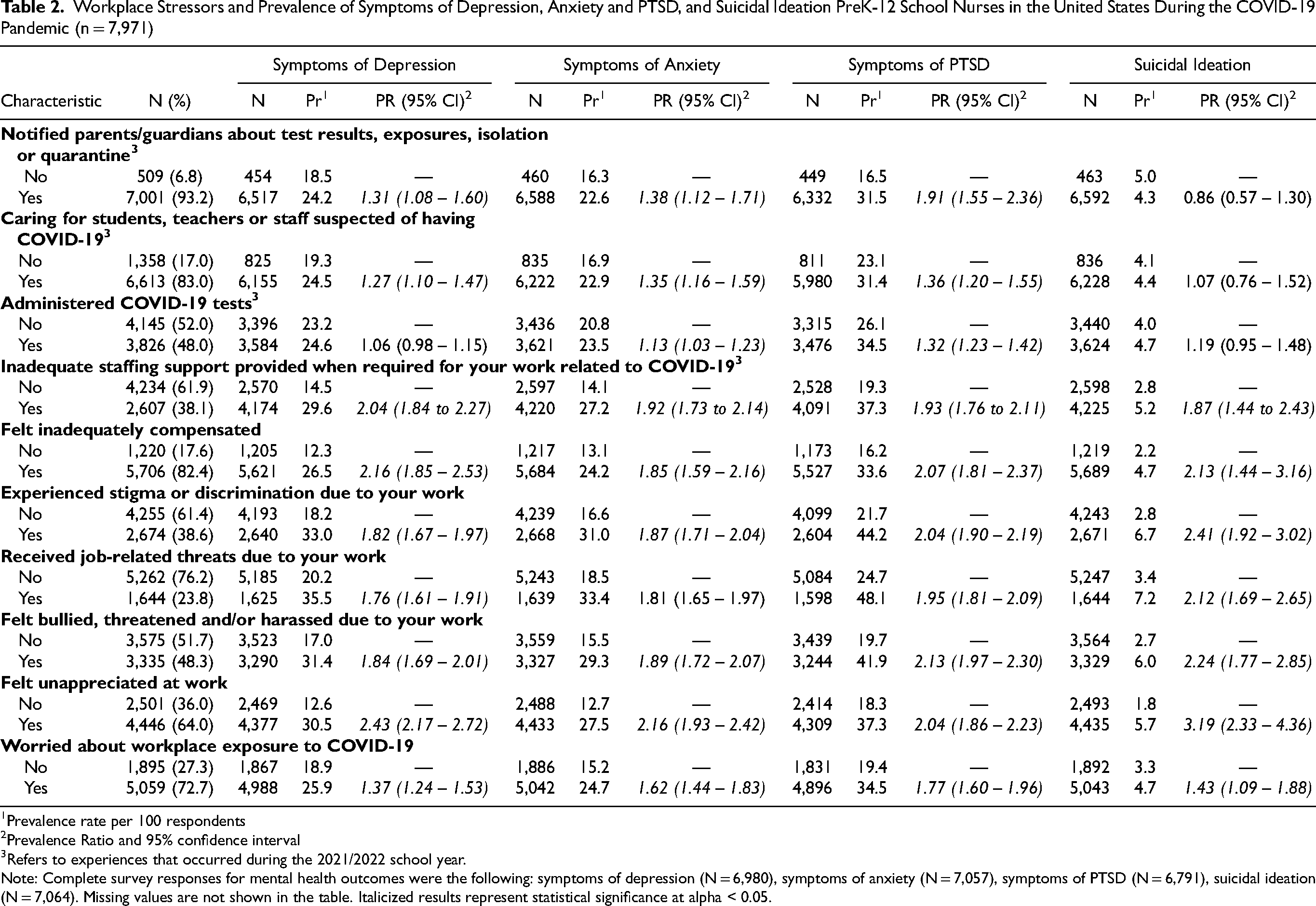
Prevalence rate per 100 respondents
Prevalence Ratio and 95% confidence interval
Refers to experiences that occurred during the 2021/2022 school year.
Note: Complete survey responses for mental health outcomes were the following: symptoms of depression (N = 6,980), symptoms of anxiety (N = 7,057), symptoms of PTSD (N = 6,791), suicidal ideation (N = 7,064). Missing values are not shown in the table. Italicized results represent statistical significance at alpha < 0.05.
