
Abstract
Although Slovenia is becoming an aging society, very little is known about the abilities and needs of home-dwelling older people or their preferences regarding assistance. The aim of the study was to explore the need for assistance in daily activities among older Slovenian people living at home. Older adults aged between 65 and 97 years (N = 358) participated in the cross-sectional survey study. A questionnaire that assessed independence in daily activities and assistance in the home environment was developed. Data were analyzed using descriptive statistics, a nonparametric test (Wilcoxon signed rank test), and the chi-square test. The results showed that older Slovenians were more independent in activities of daily living (ADLs) than instrumental activities of daily living (IADLs). Independence was the highest for using the toilet, feeding, and mobility transfers, and the lowest for bathing. With IADLs, assistance was most often required with shopping and housework; this assistance was usually provided by family members. The provider of assistance was generally compatible with older people’s preferences concerning assistance at home. We found no differences in care preferences between urban and rural settings. Assistance in the home environment was predominantly provided by unpaid helpers, which reflects recent developments in health and social services that put an emphasis on a person’s social network. Due to demographic changes and the decrease in the number of adult children, reliance on close relatives might soon become a challenge. These findings can help policy makers understand older people’s choices and preferences better when planning long-term care.
Previous studies have established the need for formal and informal care based on the level of (unmet) needs of older people in Slovenia.
This study examines older people’s perceptions of their abilities in connection to different activities and their preferences regarding assistance. It also examines the association between current needs and preferences and specific demographic factors.
The findings can help policy makers understand older people’s needs and preferences, which is particularly relevant since the Long-Term Care Act is currently being developed in Slovenia.
Introduction
The Eurostat Dissemination Database estimates that by the end of 2030, almost a quarter (24.9%) of Slovenians will be 65 years or older. 1 The changed demographic structure is bringing various economic, social, and political challenges. It also highlights the need for careful consideration of available resources in the current socioeconomic climate. 2 Long-term care (LTC) of the aging population is a question many countries are trying to address.3,4 Long-term care can be provided in different places by different caregivers, depending on a person’s needs, and encompasses both medical and non-medical care. Mostly, it is provided at home by unpaid family members and friends. It can also be given in a facility such as a nursing home or in community, for example, in an adult day care center. 5 Recent changes in social and structural factors have created an urge for a gradual move from informal to professional services, which has implications for the structure and organization of LTC in most countries. 6
Although LTC policies apply to people of all ages who require assistance and support, this article will focus on 1 group: people over 65 living at home. Home-based LTC services can enable older people to live as independently and safely as possible when they can no longer perform everyday activities. They are also considered financially more viable compared with institutional care. 7 When designing LTC programs, policy makers should understand the needs and preferences of older people better, so that the care that is offered can adequately support them in the home environment. 8 Our aim is to provide data that could guide the development of the LTC Act in Slovenia by eliciting formal and informal care preferences of the Slovenian population of older people and their needs for assistance.
Theoretical Background
Aging in place
The option of remaining in the home environment—“aging in place”—is increasingly being promoted and is now considered the preferred method of aging.9-12 Although aging in place initiatives have a favorable status in both literature and professional discourse, knowledge about the needs and intervention preferences of older adults living at home is lacking.13-15 Many home-dwelling older people experience difficulties and require assistance with various activities, including personal care, shopping, and home maintenance. A person’s ability to perform basic activities of daily living (ADLs) that involve caring for one’s self and body—such as dressing, using the toilet, and bathing—is related to their functional mobility and can be a measure of age-related disability.16,17 Generally, independence in ADLs is the main goal in the care of older adults and improves their quality of life. 18 Instrumental activities of daily living (IADLs)—which include shopping, managing finances, and meal preparation—are another important aspect of maintaining independence as people grow old. Their performance can be associated with both cognitive and physical abilities. To enable a person to stay at home, IADLs are often the first to be delegated to others. 16
Coleman, Kearns, and Wiles 11 argue that to age in place, older people require supportive relationships; interdependence is crucial in this process. In most European Union (EU) countries, family members are the most likely providers of care, with over 60% of assistance carried out by informal caregivers. 19 In fact, to support aging in place and reduce expenses, informal care structures and the use of outpatient services have been widely encouraged in Europe. 8 Nonetheless, formal carers have been recognized as an essential component of the so-called “care triads,” consisting of informal carers, professionals, and the client. 20 A literature review performed by Hengelaar and colleagues 21 showed that of all the health and social care professionals, nurses were the most common providers of LTC services, followed by case managers, occupational therapists, physiotherapists, social workers, managers, and support staff. Hengelaar et al 21 also concluded that cooperation between professionals and informal caregivers was not always efficient, which they contributed to their diverse backgrounds. Assistance, however, is not the only requirement for aging in place. A qualitative study by Grimmer, Kay, Foot, and Pastakia 22 showed that the success of aging in place involves other elements too, as described by the acronym HIPFACTS: Health, Information, Practical assistance, Finance, Activity (physical and mental), Company (family, friends, pets), Transport, and Safety.
