
Abstract
The aim of this systematic scoping review was to identify and analyze indicators that address implementation quality or success in health care services and to deduce recommendations for further indicator development. This review was conducted according to the Joanna Briggs Manual and the PRISMA Statement. CINAHL, EMBASE, MEDLINE, and PsycINFO were searched. Studies or reviews published between August 2008 and 2018 that reported monitoring of the quality or the implementation success in health care services by using indicators based on continuous variables and proportion-based, ratio-based, standardized ratio–based, or rate-based variables or indices were included. The records were screened by title and abstract, and the full-text articles were also independently double-screened by 3 reviewers for eligibility. In total, 4376 records were identified that resulted in 10 eligible studies, including 67 implementation indicators. There was heterogeneity regarding the theoretical backgrounds, designs, objectives, settings, and implementation indicators among the publications. None of the indicators addressed the implementation outcomes of appropriateness or sustainability. Service implementation efficiency was identified as an additional outcome. Achieving consensus in framing implementation outcomes and indicators will be a new challenge in health services research. Considering the new debates regarding health care complexity, the further development of indicators based on complementary qualitative and quantitative approaches is needed.
While measuring implementation success, it is important to differentiate among service, client, and implementation outcomes. Several studies report the need for valid measures.
This systematic scoping review shows a need to develop valid indicators to measure implementation success. In this context, both health care complexity and pragmatism should be considered.
A new generation of complementary qualitative and quantitative indicators may be suitable to meet the challenges of health care complexity.
Introduction
Substantial resources are invested in the health care system to improve the quality of care.1,2 However, evidence-based innovations in health care do not necessarily achieve their desired effects if they are affected by poor implementation quality. 3 Therefore, it is important to differentiate between innovation and implementation effectiveness to measure implementation success. 4 Innovation and implementation effectiveness can be measured in research settings or in a daily routine setting. 5
“Innovation effectiveness describes the benefits [that] an organization receives [because] of its implementation of a given innovation (. . .)” 4 and can be measured by service or client outcomes, e.g., efficiency, safety, equity, patient centeredness, and timeliness. 5
“Implementation effectiveness refers to the consistency and quality of targeted organization members’ use of a specific innovation”. 4 It can be measured by implementation outcomes, e.g., acceptability, adoption, appropriateness, costs, feasibility, fidelity, penetration, and sustainability. 5 In the context of the quality implementation framework, the term quality implementation is used and defined as “(. . .) putting an innovation into practice in such a way that it meets the necessary standards to achieve the innovation’s desired outcomes”. 6 This definition emphasizes that implementation can be seen as a construct with gradations between low and high quality. 6 The definition of implementation quality also emphasizes the importance of a predefined determination of the level of expectations for the implementation outcome. 6 The following related terms also exist: implementation strength, which refers to the “(. . .) amount of the program that is delivered”; 7 implementation intensity, which refers to the “quantity and depth of implementation activities”; 7 implementation quantity, which refers to the “dosage”; 7 and implementation degree, which refers to the “degree to which the intervention can be adapted to fit the local context, the strength and quality of the evidence supporting the intervention, the quality of design and packaging and the cost”. 7 However, in all the definitions, the implementation outcome measurement is central.
Finally, implementation success comprises both innovation and implementation effectiveness in a setting of the daily routines of health care services, including the measurement of service, client, and implementation outcomes.4,5
The importance of valid implementation measures to evaluate effectiveness due to their intermediate function between service and client outcomes and implementation outcomes is reported in several studies.1,5 Although there are several strategies to integrate evidence-based practices into daily routines to improve health care services’ effectiveness, there is still a need for validated implementation measures. 1
Implementation outcomes can be measured by using administrative data and indicators.8,9 Indicators have a long tradition in measuring the quality of health care; 10 they measure factors that cannot be directly observed, 11 they have a predictive function, 12 and their reference range or value indicates good or bad quality. 13 An indicator “is a quantitative measure that can be used as a guide to monitor and evaluate the quality of important patient care and support service activities (. . .)”. 10 Comparable implementation indicators have a crucial function in implementation monitoring and benchmarking. 9 Although there are reviews that address the measurement of implementation outcomes8,14 and another review is planned, 15 none of them explicitly focuses on quantitative implementation indicators. Therefore, the aim of this systematic scoping review (SR) was to identify and analyze indicators that address implementation quality or success in health care services and to deduce recommendations for further indicator development.