Table 3 presents school nurses’ workplace supports and associations with the prevalence of mental health outcomes, along with the prevalence ratios and 95% confidence intervals. Among respondents, since the beginning of the 2021/2022 school year, 67.6% of school nurses felt supported always or most of the time by their coworkers/peers, 60.9% by their supervisor, and 41.5% by their school district leadership. Additionally, 54.5% reported that their employer offered an Employee Assistance Program (EAP) or a similar program, 58.2% agreed with how their management, employer or organization responded to the risk of COVID-19 exposures at work, 27.4% reported that their workplace/employer offered training to prevent stress or burnout, 18.7% reported that their workplace/employer offered a flexible work schedule, and 38.1% reported that adequate staffing support was provided when required for their work related to COVID-19. School nurses who responded that they were supported always or most of the time by their coworkers/peers, supervisor, or school district leadership were less likely to report symptoms of depression, anxiety or PTSD, or suicidal ideation than those who reported they were not at all or were somewhat supported. Nurses who reported they agreed with how their management, employer or organization responded to the risk of COVID-19 exposure at work, and those who reported that adequate staffing support was provided for work related to COVID-19 were less likely to report symptoms of depression, anxiety or PTSD, or suicidal ideation than those who did not. Respondents who reported their workplace/employer offered training to prevent stress or burnout or who reported their workplace/employer offered a flexible work schedule were less likely to report symptoms of depression, anxiety or PTSD than those who did not.
Workplace Support and Prevalence of Symptoms of Depression, Anxiety and PTSD, and Suicidal Ideation among PreK-12 School Nurses in the United States During the 2021/2022 School Year (n = 7,971)
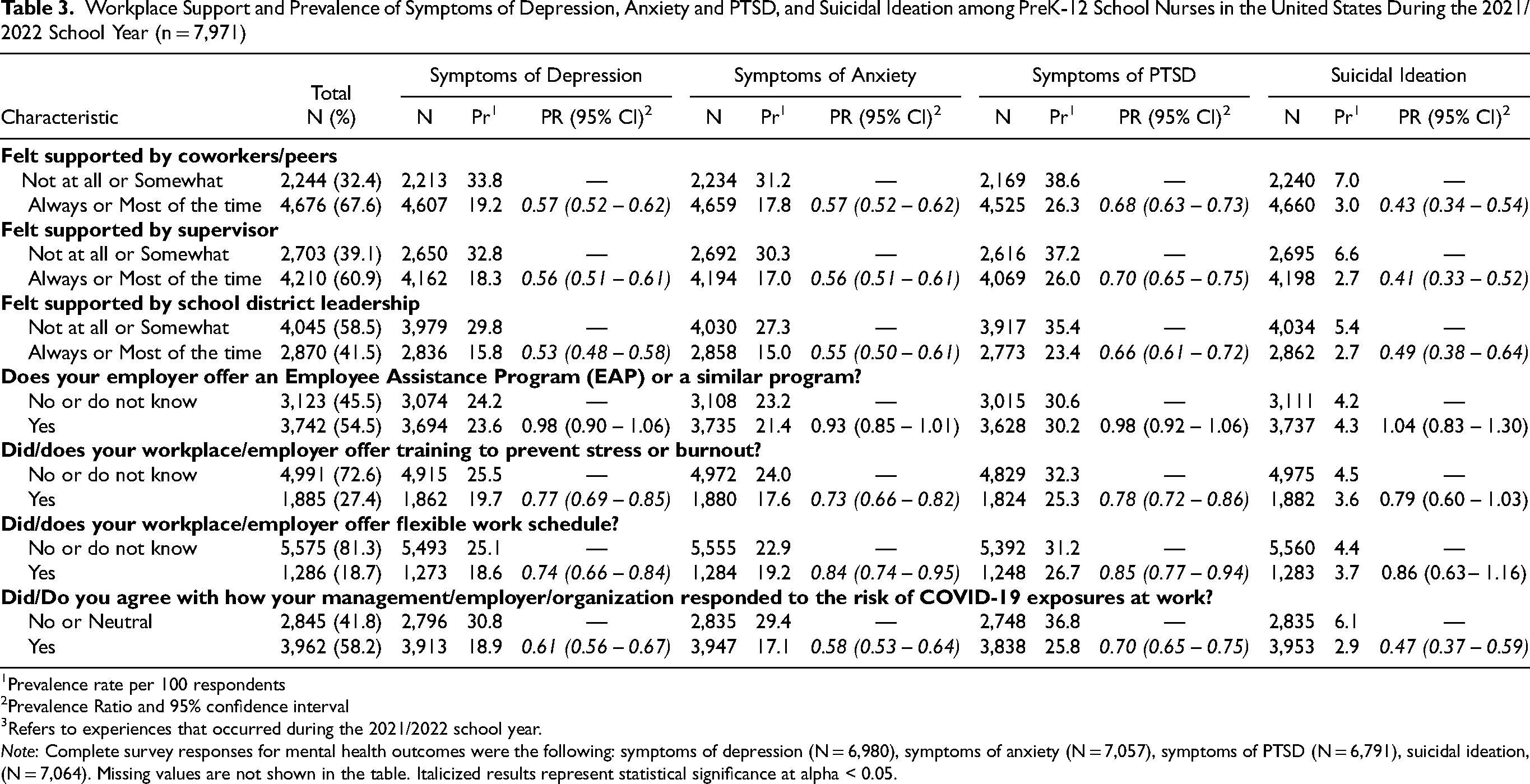
Prevalence rate per 100 respondents
Prevalence Ratio and 95% confidence interval
Refers to experiences that occurred during the 2021/2022 school year.