International studies show that if older people’s needs regarding ADLs and IADLs are not met in their home environment, this can lead to adverse effects, including falls, hospitalizations, and nursing home placements. 13
A New Zealand–based study found that 81% of people over the age of 75 require assistance with at least 1 activity, and that support is most often provided by spouses, except for heavy housework and transportation. 13 A Swedish study also found that the majority (90%) of informal care is provided by spouses and children. 23 In urban environments, however, where many people live alone, informal care is less available, suggesting a potentially vulnerable group of older people. Generally, older people who live alone are more likely to experience unmet needs. 24 Researchers also noted a pattern; while in high-income countries, informal care is most often provided by spouses, in mid-income and low-income countries, children and children-in-law are the most likely providers. 23
The above review of the literature suggests that informal family support as well as formal assistance are an essential aspect of aging in place. Nonetheless, the availability of formal LTC services is generally low. A review of coverage deficits in 46 countries found that 48% of older persons are not covered by any type of formal provision of services and 46% are excluded from any coverage that does exist by some form of means testing. Only 5.6% of older persons worldwide are covered by legislation that provides coverage for all. 25
Context of the study
There has been a strong tendency in Slovenia to promote personal responsibility for one’s health and well-being. Consequently, older people, their families, and friends are increasing their active participation in the provision of care and assistance, especially in the home environment.26,27 Currently, LTC provision is not clearly defined in Slovenia, criteria for inclusion are not unified, and the formal procedures are complex and lengthy. 28 Furthermore, the proportion of gross domestic product (GDP) afforded to LTC dropped in 2013 to 1.33%. Of this amount, 77.7% was spent on institutional care and only 22.3% on home care, which suggests that investments in home care are relatively low. 29 These data put Slovenia below the average of other member countries of the Organisation for Economic Co-operation and Development, where home care is generally seen as a priority. According to Eurostat, 30 the share of LTC services in Slovenia accounted for just over 15% of current health care expenditure. In comparison, the share of LTC services was 31.3% in Sweden, 39.1% in the Netherlands, and 41.9% in Finland.
In February 2017, the Personal Assistance Act was passed by the Slovenian Parliament. This new legislation will support the provision of personal assistance to people with long-term disabilities to facilitate their participation in society. However, legislation that would specifically address people with long-term needs—including those who live at home—and that would clearly define the nature and scope of such assistance is still missing in Slovenia. This niche is expected to be covered by the LTC Act, which has been in preparation since 2002. Purportedly, when this law is passed, Slovenia will get a more contemporary and holistic system of LTC, with the possibility of developing different social care programs with a stable source of financing. The law will also define which health and social care professionals will be included in the provision of LTC at home. 28 It is, therefore, crucial to provide evidence-based information that could guide policy makers when developing new legislation.
A study that explored the unmet needs of the older population in Slovenia showed that although the majority (87%) of old people do not report care needs, 4% of older people in Slovenia have severe needs for care, which are not being met. 26 Hlebec 31 also noted that particularly in urban environments, which are less family oriented, the need for formal care providers might be more pronounced. Formal care is presently more frequently received by those with higher needs and those living in urban environments. 27 This suggests that to minimize the risks to specific groups of older people, coordinated formal care services and LTC social policies are required in Slovenia.
