
Abstract
Despite largely unproven clinical effectiveness, incentive spirometry (IS) is widely used in an effort to reduce postoperative pulmonary complications. The objective of the study is to evaluate the financial impact of implementing IS. The amount of time nurses and RTs spend each day doing IS-related activities was assessed utilizing an online survey distributed to the relevant national nursing and respiratory therapists (RT) societies along with questionnaire that was prospectively collected every day for 4 weeks at a single 10-bed cardiothoracic surgery step-down unit. Cost of RT time to teach IS use to patients and cost of nurse time spent reeducating and reminding patients to use IS were used to calculate IS implementation cost estimates per patient. Per-patient cost of IS implementation ranged from $65.30 to $240.96 for a mean 9-day step-down stay. For the 566 patients who stayed in the 10-bed step-down in 2016, the total estimated cost of implementing IS ranged from $36 959.80 to $136 383.36. Using national survey workload data, per-patient cost of IS implementation costed $107.36 (95% confidence interval [CI], $97.88-$116.98) for a hospital stay of 4.5 days. For the 9.7 million inpatient surgeries performed annually in the United States, the total annual cost of implementing postoperative IS is estimated to be $1.04 billion (95% CI, $949.4 million-$1.13 billion). The cost of implementing IS is substantial. Further efficacy studies are necessary to determine whether the cost is justifiable.
Keywords
Despite largely unproven clinical effectiveness, incentive spirometry (IS) is widely used in an effort to reduce postoperative pulmonary complications.
The current cost of implementing IS is substantial.
Further clinical effectiveness studies are necessary to determine whether the cost of IS is justifiable.
Introduction
Implementation of incentive spirometry (IS) involves a team of providers including physicians, respiratory therapists (RT), and nurses. 1 Clinical practice guidelines recommend IS usage in acute care inpatient, skilled nursing facility, extended care, and home care settings to optimize pulmonary function. 2 IS has been reported to be used in 95% of US hospitals after surgery. 3 Most commonly, RT lead initial patient education on IS use, followed by nurse reeducation and reminding. Provider time and costs of IS implementation have not previously been reported.
Despite widespread use of IS, there is a paucity of data demonstrating therapeutic value.4-22 One systematic review 23 stated, “Presently, the evidence does not support the use of IS for decreasing the incidence of postoperative pulmonary complications.” Another combined analysis 16 concluded, “routine use of respiratory physiotherapy after abdominal surgery does not seem to be justified.” The most recent meta-analyses found “no evidence” of benefit from IS.24-26 Last, the American Association For Respiratory Care (AARC) Clinical Practice Guideline: Incentive Spirometry: 2011 2 states that “evidence strongly suggests that IS alone may be inappropriate to prevent or treat postoperative complications.”
In an increasingly cost-conscious health care environment,27-33 the goal of this study was to assess the costs of implementing IS.
Methods
Installation Costs
To assess the amount of time spent by RTs on IS-related activities, an IRB (Institutional Review Board)-approved, secure online survey was created and distributed via social media and newsletters by the AARC, from September to December 2016. As a complementary analysis, the survey was also distributed to RTs at a single academic medical center (AMC). Survey results were de-identified.
RTs national hourly wage data were gathered from the U.S. Department of Labor (2015). Using the latest Consumer Price Index data from the U.S. Department of Labor Bureau of Labor Statistic, wages were inflation-adjusted to 2017 dollars. 34 RTs’ per-minute wage was calculated by dividing hourly wage by 60 minutes.
Individual IS unit (4000 mL Coach 2 [Smiths Medical, Saint Paul, Minnesota]) cost was determined based on the wholesale case price paid to the hospital supplier by AMC. 35 This commonly used IS model represents the IS device type recommended by the AARC. 2
Maintenance Costs
To assess the amount of time spent per patient by nurses on IS-related activities, an IRB-approved, secure online survey, as described, was distributed via social media and newsletters by the following national nursing societies from September to December 2016: Academy of Medical-Surgical Nurses (AMSN), American Association of Critical-Care Nurses (AACN), and American Society of Peri-Anesthesia Nurses (ASPAN). The survey was also distributed to the nurses at the AMC. Survey results were de-identified.