Note: Complete survey responses for mental health outcomes were the following: symptoms of depression (N = 6,980), symptoms of anxiety (N = 7,057), symptoms of PTSD (N = 6,791), suicidal ideation, (N = 7,064). Missing values are not shown in the table. Italicized results represent statistical significance at alpha < 0.05.
Figure 1 illustrates the prevalence of mental health outcomes by U.S. Department of Health and Human Services regions
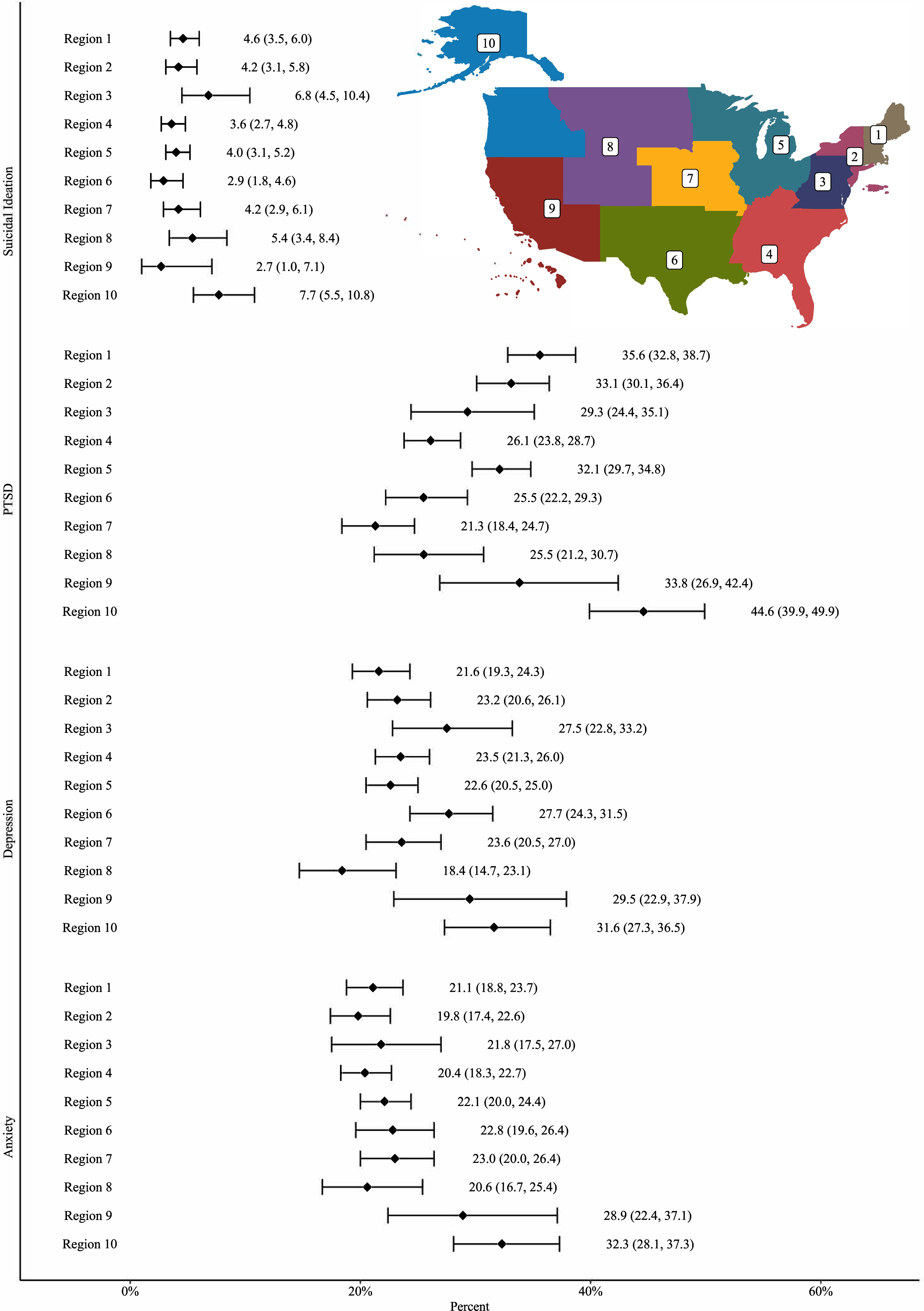
Prevalence* of symptoms of depression, anxiety and post-traumatic stress disorder, and suicidal ideation among preK-12 school nurses in the U.S. during the 2021/2022 school year by U.S. Department of Health and Human Services regions. *Prevalence rate per 100 individuals and 95% confidence interval. Note: Complete survey responses for mental health outcomes were the following: symptoms of depression (N=6,980), symptoms of anxiety (N=7,057), symptoms of PTSD (N=6,791), suicidal ideation, (N=7,064). Region 1: CT, ME, MA, NH, RI, and VT, Region 2: NJ, NY, PR, and VI, Region 3: DE, DC, MD, PA, VA, and WV, Region 4: AL, FL, GA, KY, MS, NC, SC, and TN, Region 5: IL, IN, MI, MN, OH, and WI, Region 6: AK, LA, NM, OK, and TX, Region 7: IA, KS, MO, and NE, Region 8: CO, MT, ND, SD, UT, and WY, Region 9: AZ, CA, HI, NV, AS, MP, FM, GU, MH, and PW, Region 10: AK, ID, OR, and WA.
Discussion
This study presents a novel investigation of a critical issue impacting a key workforce in the COVID-19 response effort. There has been consensus among population surveys examining mental health outcomes among U.S. adults, finding increases in the prevalence of symptoms of depression, anxiety, and suicidal ideation during the COVID-19 pandemic (Ettman et al., 2020, Vahratian et al., 2021). Some similarities and differences are apparent when comparing the prevalence of mental health outcomes among school nurses to other U.S. adults during the COVID-19 