Although previous studies have established the need for formal and informal care based on the level of (unmet) needs of older people in Slovenia,26,27,31 little is known about older people’s perceptions of their abilities and their preferences regarding assistance. To address this knowledge gap, we adopted a user-engagement perspective and recorded the perspectives of older Slovenians regarding their independence and the need for assistance in the home environment. The research questions driving this study were as follows:
The information generated from this research is expected to provide some important insights that could guide the planning of services and policies in Slovenia, by including the users’ perspective. In particular, it could help us understand which professionals and non-professionals should be included in the upcoming LTC legislation so that their services and assistance could be provided to home-dwelling older people according to their wishes.
Methods
Study Design
This was a cross-sectional study. To gather data, we developed and validated a novel questionnaire that was distributed among community-dwelling adults over the age of 65 living in different Slovenian counties. Data were analyzed using descriptive statistics, a nonparametric test (Wilcoxon signed rank), and the chi-square test in SPSS Statistics 24.
Measurement Instrument
The questionnaire that was developed for this study consisted of the following:
Seven questions that were linked to the participants’ demographic characteristics.
One question (with 15 items) that was related to the level of independence in performing ADLs and IADLs. The scale consisted of 8 ADLs and 7 IADLs. Activities of daily living were chosen based on the Katz Index of Independence in Activities of Daily Living 32 and IADL were based on the Lawton Instrumental Activities of Daily Living Scale. 33 Reliability was checked for this part of the questionnaire. Cronbach’s alpha was .966 for ADLs, .950 for IADLs, and .971 for all 15 items together, which shows that the instrument can be considered highly reliable. 34 Table 1 shows the definitions that were used for each ADL and IADL activity. A 3-point scale was used for each activity performance: performs independently, partially independent, and unable to perform.
Three questions were related to the assistance received with everyday activities.
Description of Activities of Daily Living and Instrumental Activities of Daily Living Included in the Questionnaire.

Participants and Data Collection
In Slovenia, in 2016, 359 577 people over the age of 65 lived at home. 35 Of these 206 041 were members of Older People’s Associations (OPAs). 36 As this was an independent study that received no funding, the researchers decided to access older people through OPAs. The inclusion criteria were that the potential participants were over 65 years old, living at home and that they had no diagnosed cognitive impairments. Potential participants could be recipients of home care, could attend day centers, and/or be active in non-governmental organizations. The aim of the sampling was to include a wide variety of people, with different interests and characteristics who could represent the population of Slovenian older people living at home.
The first author approached all OPAs in Slovenia (N = 509) either by mail or email and asked for assistance with the study. Almost 20% of OPAs (N = 94) responded and expressed an interest to participate. Subsequently, meetings were arranged in public places where the researchers could contact potential participants, members of OPAs, in-person. For example, after a lecture in a community center organized by an OPA, lecture participants were approached by the researchers and asked to take part in the study. The researchers first introduced the research project and provided research information sheets, as well as contact information. The questionnaire was then presented to those who expressed an interest and they were given instructions about each of the questions. Participants could either complete the questionnaire after the initial meeting or choose to be visited at their homes at a time convenient for them. Prior to completing the questionnaire, they were also invited to ask questions to clarify the aim of the research as well as question wording. The participants completed the questionnaire independently; however, assistance was provided if required. As an incentive, the participants were offered a free lecture on falls prevention in the home environment and a presentation relating to medical equipment. Participation in the study was voluntary and unpaid. Participants were able to terminate their involvement at any point with no consequences.
The questionnaire was presented to 635 people, of which 358 agreed to participate. After reviewing the questionnaires, we noticed that 316 people completed the questionnaire in full, while 46 completed it partially. Therefore, the number of respondents differs among questions.
Data Analysis
Basic descriptive statistics were used to (1) describe the sample, (2) record the level of independence in ADLs and IADLs, (3) identify what type of assistance is being used, (4) identify who is providing support with activities at the moment, and (5) identify who the preferred provider of assistance would be. As differences between pairs were non-normally distributed, Wilcoxon signed rank test was used to establish whether participants were more independent in ADLs compared with IADLs. First, a new variable was calculated for ADLs as the mean of all 8 items. The same was done for 7 items for IADLs. The 2 variables were then compared using the nonparametric test. To establish if preferences regarding assistance provision were associated with current providers of support, we first looked at the frequency distribution of both questions and then used the chi-square test.