Methods
A systematic scoping review (SR) was performed according to the approved standards of the “Joanna Briggs Institute Reviewers Manual 2015” 16 and the “PRISMA Statement”. 17
Data Sources and Search Strategy
The databases CINAHL via EBSCO, EMBASE via OVID, MEDLINE via PubMed, and PsycINFO via OVID were searched (see Supplemental Appendix 1). The search strategy was developed according to a predefined SR protocol. The search strategy was pretested by 2 authors (T.W., S.K.) by performing a title-abstract screening of the first 100 records. The search terms were verified according to the PRESS Checklist. 18 A two-part search string that combined the search components of implementation and indicator was used. The first string included several terms and synonyms for implementation, e.g., implementation, implementing, implemented, knowledge translation, and dissemination. This was supplemented by the implementation outcomes defined by Proctor et al., 5 e.g., acceptability, implementation costs, and sustainability. The second string included several terms and synonyms of indicator, e.g., indicator, indicators, index, indices and measure, validation, monitoring, and outcome. The search terms were limited to their appearance in the titles of publications to improve precision.
Inclusion and Exclusion Criteria
The literature published in English or German between August 2008 and August 2018 was included. Publications were included if they reported monitoring of the quality or success of the implementation of health care interventions or innovations by using quantitative process or outcome indicators or indices. The type of implemented interventions or innovations was not relevant for inclusion or exclusion. However, the identified publications had to be related to health care settings, e.g., inpatient, outpatient, and community health care.
Included publications had to contain indicators that measured continuous variables or proportion-based, rate-based, ratio-based, or standardized ratio–based variables. Indicators that were not explicitly associated with implementation were excluded, for example, performance measures that serve to measure the quality of the provided evidence- and/or consensus-based care and its changes in daily routines. 19 These types of measures were only included if they were aimed at and described in the context of implementation measurement.
All types of studies, reviews, and expert reports were included. Letters, editorials, and comments were excluded. Publications that only contained qualitative indicators were excluded.
Literature Selection
The literature selection was conducted and double-checked independently by 3 reviewers (T.W., S.K., B.W.). Duplicates were excluded. First, a title-abstract screening was conducted by categorizing the records (“included,” “excluded,” or “unclear”). For the records that were categorized as “included” and “unclear,” the full text was screened for final eligibility. Backward and forward citation tracking was performed. In cases where there was uncertainty, an uninvolved reviewer was consulted.
Data Extraction and Synthesis
Relevant core data such as the author, publication year, study design, methods, setting, objective, and results were extracted and tabulated according to the Joanna Briggs Institute Reviewers’ guideline. 16 The Cochrane guideline 20 was also considered for the narrative presentation of the results. A content analysis and data synthesis was performed by combining a deductive and inductive analysis process. 21 The coding of the literature was performed by 2 authors (T.W., S.K.). The indicators were categorized as a continuous variable, proportion, rate, ratio, or standardized ratio (see Figure 1). Continuous variable indicators (CBIs) are based on aggregate data whereby the measured value can be represented by any point on a continuous scale, 13 e.g., the indicator session exposure, which “(. . .) represents the average number of (. . .) sessions that [an] organization delivered”. 1

Types of quantitative indicators.
