
Abstract
The aim of this article is to present an artifact for evaluating the quality and performance of service providers in the field of health care: the UNIPLUS Program. To verify the scientific nature of the artifact and ensure that it meets the criteria set by the community and the environment, the premises of Design Science Research (DSR) were used. As this research field lacks empirical evidence, the artifact was tested from 2013 to 2015 with 25 health care service providers from different categories, with an emphasis on hospitals and clinics located in 7 cities in the south of Brazil. This article makes 3 main contributions to the field: (1) the artifact can be applied to any health insurance operator in Brazil and other countries, as it meets the legal norms and requirements established by current legislation; (2) it helps health service providers by generating information that identifies shortfalls and possibilities for improvement for every aspect analyzed in the evaluation process; and (3) it uses the DSR methodology in an evaluation artifact that evaluates the quality and performance of services in the field of health care. The artifact proved to be adequate for the purpose in question, helping to improve the quality of care and institutional performance.
Keywords
Methods of assessing the quality of health service delivery exist, but are not shared.
It presents a complete methodology that can be applied anywhere in the world by adjusting to local legislation.
It contributes in a theoretical way in the presentation of an artifact and of practical form in the applicability of this artifact.
Introduction
Health insurance companies provide health care services in Brazil to approximately 25% of the population through their accredited network. 1 This network is composed of hospitals, clinics, diagnostic and therapeutic support services, and freelance professionals. In the 1990s, the public health care service became concerned with assessing the quality of the services provided. 2
In Paraná State, until 1999, the system adopted by self-managed operators was empirical and classificatory. At this time, a group of technicians from the fields of health and management prepared an assessment model for hospitals and clinics called the Paraná State Health Service Assessment Program (PROPASS PLUS), which was implemented for 12 years in the state. 3 In 2012, the program required upgrades in its technical and methodological validation criteria to ensure the quality of the results and maintain its applicability. The result was the UNIPLUS Program, consisting of a quality assessment method for the National Union of Self-managed Healthcare Institutions (UNIDAS).3 The research question of this study is as follows:
The aim of this article is to present the artifact known as the UNIPLUS Program as a method for assessing the quality and performance of health care providers that generate daily rates and fees, based on the groundings of Design Science Research (DSR). As the essential requirement for the evaluation of the artifact in accordance with DSR is its practical applicability to solve a problem and its adaptation to the conditions of the environment, the contribution emerges from the utility of the artifact. The results of the application of DSR are defined as an artifact. 4
The specific objectives of this study are to present an artifact that can be applied in any health insurance company in Brazil and abroad, assess whether the artifact is capable of demonstrating deficiencies and possible improvements in the processes of health service providers, and identify the different levels of quality of care and institutional performance of health service providers.
The artifact aids the supplementary health system, representing the assessment of indicators of quality assistance and institutional performance in the dimensions of patient safety, centrality and communication, and efficiency and effectiveness. For operators, it enables managers to access the dossier of evaluated hospitals, aiding the choice of quality in the network of each provider. Moreover, it promotes strategic alliances between health care service operators and providers evaluated by the UNIPLUS Program. For the evaluated health care service providers, it provides information that allows a review of standards of compliance, enabling better levels of payment for the evaluated entities when they achieve higher levels of sufficiency. For beneficiaries, it increases the power of evaluation and the choice of network offered by the health insurance operator.
The present study is structured as follows. The “Literature Research” section presents the literature research, highlighting supplementary health and health service quality. The “Study Data and Methods” section presents the study data and methods, DSR, and DSR method applied to the UNIPLUS Program. The “Analysis” section presents the steps 1 to 3 of the DSR method. The “Results” section presents steps 4 and 5 of the DSR method. The conclusions, limitations and suggestions for future studies are outlined in the “Conclusions” section.