Results
Sample Description
More than two-thirds (68%) of the participants were women and 32% were men. They were between 65 and 97 years old (mean = 74.2, SD = 7.1). More than half (59%) lived in the city and 41% in rural areas. A quarter of the participants lived alone, 50% with a partner or a spouse and 23% with close family members (children, grandchildren). The rest (2%) reported living with other family members. Almost half of the participants (49%) lived in a private house with more than 1 floor, 24% lived in a private house with ground-level living only, 13% lived in an apartment block with more than 4 floors, and 11% lived in an apartment block with less than 4 floors. The rest (3%) reported living in other types of residencies, such as a country house.
The Level of Independence in ADLs and IADLs
Table 2 presents data on the level of independence in different ADLs and IADLs as expressed by the participants. Over 95% of the respondents reported that they were independent with feeding and using the toilet. These 2 activities were followed by transfers (from bed to chair and getting up from a chair), which were performed independently by 94% of the participants. Out of the 8 ADLs included in the questionnaire, the highest dependence was recorded in bathing, with 4.2% unable to perform this activity and another 5.7% requiring some assistance to bathe. Grooming was another ADL in which a comparatively high number of participants reported limited independence, with 7.2% requiring some assistance and 2.3% unable to groom themselves. Out of the 7 IADLs, the highest independence was recorded with using the telephone (89.7%). In contrast, shopping and housework were the 2 activities where the highest number of participants reported that they were not independent.
Descriptive Statistics and Frequencies for Independence in ADLs and IADLs.

Note. ADLs= activities of daily living; IADLs = instrumental activities of daily living.
The first 8 activities are basic ADLs, followed by 7 IADLs.
Valid answers for each question.
A Wilcoxon signed rank test indicated that independence in ADLs was statistically significantly higher than independence in IADLs (Z = −7.006, P = .000) at 5% significance level. This suggests that older Slovenian people included in our study were more independent in ADLs compared with IADLs.
Assistance With ADLs and IADLs
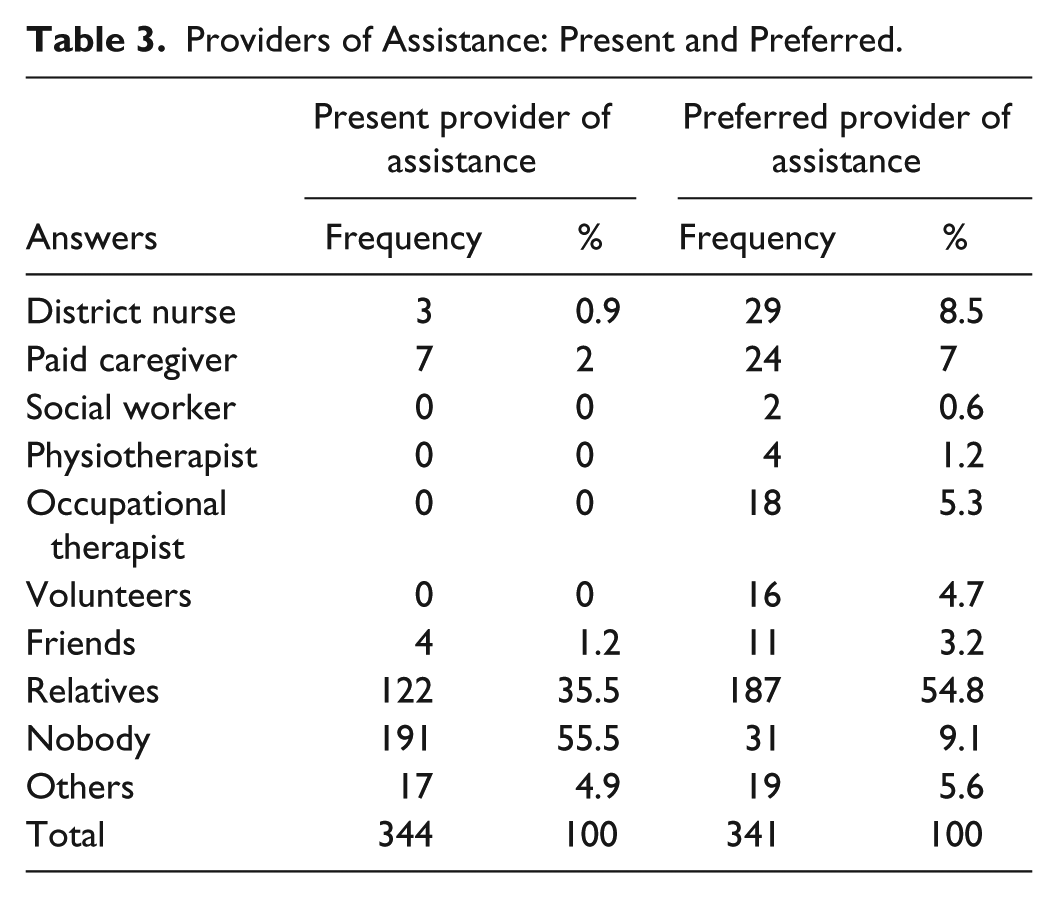
More than three-quarters of the participants (76.7%) reported that they currently had no assistance with their everyday activities; 15.5% reported they used unpaid helpers, and 7.8% used paid assistance. Participants reported that help was most often provided by relatives (35.5%). Other providers of help, such as friends and paid caregivers, were used less often. When asked about the preferred provider of assistance, a strong preference was given to relatives, which were chosen as preferred caregivers by 54.8% of the respondents. Out of health care providers, district nurses were the preferred option (8.5%), followed by paid caregivers (7%). Table 3 shows the current and preferred providers of assistance.
Providers of Assistance: Present and Preferred.