Questionnaires on IS workload were prospectively collected every day for 4 weeks in December 2016 from nurses on a 10-bed cardiothoracic surgery step-down unit at the AMC. On that unit, nursing orders for IS are “Routine, Now then every 4 hours.” IS orders are bundled as part of the admission order set, specifically requiring opt-out for exclusion. Surveys were collected at 6:45
Registered nurses’ national hourly wage data were gathered from the Bureau of Labor Statistics of the U.S. Department of Labor (2011) and 2017 inflation-adjusted numbers. 34 Nurses’ per-minute wage is calculated by dividing hourly wage by 60 minutes.
Calculations
The following equation was used to calculate IS implementation costs per patient (Table 1):
Estimating Equation Cost Per Patient.

Note. IS = incentive spirometry; RTs = respiratory therapists.
The data from the AMC study were used to estimate the annual cost of IS implementation on the 10-bed cardiothoracic surgery step-down unit. Annual costs for implementing IS in the United States were estimated using national mean hospital length of stay (4.5 days), 37 number of inpatient surgeries per year (9.7 million), 38 and provider time spent doing IS-related activities from our national surveys. Point and interval estimates of time were calculated using a generalized linear model assuming a negative binomial distribution using SAS/GLIMMIX 9.4 (SAS Inc, Cary, North Carolina). Microsoft Excel (Microsoft Corporation, Redmond, Washington) was used for standard data analysis.
Results
Installation Costs
There were a total of 416 unique respondents from the AARC and 19 from the AMC with various educational backgrounds, years of experience, and primary practice locations (Table 2). Survey completion rates were 80.3% for AARC and 78.9% for AMC. Given the distribution methodology, response rate cannot be determined due to the inability to identify the total number of individuals the survey may have reached. AARC respondents reported spending an average of 16.4 (95% confidence interval [CI], 14.7-18.4) minutes per 8-hour shift educating or reminding patients to use IS, equating to 2.1 (95% CI, 1.8-2.3) minutes per hour. AMC RT respondents reported an average of 21.6 (95% CI, 1.1-42.2) minutes per 8-hour shift, equating to 2.7 (95% CI, 0.1-5.3) minutes per hour. There was no significant difference between AMC and AARC times spent educating or reminding patients (P = .5349).
RT Survey Respondent Characteristics.
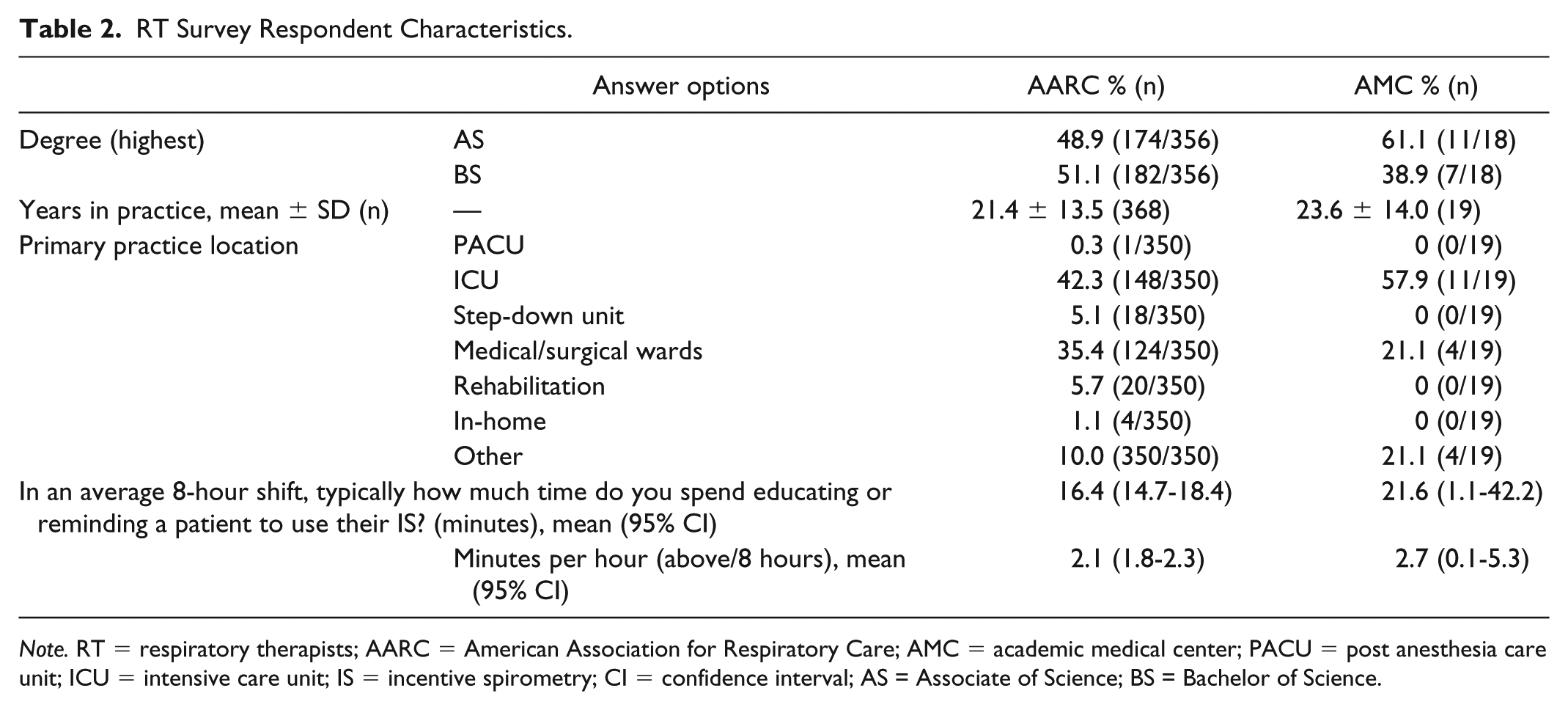