Proportion-based indicators (PBIs) measure the frequency of an event (numerator) in a defined population (denominator), 22 e.g., “(. . .) the number of providers who deliver a given service or treatment, divided by the total number of providers trained in or expected to deliver the service”. 5
Rate-based indicators (RABIs) are expressed by proportions or rates within a given time period. Both the numerator and denominator must contain the population at risk or defined event(s). Additionally, the period of time in which the deviation might occur has to be considered, 12 e.g., “[Health Surveillance Assistants] supervised at village clinic in [Integrated Community Case Management] in the last 3 months [divided by] [s]urveyed [Health Surveillance Assistants] working in [Integrated Community Case Management] at the time of assessment”. 9
Ratio-based indicators (ROBIs) measure different endpoints in the numerator and denominator, 22 e.g., the number of patients who request the implemented service compared to the number of patients who are being offered the service. 23
Standardized ratio–based indicators (SROBIs) play a special role among the indicators based on discrete variables. 24 They were measured by the number of events that occurred compared to the expected number of events, e.g., the penetration rate, which is calculated as the “Number of eligible patients who use the service [divided by the] number of potential patients eligible for the service”. 23
Indices contain several indicators that measure one phenomenon of interest. 11
To apply deductive coding, a coding guide was used that considered the implementation outcomes of Proctor et al. 5 Additional categories, e.g., implementation quality or success, were developed inductively. By clustering 21 and the tabulation of the key results, the differences and commonalities among the identified indicators were identified. In the case of uncertainty regarding the identification of indicators as implementation indicators, the corresponding authors of the publications were contacted, e.g., Karim et al. 25 and Garcia-Cardenas et al. 23
Quality Appraisal of the Indicators
The quality of the indicators was checked by the following criteria based on “Measure Evaluation Criteria and Guidance for Evaluation Measures for Endorsement” of the National Quality Forum (NQF): 26 (1) importance to measure and report refers to the “Extent to which the specific measure focus is (. . .) important to making significant gains in healthcare quality where there is variation in or overall less-than-optimal performance”; 26 (2) scientific acceptability of measure properties refers to the availability of psychometric data, especially reliability and validity; (3) feasibility refers to the “Extent to which the specifications, including measure logic, require data that are readily available or could be captured without undue burden and can be implemented for performance measurement”; 26 (4) usability refers to the “Extent to which potential audiences (. . .) are using or could use performance results for both accountability and performance improvement to achieve the goal of high-quality, efficient healthcare for individuals or populations”; 26 and (5) related and competing measures refers to “(. . .) endorsed or new related measures (. . .) or competing measures (. . .), the measures are compared to address harmonization and/or selection of the best measure”. 26
Each criterion was rated yes if the authors of the included papers provided comprehensive information about the quality of the indicator (set) or explicitly stated that the criterion, e.g., validity, was met. Yes* was assigned if the quality criterion was only mentioned briefly or was applicable to individual indicators. No was assigned if the given information suggested that the indicator (set) did not meet the criterion. Not mentioned was assigned if there was no information in relation to the criterion.