pandemic. The overall prevalence of symptoms of mental health conditions among school nurses in this study (45%) was higher than the 40.9% previously reported in the general population in June 2020 (Czeisler et al., 2020) but lower than the 52.8% previously reported among public health workers in March-April 2021 (Bryant-Genevier et al., 2021)
The findings align with other analyses that demonstrated nurses have been faced with adverse working conditions during the COVID-19 pandemic. In a previous study on school nurses’ reports on reopening roles, practices, and concerns during the COVID-19 pandemic at the start of the 2020/2021 school year, over one-third (36.9%) reported not being included in school reopening planning, and only one quarter reported that their school had an isolation space suitable and ready for students with COVID-19 symptoms waiting to leave school (Gormley et al., 2021). A meta-analysis of nurse burnout during the COVID-19 pandemic found similar results that some associated risk factors included increased workload, low levels of COVID-19 training, increased working times and number of patients (Galanis et al., 2021).
Among the study population, there was an evident theme that suggested greater support of school nurses is warranted from a leadership level. Not feeling supported by leadership, not agreeing with the response to how the risk of COVID-19 exposure was handled, not being supported with adequate staff, working long hours, feeling unappreciated, and feeling inadequately compensated were all reported by the majority of respondents and were all significantly associated with all mental health outcomes examined. Having access to an employee assistance program or similar program was not associated with the mental health outcomes examined. It is uncertain if this was based on limited utilization, lack of awareness, or other limitations within the structure of the programs offered.