Note. RT = respiratory therapists; AARC = American Association for Respiratory Care; AMC = academic medical center; PACU = post anesthesia care unit; ICU = intensive care unit; IS = incentive spirometry; CI = confidence interval; AS = Associate of Science; BS = Bachelor of Science.
RTs’ national 2017-adjusted mean per-minute wage is $0.49 ($29.37/60 min). Individual IS unit cost was $12.92.
Maintenance Costs
There were a total of 1265 unique respondents from the ASPAN, AMSN, and AACN and 126 from the AMC. Survey completion rates were 84.3% for ASPAN, 84.8% for AMSN, 90.1% for AACN, and 84.9% for AMC. The respondents included nurses with various educational backgrounds, years of experience, and primary practice locations (Table 3). Given the distribution methodology, response rate cannot be determined due to the inability to identify the total number of individuals the survey may have reached. Combined national society (ASPAN, AMSN, AACN) respondents reported spending an average of 15.8 (95% CI, 14.5-17.2) minutes per 8-hour shift educating or reminding patients to use their ISs, equating to 2.0 (95% CI, 1.8-2.2) minutes per hour. AMC nurse respondents reported an average of 15.1 (95% CI, 11.4-18.9) minutes per 8-hour shift, equating to 1.9 (95% CI, 1.4-2.4) minutes per hour. There was no significant difference between AMC and aggregated nursing society times spent educating or reminding patients (P = .7465).
Nurse Survey Respondent Characteristics.

Note. ASPAN = American Society of Peri-Anesthesia Nurses; AMSN = Academy of Medical-Surgical Nurses; AACN = American Association of Critical-Care Nurses; AMC = academic medical center; PACU = post anesthesia care unit; ICU = intensive care unit; IS = incentive spirometry; CI = confidence interval; AND = Associate’s degree in Nursing; LPN = licensed practical nurse; BSN = bachelor of science in nursing; MSN = Master’s of Science degree in Nursing; DNP = Doctor of Nursing Practice.
A total of 217 questionnaires from 23 the AMC step-down unit nurses were prospectively collected, representing a 100% response rate. Nurses reported spending on average 8.8 (95% CI, 7.8-9.9) minutes per 12-hours shift, equating to 0.7 (95% CI, 0.6-0.8) minutes per hour educating or reminding patients to use their ISs. In 2016, there were 566 patients, who each spent an average of 9 days on the AMC step-down unit.
Registered nurses’ national 2017-adjusted mean per-minute wage is $0.60 ($35.87/60 min).
Implementation Cost Estimates
Incorporating mean data into the estimating equation, the new estimating equation is simplified (Table 4).
Simplified Cost Estimating Equation of Per Patient.

Note. IS = incentive spirometry; RTs = respiratory therapists.