Literature Research
Supplementary Health Care in Brazil
Brazil, in the late 1980s, underwent profound changes that culminated in the promulgation of the Federal Constitution of 1988. According to Article 199 of the Constitution, “healthcare is open to the private sector.” This, in combination with the crisis in the public health care system, spurred the expansion of the private health care sector in the country.5-7
Law 9.656 8 was passed to maintain the equilibrium between competing health insurance plans and ensure services were provided to consumers. Law 9.961 9 created the National Supplementary Health Agency (ANS) to defend the interests of public supplementary health care and regulate insurance companies in terms of the relationships between health service providers and consumers. 10
A total of 1370 health insurance companies provided services, in 2015, to 50 261 602 consumers, representing 25% of the Brazilian population. The ANS classified the insurance companies according to their medical/hospital services or dental services as Administrators, Self-managed, Medical Cooperatives, Philanthropic, Specialist Health Insurance Companies, Group Medicine, Group Dentistry, and Dental Cooperatives. 1
In addition to the ANS, the supplementary health market functions as a joint complex of actors who interact with one another to defend their interests. The health insurance companies structure their services and hire health service providers to treat their customers. The insurance companies are represented by a number of national organizations, including the National Union of Self-managed Health Institutions (UNIDAS). 11
Health service providers include doctors, clinics, hospitals, and diagnostic and therapeutic services. They provide assistance to health insurance customers and are later paid for their services by the insurance companies. They are represented by a number of national organizations such as the Brazilian Federation of Hospitals, the Brazilian Medical Association, and the Brazilian Society of Clinical Pathology and Laboratory Medicine. 11 Health insurance consumers, who hire and use health care services, are represented by National Consumer and Beneficiary Defense Organizations. 11
Since it was first established, the ANS has implemented a number of norms that range from legislation to structure the sector to rules for inspection and maintenance of health insurance companies, the standardization of health care, and minimum coverage for users. Recently, the agency has focused on assessing the quality of private hospital health services.
The ANS has established rules regarding the quality of the network of health insurance operators, linked to the remuneration of health service providers. With a biannual regulatory agenda, the ANS has set as one of its points for 2016-2018 a “Guarantee of Access and Quality in Healthcare,” with a view to ensuring quality care and access to health care services when required.
Quality Assessment of Health Care Services
In a competitive market, quality can be defined as a set of attributes that are essential to the survival of health service providers.12-14 Donabedian15,16 proposed the systematization of knowledge on quality. The proposal standardizes the concepts and nomenclature with a unified model for the assessment of quality in health, including 3 health care components:
Structure: This includes the physical, human, and organization conditions in which care is begun and concluded. In this requirement, the presence and adaptation of equipment are evaluated, including physical space, installations, inputs, human, material and financial resources required, and the availability of qualified workers. A good structure does not guarantee good care.
Process: This is where the interrelation between health service provider and patient occurs. It is the dynamic of health care, including indicators, requests of examinations, listening to the patient, checking examinations, examining the patient, and executing procedures.
Result: The end product of the health care process, considering health as the mode for gauging satisfaction in terms of standards and expectations. It is the changing state of the patient’s health, which can be attributed to this care (attributable validity). It is the most difficult feature of health care to evaluate and includes indicators such as cure, side effects, adaptation to the environment, discomfort, mortality, morbidity, functional state, state of health, and quality of life.
The indicators are important for quality assessment. They provide a measure, enable monitoring, and help to identify opportunities for the ongoing improvement of services. These indicators reflect positive changes to achieve quality at a reasonable cost. 17
The assessment of quality in the field of health care shows a number of difficulties. The managers are unanimous in their view that this assessment needs a choice of evaluation systems and adequate institutional performance indicators. These in turn aid the administration of services and decision-making with the lowest possible level of uncertainty. 18
Methods for Assessing the Quality of Private Health Services in Brazil
In Brazil, the most important recognized certification agencies for health care quality assessment are (1) the National Accreditation Organization (ONA) (www.ona.org.br); (2) Accreditation Canada, maintained and implemented by the Qualisa Management Institute (IQG) (www2.iqg.com.br); (3) Joint Commission International (pt.jointcommissioninternational.org); (4) ISO 9001, recognized internationally, generic and applicable to any health care service and health insurance company; and (5) Program for Publishing the Qualification of Supplementary Health Service Providers of the National Supplementary Health Agency (QUALISS). 19
Following the promulgation of the Brazilian Federal Constitution of 1988, accreditation programs in Brazil became more relevant. In the public health system, hospitals came to play a more highlighted role in the network and management. The focus shifted to evaluating the quality of services offered to the population.