Results
In total, 4376 records were identified that resulted in 10 eligible studies,1,5,9,23,25,27-31 including 67 implementation indicators. Of these studies, the publication of Karim et al. 25 was identified by backward citation tracking of Hargreaves et al. 32 Both publications of Stiles et al. 30 and Garcia-Cardenas et al. 23 were identified by backward and forward citation tracking of Proctor et al., 5 respectively (see Figure 2). More than half of the studies, 6 out of 10, were published in the last 5 years. The most common reason for excluding publications during the title-abstract screening was missing quantitative indicators in the context of implementation.
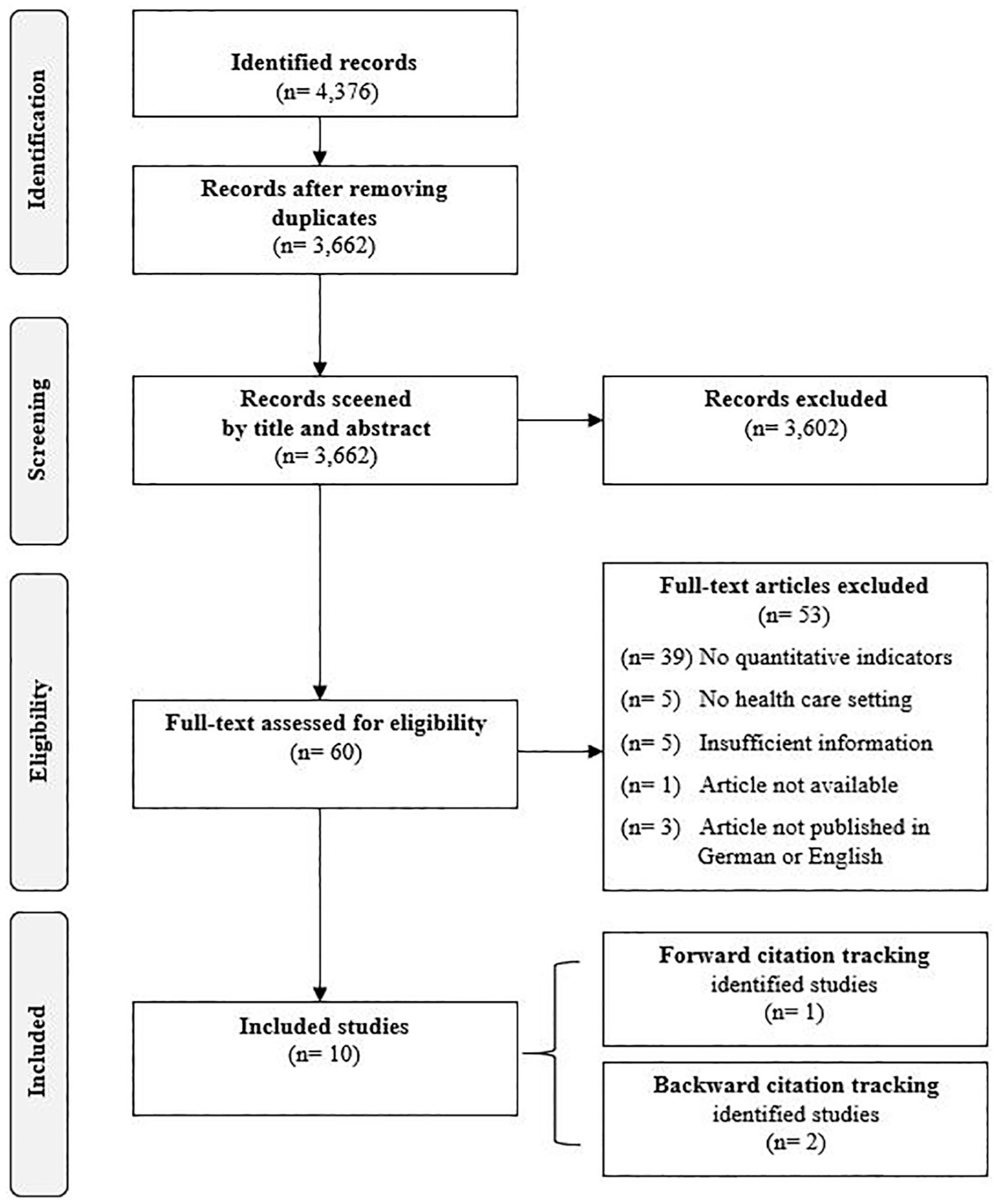
Prisma flowchart.
There were 2 mixed method studies, one based on a case report and effectiveness implementation hybrid design 23 and the other based on a narrative review and consensus-based approach 27 (see Table 1). Seven quantitative studies1,9,25,28-31 that consisted of a follow-up study, 1 cross-sectional studies,9,25 secondary data analyses, 28 (randomized) implementation trials,29,31 and an exploratory study 30 were included. One review that provided recommendations for implementation indicators was also included. 5
Overview of the Identified Publications.

Described by the authors of the publications.
There was high heterogeneity regarding the objectives and settings of the publications. Six publications reported indicator (framework) development, conceptualizations, and/or indicator validation.1,5,27,29-31 The other 4 publications reported the evaluation of implementation by implementation indicators.9,23,25,28
Seven of the publications addressed community health care settings5,9,23,25,27,29,30 including mental health care,5,29,30 2 publications addressed the stationary health care setting,1,31 and 1 publication addressed the primary health care setting. 28
Implementation Indicators
In total, 67 indicators were identified (see Table 2). The development of 41 indicators out of 5 studies1,5,23,29,31 was based on a theoretical background or framework. Three of the publications1,5,23 were based on the conceptual model of Proctor et al., 5 and 1 referred to the Stages of Implementation Completion (SIC) introduced by Chamberlain and colleagues to identify a timeframe for implementation activities and the proportions of completed activities. 29 Furthermore, the theoretical framework of information theory presented by Shannon and Weaver was used to develop indicators. 31
Indicator Description.

Note. GP = general practitioners; MRF = pharmacist-led medication review with follow-up; PBI = proportion-based indicator; CBI = continuous variable indicator; ROBI = ratio-based indicator; SROBI = standardized ratio–based indicator; RABI = rate-based indictors; A-CRA = Adolescent Community Reinforcement Approach; SAMHSA = Substance Abuse and Mental Health Services Administration; CSAT = Center for Substance Abuse Treatment; KMC = Kangaroo Mother Care; LBW = low birth weight; STS = skin-to-skin; HSA = Health Surveillance Assistant; MOH = Ministry of Health; NSO = National Statistical Office; iCCM = Integrated Community Case Management; HTRA = hard-to-reach areas; ORS = oral rehydration solution; HEW = Health Extension Workers; CHPs = Community Health Promoters; FHC = Family Health Card; iCPR = integrated clinical prediction rule; M.D.= physician; R.N. = registered nurse; DC = discontinue.