The likelihood ratio test was used to check if the current provider of assistance was linked to the participants’ choice of caregivers. The likelihood ratio test is preferred to chi-square test when theoretical frequencies equal less than 5. 34 The categories from Table 3 were combined into 3 categories; (1) formal providers (district nurse, paid caregiver, social worker, physiotherapist, occupational therapist), (2) informal providers (relatives, friends, volunteers), and (3) none. The association between 2 variables was significant, χ2(df = 4, N = 309) =51.219, P = .000, at 5% significance level. Therefore, there was a statistically significant association between the current and preferred provider of care. Detailed inspection of the contingency table showed that older people who received formal assistance wanted to keep paid providers. The majority (74.8%) of older people who received informal assistance preferred their help to remain the same in the future, 1.6% said that they did not need any assistance, and 23.6% would prefer formal assistance instead. Furthermore, almost two-thirds (64.2%) of older people who had no assistance would prefer informal assistance in the future, 16.5% would like to stay independent (with no assistance), and 19.3% expressed they would like to have formal assistance, signaling a general preference for informal care.
In addition, we investigated whether assistance preferences and current needs were associated with specific demographic characteristics. First, the living status variable was combined into 2 categories; (1) living alone and (2) living with a partner or family members. The results of the chi-square test showed no statistically significant association between the living status and current assistance provider, χ2(df = 2, N = 281) = 5.057, P = .080, and between the living status and preferred assistance provider, χ2(df = 2, N = 278) =5.911, P = .052. Also, 67.6% of the participants who lived alone and 66.2% of those who lived with a partner or family member expressed a preference for informal assistance in the future.
We also examined the association between the living environment (urban/rural) and assistance needs and preferences. The results showed that the current assistance provider was associated with the living environment at 5% significance level, χ2(df = 2, N = 289) = 9.308, P = .010. Almost a third (30.8%) of older people living in an urban environment had informal assistance, while 65.7% received no help. In rural environments, almost a half (48.3%) of the sample received informal assistance. The same percentage reported that they did not have any assistance. Only 3.3% of the respondents from rural areas had formal assistance, which was similar to the urban environment where 3.6% had formal assistance. The results for the preferred assistance provider showed no statistically significant association with the living environment at 5% significance level, χ2(df = 2, N = 286) =3.000, P = .223. Our results also showed that only a quarter of the participants in both groups preferred formal assistance (23.8% in urban and 23.7% in rural environments).