This work represents a timely and important topic among a key workforce that has been essential to the COVID-19 response. The mental health outcome measures have been validated and widely used in other mental health investigations. A large number of school nurses responded to the survey, with representation from all states and some territories and tribes. School nurses who responded to our survey had similar demographics as compared to previous published estimates of school nurses nationwide (Willgerodt et al., 2018). The findings highlight opportunities to improve supportive policies and practices to reduce workplace stressors and increase workplace supports for school nurses.
The findings in this report are subject to several limitations. A nonprobability-based convenience sample of school nurses was used, and a completion rate could not be determined. Though strict tests of generalizability were not performed, the 7,971 survey respondents were from all 50 states, the District of Columbia, tribal nations, and U.S. territories and present similar demographic characteristics to other assessments of school nurses in the United States (Willgerodt et al., 2018). Second, self-reported mental health symptoms were assessed using screening instruments that do not provide clinical diagnoses; however, the screening instruments have been clinically validated (Kroenke et al., 2001, 2007; Thoresen et al., 2010). Third, participants were surveyed about symptoms experienced in the two weeks preceding the survey, which may not reflect all symptoms experienced during the pandemic. Pre-pandemic mental health conditions were not available for comparison. Fourth, between 11.3% and 14.8% did not respond to the full series of questions about mental health outcomes. Finally, some other stressors or events experienced by school nurses were not assessed by the survey, such as being diagnosed with COVID-19 or experiencing changes in COVID-19 prevention strategies at their school (e.g., masking requirements).
Future quantitative analyses could explore additional stressors or protective factors that were included in this survey but were not part of this analysis. Further effort is needed to identify factors contributing to the disparity in reported symptoms of depression between nurses of Hispanic or Other race/ethnicity and their White counterparts. Future investigations could look at the relationship between different types and numbers of stressors and protective factors and the mental health outcomes among school nurses. Additionally, future efforts could explore factors that increase successful utilization of EAP programs, how workplace stressors could be reduced, and how mental health and well-being could be promoted.
School districts, schools, and others could consider various strategies to support school nurse mental health. Leadership could provide principals and school nurse managers with training to help them recognize the signs and symptoms of stress and depression in team members and encourage them to seek help from qualified mental health professionals. Leadership's focus on appropriate work hours and staffing is also critical for school nurses. Leadership could also provide free or subsidized lifestyle coaching, counseling, or self-management programs and offer workplace training to prevent stress or burnout during work time, perhaps during designated school staff professional development days. Resiliency training, support groups, skill building to defuse tense situations, virtual and distance learning could also be offered. School nurses could be consulted about decisions that affect their job and stress levels and given the opportunity to advise decisions. Adopting layered strategies that promote prioritization of school nurse mental health may influence the social norms around mental health more broadly (CDC, 2018; Maughan et al., 2016; NASSNC, Personal Communication, March 2022).
Conclusion
The goal of this study was to assess school nurse mental health during the COVID-19 pandemic. The survey findings underscore the personal mental health challenges many school nurses experienced during the 2021/2022 school year. Results highlight employment characteristics, COVID-19-related job duties, and other workplace stressors and supports that affected school nurse mental health. While significant association between workplace support and stressors, and mental health outcomes during the pandemic were identified, it is important to recognize that there is no baseline data on school nurse mental health prior to the pandemic. Many of these factors may have been present before the pandemic and may remain as the pandemic subsides.
Implementing prevention and control policies and practices that reduce factors that contribute to school nurses’ poor mental health might improve mental health outcomes. Tools and strategies to recognize burnout and mental health symptoms could be provided for school nurses. The findings may inform national, state, and local education and public health agencies on supportive policies and practices to reduce workplace stressors and increase workplace supports for school nurses. Supportive policies and practices could include adequate staffing, training and support, particularly as they relate to COVID-19 or future public health emergencies.
Footnotes
Acknowledgments
CDC: Katherine Bruss, Ramona Byrkit, Melissa Fahrenbruch, LaShonda Hall, Sarah Lee, Nicole Liddon, Barbara Lopez-Cardozo, Sanja Papati, Catherine Rasberry, Craig W. Thomas, Jorge Verlanden, CDC COVID-19 Response Team and the State, Tribal, Local, and Territorial Support Task Force; National Association of School Nurses: Elizabeth Clark, Donna Mazyck, Carol Walsh; National Association of State School Nurse Consultants: Marjorie Cole, Ann O. Nichols, Emily Poland, Janice Selekman, Linda Wolfe
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article