Indicators categorized by outcomes consistent with Proctor et al. 5 by the authors of the identified publications.
Indicators categorized by described outcomes of the authors of the identified publications.
Indicators categorized by outcomes described by the authors of this article consistent with Proctor et al. 5
Indicators categorized by Proctor et al. 5 according to their defined outcomes.
The distribution regarding the indicator types and the indicators that address implementation outcomes was not balanced. There was high heterogeneity regarding the objectives of the indicators. The indicators were based either on a continuous variable (n = 23)1,23,31 or on a discrete variable (n = 42),1,5,9,23,25,27-30 and some (n = 2) could not be categorized because the data provided were poor. 28 There were only 2 standardized ratio-based indicators, namely, the penetration rate, i.e., the “Number of eligible patients who use the service [divided by the] number of potential patients eligible for the service”, 23 and Kangaroo Mother Care (KMC) coverage, i.e., the “Percentage of newborns initiated on facility-based KMC”. 27 Most of the indicators were provided by Weir and McCarthy (n = 24). 31
Nearly all implementation indicators could be assigned to implementation outcomes (acceptability, adoption, costs, feasibility, fidelity, and penetration) according to the conceptional model of Proctor et al. 5 None of the indicators were assigned to appropriateness or sustainability. However, Garcia-Gardenas et al. 23 addressed the implementation outcome appropriateness by three qualitative indicators, e.g., “(. . .) the perceived fit of the innovation to address the drug-related problems of the local community”. 23 These indicators did not meet our inclusion criteria. Garcia-Cardenas et al. 23 and Garner et al. 1 did the matching themselves to the model of Proctor et al., 5 and one additional outcome, service implementation efficiency, was described and measured by “[t]he degree to which the service provider improves his/her skills and abilities to provide it”. 23 The indicators of Stiles et al. 30 were directly assigned by Proctor et al. 5 ; the indicators of McCullagh et al. 28 were assigned by the authors themselves without considering Proctor et al. 5
Interestingly, fidelity (n = 22)9,23,27,31 and penetration were most frequently addressed by indicators (n = 19).1,9,23,25,27,30,31 In contrast, implementation cost 23 and service implementation efficiency 31 were addressed by only 1 indicator each. Furthermore, acceptability (n = 3),23,28 adoption (n = 9),9,27,31 and feasibility (n = 9)23,29,31 were poorly addressed by the indicators throughout the studies.
All indicators monitored a defined population, e.g., patients, health care providers, or the intervention itself. The indicators included service delivery, service use or activity completion as an endpoint, each from a defined perspective on the outcome, e.g., fidelity and penetration are measured by service delivery.1,9,23,25,27,29-31 On the one hand, service delivery, considering the outcome fidelity, is measured by a predefined standard. On the other hand, service delivery, considering the outcome penetration, is measured by the provision of the service in an area or between areas.1,9,23,25,27,29-31 In contrast, the implementation of the safety indicators 31 that addressed fidelity and feasibility were focused on inefficient service provision or activities, e.g., “[number] of incident reports for errors” 31 or “[number] of orders incorrectly entered as text orders”. 31 Nearly all identified indicators are process indicators.