Discussion
In the context of an ongoing pursuit of a more comprehensive national strategy for the provision of LTC in the home environment, the aim of our study was to better understand the current needs and preferences of older people in Slovenia from their perspective. Our findings suggest that community-dwelling older Slovenians are more independent in their basic ADLs, such as using the toilet, eating, and dressing, compared with IADLs that include shopping, meal preparation, and housework. The independence was the highest for using the toilet and feeding, 2 important self-care activities, as well as for mobility transfers. This is not surprising considering that these are the activities which are essential for a person’s ability to function independently at home. Once a person needs assistance with ADLs, they are more likely to be institutionalized. 17 In other words, independence in ADLs is crucial for a person’s ability to age in place.37,38
It is generally easier to provide support with IADLs via an informal network than it is to assist with ADLs.13,39 The latter frequently require involvement from outside health agencies.40,41 Moreover, ADLs performance is often linked to a person’s immediate safety and physical well-being; therefore, it often receives more attention. 42 While family members can be a source of assistance for IADLs, professional services should be available for ADLs when needed. 43 This has also been suggested by our study; the participants mostly required assistance with IADLs, which was offered by relatives and enabled the older people to continue living at home. Home-based LTC policies in Slovenia might, therefore, need to prioritize formal assistance with ADLs as a way to enable people to stay in their home environments once they start experiencing needs related to personal care, especially since this is more difficult to be managed by a person’s social network.
Another important finding of our study was that older people most frequently required assistance with bathing. According to previous studies, difficulties with bathing have shown the highest associated risk of future institutionalization. 44 Therefore, this activity requires special consideration when planning LTC interventions in the home environment. In Slovenia, older apartments and houses frequently have a bath tub with no shower that could be used as an alternative. This makes the performance of this activity (as well as assistance) more difficult. By providing assistance with bathing, we might be able to delay institutionalization. To minimize the risks of falls and injury, a good safety assessment should be considered in relation to bathing and washing. 17 Potential caregivers should be included in the planning of services, so that they, too, understand the risks and can be instructed in the best techniques for providing assistance.
Perhaps surprisingly, our study also found that grooming was an activity that a number of participants required assistance with. As grooming is an activity that is developed early on in a person’s life, this finding goes against the hierarchy of functional decline. In a study by Njegovan and colleagues, 45 grooming, along with feeding, was the most preserved activity in old age. Our finding could be explained by the way this item was defined in the questionnaire. In addition to hair brushing and styling, grooming also included hair washing. Many participants found hair washing difficult to perform and therefore rated the item lower as we expected. This finding signals that hair washing is another ADL that older people require assistance with and should be considered when providing LTC services in the home environment.
The majority of our participants required no assistance for everyday activities. Our findings are similar to the results of a Swedish study that recorded the need for assistance among community-living older people. 23 They found that 73% of older people received no care, 14% received formal care, 17% informal care, and 7% received both. On the contrary, Slovenian older people appear to remain more independent compared with older people in New Zealand, where 81% reported the need for assistance. 13 However, the New Zealand study included only those over the age of 75, whereas our study also included younger people who could arguably be physically and mentally fitter compared with their older counterparts, which influenced the outcome.
Older Slovenians who had assistance mostly used unpaid helpers, such as family members. This is congruent with previous findings from Slovenia that indicated older Slovenian people mostly relied on their relatives to assist.26,27,31 Participants’ preferences for informal carers were clear among all the participants, regardless of setting and living status. According to the statistical analysis, the current and preferred provider of assistance often matched, suggesting an isomorphic relationship. Among formal providers of care, the strongest preference was given to district nurses, paid carers, and occupational therapists. In the Slovenian health care system, district nurses are providers of medical care, paid carers are associated with assistance with ADLs, while occupational therapists could be seen as the promoters of general independence. This might imply that these are the needs older people feel most strongly about, so should be considered when planning home-based services.