Using AMC mean data, per-patient cost of IS implementation ranged from $65.30 to $240.96 (Table 5). For the 566 patients who stayed in the AMC’s 10-bed cardiothoracic step-down unit in 2016, total annual costs of implementing IS ranged from $36 959.80 to $136 383.36.
Per-Patient IS Implementation Cost Estimates Using AMC Data.
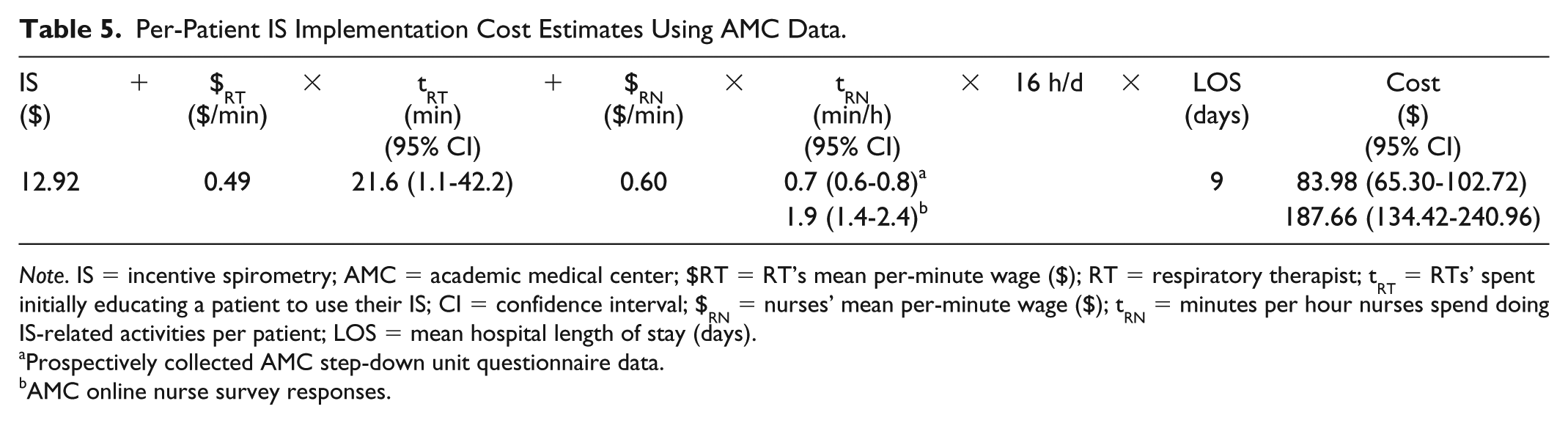
Note. IS = incentive spirometry; AMC = academic medical center; $RT = RT’s mean per-minute wage ($); RT = respiratory therapist; tRT = RTs’ spent initially educating a patient to use their IS; CI = confidence interval; $RN = nurses’ mean per-minute wage ($); tRN = minutes per hour nurses spend doing IS-related activities per patient; LOS = mean hospital length of stay (days).
Prospectively collected AMC step-down unit questionnaire data.
AMC online nurse survey responses.
Using national survey mean data, per-patient cost of IS implementation costs $107.36 (95% CI, $97.88-$116.98) (Table 6). For the 9.7 million inpatient surgeries performed annually in the Unites States (Project HCaU, 2015), total annual cost of implementing IS is $1.04 billion (95% CI, $949.4 million-$1.13 billion).
Per-Patient IS Implementation Cost Estimates Using National Survey Data.

Note. IS = incentive spirometry; $RT = RT’s mean per-minute wage ($); RT = respiratory therapist; tRT = RTs’ spent initially educating a patient to use their IS; CI = confidence interval; $RN = nurses’ mean per-minute wage ($); tRN = minutes per hour nurses spend doing IS-related activities per patient; LOS = mean hospital length of stay (days).
Discussion
This study estimated the cost of implementing IS. IS is used in more than 95% of hospitals across the United States, even though no clear clinical or cost benefit has been documented. The current study attempted to define the cost of using IS in an academic cardiothoracic surgery step-down unit and correlate those data with the national average costs. To accomplish that, a survey was conducted at AMC and nationally by targeting relevant nursing and respiratory therapy organizations.