Outcomes Addressed by the Indicators
Garcia-Cardenas et al. 23 aimed to describe the implementation process of a medication review and evaluation of its initial outcomes in a community pharmacy; they measured/analyzed acceptability (n = 2) on the 2 levels of patient acceptability and health care provider acceptability (general practitioners). 23 Feasibility (n = 3) was measured by several rates, such as recruitment rates, the retention of participation rates, and service offering rates. Fidelity (n = 1) was measured by the quantity, frequency, and duration of service provision. Implementation costs (n = 1) were measured regarding service provision cost and resources, and penetration (n = 1) was measured by the level of organizational integration. 23 Service implementation efficiency (n = 1) was operationalized by the degree of service provision skill improvement and measured by the needed service provision time. 23
Garner et al. 1 aimed to develop evidence-based measures to evaluate the implementation of the Adolescent Community Reinforcement Approach in stationary health care in substance abuse treatment organizations. They also aimed to examine the relationship between implementation and client outcomes. Fidelity (n = 2) and penetration (n = 2) were measured by session and procedure delivery. 1 Penetration was additionally measured by staff certification days. 1
Guenther et al. 27 aimed to develop a standardized approach to measure the implementation and progress of KMC by using a measurement framework and a core list of indicators that facilitate the monitoring of penetration. Adoption (n = 5) was measured by the number of newborns who were weighed, identified, initially assessed, discharged from or admitted to KMC. 27 Fidelity (n = 1) was measured by the number of newborns who were discharged and received follow-up per the protocol; penetration (n = 1) was measured by KMC service availability. 27
Heidkamp et al. 9 aimed to measure the implementation of Integrated Community Case Management (iCCM) (childhood illness) by implementation strength and utilization indicators. Adoption (n = 2) was measured by Health Surveillance Assistants (HSAs) who were supervised at the clinic regarding iCCM. Fidelity (n = 2) was measured by HSAs with no stockouts during a predefined period. Penetration (n = 6) was measured according to the distribution of the HSAs and by the utilization of the iCCMs: HSAs that were working or trained in iCCM or by the number of children seen by an iCCM-trained HSA. 9
Karim et al. 25 aimed to report the effects of the implementation, labeled program intensity, of a newborn survival intervention in 101 districts of Ethiopia. Penetration (n = 4) as the core outcome was measured by the period prevalence of visits of households and by the proportion of households that were a model family household or that had a family health card. 25
McCullagh et al. 28 aimed to determine the adoption rates of clinical decision support tools. Acceptability as defined by McCullagh et al. 28 was described as the use of the integrated clinical prediction rule (iCPR) (n = 1). Two other measures from the iCPR tool or smartest completion could not be categorized because of poor contextual information for the indicators. However, the outcome adoption is conceivable. 28
Saldana et al. aimed to investigate behavior in the early implementation stages regarding the prediction of a successful start of the Multidimensional Treatment Foster Care program and to measure the predictive validity of the first 3 “Stages of Implementation Completion”. 29 In this context, fidelity (n = 1) was measured by completed activities, and feasibility (n = 1) was indicated by the total time spent in the individual stage to complete the activities. 29
Stiles et al. 30 aimed to explore, conceptualize, and operationalize the indicators of service penetration. Penetration (n = 3) was measured by service use and service contact, including an overall measure of penetration that considered different time frames. 30
Weir and McCarthy 31 aimed to develop an implementation process monitoring framework by using the example of a computerized provider order entry (CPOE) that considered implementation safety indicators. Adoption (n = 2) was measured by entered orders. Fidelity (n = 15) was measured by unsigned, incorrect or discontinued orders, by unsolved problems regarding CPOE, and by the time that is needed for a predefined CPOE activity. Feasibility (n = 5) was measured by unplanned, unexpected, discontinued, and inefficient activities and penetration (n = 1) was measured according to the origin of the order. The categorization of automatically generated co-orders was unclear. 31
Proctor et al. 5 aimed to conceptualize implementation outcomes in addition to service and client outcomes. They recommended that indicator penetration (n = 1) could be measured by the service or treatment delivery by trained providers. 5
Quality of the Implementation Indicators
Only the indicators in 2 publications9,25 met 5 of the 6 quality criteria of the NQF (see Table 3). Only these publications described at least one of their indicator as scientifically acceptable.9,25,29 One publication reported related and competing measures or reference values. 27
Quality of the Implementation Indicators.

Note. Yes = the authors provided comprehensive information about the quality of the indicator (set) or explicitly stated that the criterion was met; Yes* = the quality criterion was only mentioned briefly in the publication or it was only applicable to individual indicators; No = the given information suggested that the indicator (set) did not meet the criterion; Not mentioned = there was no information in relation to the criterion.
Discussion
Although a comprehensive SR was performed, only a small number of publications and implementation indicators were identified. Several challenges of indicator-based implementation measurement and the need for new types of validated indicators were deduced.
We showed that several terms, frameworks, and models do exist for implementation measurement. This is problematic for both scientists and practitioners to identify implementation measures. 33 Some authors1,23 applied the terminology introduced by Procter et al. 5 Additionally, the term implementation strength was used. 9 Schellenberg et al. 7 also introduced the term implementation strength and added the terms implementation intensity, degree, and quality. Other authors discussed the term implementation quality.6,34 Rabin et al. 35 addressed this problem by establishing a web-based, collaborative platform to stimulate an organized exchange among scientists, physicians, and other stakeholders to evaluate and standardize the constructs and measurement tools for implementation processes.