The fact that the actual provider of care was often the preferred option could potentially have a positive effect on the older people’s psychological health and well-being. This aspect could be explored in future studies. It is, however, not clear if the choice was perhaps influenced by the perceived lack of other options and unfamiliarity with what else was available (for instance, state-funded alternatives), or whether it was a reflection of factors such as older people personal characteristics and Slovenian culture. Also, we do not know how the relatives perceived this relationship. For instance, was the assistance provided voluntary, or was it driven by personal and social expectations? A study from the Czech Republic showed that family caregivers often provide care out of moral and emotional reasons. Although they usually want to continue caring for their relatives, this involves several risks, including financial worries and loss of employment. 46 This needs to be considered when developing new models of LTC. Over-reliance on family members could potentially put another segment of the population at risk. 6 Research also shows that informal providers of care often experience significant stress and reduced quality of life related to helping their relatives on an ongoing basis.47-49 Due to high exposure to mental stress, Knussen and colleagues 48 suggest that family caregivers of older relatives need to occasionally take breaks from caring to restore balance in their lives. There might be a need to alternate between formal and informal forms of assistance to ensure that the caregivers do not experience distress or burn out. Future policies should allow for such an arrangement; for example, if a relative provides the majority of care, that person should regularly be allowed some respite time. 6 Older Slovenian people expressed a preference for informal carers, which should be considered by the policy maker. However, family members or friends who provide care should be offered reimbursements, benefits, and social security to acknowledge their assistance as work.
Reliance on close relatives appears to be an international trend.6,50 However, due to demographic changes, the decrease in the number of adult children might affect this arrangement. Not all older people have close kin; therefore, the option of close relatives providing care and support should not be automatically presumed. In our sample, only 23% of the participants lived with close family members. This implies that a significant proportion of the population does not have potential providers of assistance on-site or in proximity, and might, therefore, be more vulnerable to self-neglect and injury.
Limitations
The present study had several limitations. Although great efforts were made to recruit a wide variety of older people, the sample did not comply with the principles of probability; therefore, generalizations to the general population can only be made tentatively. We acknowledge that our participants were members of OPAs and that they might be more informed and active compared with older people who do not engage in activities outside of their homes. Also, we did not include people with cognitive impairments; therefore, our results most likely reflect the needs and preferences of cognitively relatively intact older people. The cognitive status of our participants was not objectively assessed. It could be that some of them experienced cognitive decline and might have shown limited insight when answering the questions about independence. On the contrary, the 2 activities that are traditionally connected with higher cognitive skills—medication management and using the telephone—were the 2 activities in which the participants reported the highest independence out of all IADLs included in the questionnaire. We could, therefore, assume that cognition was probably not the most significant factor that predicted the need for assistance in our sample. However, as the level of independence was self-reported, we do not know essentially how well the older people everyday performed these activities, for instance, whether the doses of medication were appropriate. Older people with cognitive difficulties represent a distinct population with specific needs for LTC, especially pertaining to safety. They usually require more hours of formal and informal care compared with cognitively intact peers to stay in the home environment. 51 Future studies could focus specifically on older adults with cognitive impairments and provide separate policy recommendations for this group.
Data were gathered using a questionnaire, so all answers were a reflection of the participants’ self-assessment and revealed their subjective perceptions of independence. As there was no objective measurement, it could be that the participants either under-estimated or over-estimated their competencies and the amount of assistance they required. Furthermore, some participants did not complete the questionnaire in full. We believe this was probably due to the length of the questionnaire, causing survey fatigue. This observation would need to be considered when designing future studies in this area.
In conclusion, our study suggests that older, home-dwelling Slovenian people (members of OPAs) are more independent in their basic ADLs than IADLs. They most often require assistance with tasks such as shopping and housework. The assistance is usually provided by informal carers, which is congruent with older people’s wishes regarding their caregivers. Informal caregivers appear to be the preferred option regardless of the living status (living alone vs living with family) and the environment (rural vs urban). Based on our findings, we suggest that home-based LTC in Slovenia should include a combination of formal and informal services. While formal services are mostly required for severe ADL needs, informal structures should be utilized for IADLs when possible. As reliance on informal caregivers is very pronounced in Slovenia, future policies should consider the health and well-being of care providers and allow for a balanced approach as well as offer appropriate financial reimbursements for informal caregivers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.