Nurses and RTs report spending a substantial portion of their time performing IS-related activities. This is the first study to report IS implementation cost per patient (⩾$65.30), annual cost per a 10-bed cardiothoracic step-down unit at AMC (⩾$36 959.80), and annual expenditures in the United States (⩾$949.4 million). Provider time dedicated to IS was not significantly different between the AMC and national survey responses, validating the accuracy of the cost analysis.
Despite a dearth of evidence in reducing postoperative pulmonary complications, IS began to be prescribed in the 1970s after intermittent positive pressure breathing was proven therapeutically ineffective. 36 In addition to IS’s benign safety profile 2 and physicians’ lack of knowledge regarding costs,39-42 the relatively low per-patient financial impact of implementation may explain why IS continues to be so widely prescribed today relative to the lack of evidence establishing its benefit. Until now, IS-prescribing physicians had no data on the time and effort required of nurses and RTs to implement IS. When compared directly with costs of other tests or interventions, IS may appear relatively low. However, when implementation is considered at the step-down unit, hospital, or nationwide levels, the estimated $1.04 billion cost spent on IS in the United States is substantial, especially given the lack of efficacy data.
As health care costs continue to rise in an unsustainable fashion, so does the need to cut out wasteful spending. 43 Per Berwick et al, major sources of waste in medicine include (1) failures of care delivery, (2) failures of care coordination, (3) overtreatment, (4) administrative complexity, (5) pricing failures, and (6) fraud and abuse. 43 Until now, IS-prescribing physicians had no data on the time and effort required of nurses and RTs to implement IS. In 2008, health care expenditure totaled $2.4 trillion comprising 16% of the US gross domestic product. 44 However, when implementation is considered at the step-down unit, hospital, or nationwide levels, the estimated $1.04 billion cost spent on IS in the United States is substantial, especially given the lack of efficacy data. IS falls into the category, as delineated by Berwick et al, of “Overtreatment”—when patients are subjected to care not necessarily grounded in literature or science. 43 Other examples of overtreatment include excessive use of antibiotics, excessive and even unwanted care toward the end of life, and the use of expensive, more lucrative, treatment modalities which conservative treatment is sufficient. 43 The category of “Overtreatment” as a whole is thought to comprise between 158 and 226 billion dollars of wasteful spending.
This study has several potential limitations. National survey respondents were members of professional societies, which may have created a sampling bias of individuals who tend to have certain perspectives. Surveys ideally would be distributed nationwide to all RTs and nurses. Whether respondents had an Master of Science in Respiratory Care degree was not surveyed. Time reported by providers is subjectively recollected and may be influenced by recall bias. The ideal observation method would be quantified provider time measured via video recording; however, implementation of such procedures is not realistic. Last, the local survey was performed in a cardiothoracic step-down unit, and estimates may not be generalizable to all inpatient bed or other types of step-down units. More data are needed regarding specific uses, costs, efficacy, and compliance. Without adequate clinical efficacy data, whether or not IS should continue to be prescribed warrants consideration. As overall costs of health care continue to rise, 29 allocation of resources to early mobilization45,46 and optimizing pain control,47-56 as well as other evidence-based therapies, may be more appropriate.
IS makes clinical sense but has limited support in the literature and is associated with very high costs. The current data highlight a broader need for greater critical inquiry concerning the evidence supporting and costs associated with common medical practices in an effort to avoid unnecessary spending and optimize quality care. Further studies are needed to determine clinical efficacy and cost-effectiveness of IS to determine whether costs are justifiable.
Footnotes
Acknowledgements
For distributing the survey, special thanks to the national societies mentioned.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Several hypotheses are being explored from the data from the survey to the national societies (American Society of Peri-Anesthesia Nurses [ASPAN], American Association For Respiratory Care [AARC], Academy of Medical-Surgical Nurses [AMSN], American Association of Critical-Care Nurses [AACN]), with articles under consideration elsewhere related to providers’ perspectives on incentive spirometry (IS), IS use protocols, and IS use compliance. Although the respondents are the same, the hypotheses and most variables under investigation are distinct necessitating separation of discussion. Dr. Daniels reports relationships with DePuy, Globus Medical, Orthofix, Springer, and Stryker. Dr. Eltorai reports relationships with Springer, Quitbit, and Lippincott and being listed as an inventor on the patent application related to the reminder. Dr. Sellke reports a relationship with Stryker and Boehringer Ingelheim. The other authors report no conflicts.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.