Several authors14,36,37 have already applied or discussed the Conceptional Framework for Implementation Research of Proctor et al. 5 Throughout the last few years, they have all concluded that there is still a need for the development of an implementation framework including its related measures.14,36,37 The Context and Implementation of Complex Interventions (CICI) framework is recommended as a determinant and evaluation framework that considers the factors that influence implementation outcomes. It allows the assessment of implementation success by considering the context and setting of implementation endpoints. 37 In addition to the outcomes of Proctor et al., 5 it is suggested by Pfadenhauer et al. 37 that outcome dissemination should be added to the framework. Furthermore, service implementation efficiency is provided. 23 However, a recent discussion describes implementation outcomes in light of health care and health care services research complexity in contrast to pragmatism. 38 A redefinition of implementation success is postulated in addition to a discussion of the suitability of predetermined outcomes and process fidelity in the context of a complementary holistic view, where outcomes are emergent and measured by mixed method approaches to allow flexibility in a changing research context. 38 The identified indicators were often related to a defined context and defined processes. Not all outcomes were addressed by indicators.
It would be of interest to develop indicators that are suitable for several implementation purposes. It is argued to consider several dimensions of implementation quality, e.g., process and outcome, for implementation measurement. 6 Along these lines, the question also arises regarding how can existing measures stand up to the new debate on health care complexity and pragmatism? 38 Two of the identified studies represented a first attempt by emphasizing the need for both qualitative and quantitative indicators or describe a qualitative view on selected indicators.23,27 A combination of complementary qualitative, and quantitative indicators can be assumed. 38
We show that the publication of validated implementation indicators is lacking. Additionally, Garner et al. 1 state that the availability of a validated implementation indicators is limited. We also show that the implementation indicator references were poorly reported. If calculated reference values or reference ranges based on normative or empirical data are missing, determining experience-based values is suggested. 24 In a monitoring setting, a high sensitivity should be the aim. 13 In this regard, the present SR seeks to increase awareness of the definitions for the corresponding reference values or ranges and to maintain an awareness of the changes in implementation processes. Continuous monitoring of implementation allows the early identification of deviations and new problems. Additionally, it allows the ongoing evaluation of adaptions in the implementation efforts. 6
Finally, we identified interesting indicators of implementation safety. 31 These indicators are being developed considering changing systems, including information changes at both the system and individual levels. 31 The authors state that these types of indicators are necessary to ensure patient safety. 31
Limitations
This SR has considered approved scientific standards. According to Krippendorff, 21 an independent content analysis of the literature might minimize the risk of bias. Here, the coding was conducted by just one of the authors (T.W.); further coding and checks were conducted by another author (S.K.). In cases of uncertainty, either another reviewer or the corresponding author of the identified publication was contacted. Due to a significant number of publications that would not meet the inclusion criteria, the search string was restricted to the title. However, this served to increase precision so that the reduction in quantity was acceptable. A publication bias can be assumed, because unpublished or gray literature was excluded. However, we contacted selected authors of the included literature for further unpublished works to be considered. Although an initial assessment of the quality of the indicators was made, no final critical appraisal of the included publications was performed. It should be noted that this is not required for an SR. 16
The quality indicator description differed throughout the publications. Therefore, in some cases, it was necessary to assemble indicator components for a structured presentation.
Conclusion
Finding consensus in framing and defining implementation success and outcome measurement by implementation indicators will be a new challenge in health services research; such a consensus would facilitate the development and use of valid implementation indicators in health services research and practice. Therefore, it is essential to consider the new debates in the context of health care complexity and to the need for an efficient and targeted method of measurement. Finally, a new generation of complementary qualitative and quantitative indicators considering several dimensions of implementation quality may be needed to meet the challenges of health care complexity.
Supplemental Material
2019.05.04_Suplementary_Implementation_success_indicators – Supplemental material for Implementation Outcomes and Indicators as a New Challenge in Health Services Research: A Systematic Scoping Review
Supplemental material, 2019.05.04_Suplementary_Implementation_success_indicators for Implementation Outcomes and Indicators as a New Challenge in Health Services Research: A Systematic Scoping Review by Tabea Willmeroth, Bärbel Wesselborg and Silke Kuske in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is funded by the Fliedner Fachhochschule Duesseldorf, University of Applied Sciences.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.