Based on the policy of incentives to improve the quality of management and health care, in 1977, a number of quality assessment initiatives arose, such as the Brazilian Hospital Accreditation Manual, which was initially published for the public health service. In 1999, the ONA was established. A health care provider is accredited when it complies with the accreditation standards, assuming that this compliance means that a good quality service is provided. 20
Study Data and Methods
Design Science Research
To do science, a scientific method with the basic instruments is necessary. These help the scientist in an orderly manner from the outset and throughout the process to achieve the goals of the study. 21 Through a research method, 22 consider DSR as a set of steps recognized by the academic community and used by researchers to construct scientific knowledge. Thus, DSR is a rigorous process for projecting artifacts to resolve problems, evaluate what has been projected or what is working, and report the results obtained.23,24
To conduct DSR, stages or steps of the process are followed that result in output. The first stage is awareness of the problem to gain a broad understanding of it to define what needs to be solved. The second stage is suggestion, in which protocols are developed to ensure the internal validity of the research and enable its traceability. 25-27 The model must comply with a world that is closer to reality. 28 In the third stage, the constitution process of the artifact itself occurs,4,29,30 resulting in the artifact in a functional state.25-27
The fourth stage is the assessment, which consists of a rigorous verification process of the behavior of the artifact n the environment for which it was projected in terms of the solutions it was proposed to achieve.25,29 A series of procedures is required to verify the performance of the artifact. The main results of the assessment process are the prior descriptions, the performance measurements to prove the adequacy of the UNIPLUS Program. The fifth stage is the conclusion, which consists of the general formalization of the process and conveying it to the academic and professional communities.25,26,29
The use of an approach grounded in a review of the literature on the method in question presents the UNIPLUS Program in detail, adapted to the set of stages recognized by the academic community to construct scientific knowledge and project artifacts to resolve problems as recommended by DSR. The choice of this method confers a scientific nature and justifies that the articles meet the criteria set by the environment and the community in which they function.
For the accomplishment of this exploratory study, with bibliographical review and extensive documentary analysis was developed with 25 health service providers in different cities and categories and 613 forms were analyzed completely in the process between 2013 and 2015.
The DSR Method Applied to the UNIPLUS Program
The methodology used for this article is DSR.25,29 From this perspective, the article shows how the UNIPLUS Program was conducted with a view to justifying its legitimacy using a rigorous and appropriate methodological approach. The presentation of the UNIPLUS Program follows the points that are explained throughout the stages of DSR.4,25 Each item in the results represents a DSR stage, the last stage being the accomplishment of this research. The methodological procedures, the detailed operationalization criteria, and the results of the UNIPLUS Program are described below.
Analysis
Step 1: State of Awareness of the UNIPLUS Program
In Brazil, from the early stages of supplementary health, the organization of the network and the provision of services is structured to meet the needs of the beneficiaries. 7 To provide complete health care services to their users, health insurance companies engage the services of hospitals, clinics, freelance professionals, and diagnostic and therapeutic services.
The health insurance companies that operate on the Brazilian market have distinct characteristics and are members of specific associations. Self-managed companies are responsible for the administration of the specific health insurance plans of their employees, workers, or members and their dependents. Self-managed companies cannot commercialize their health plans and are not for profit. 1
In 1999, in Paraná State, self-managed companies were members of the Association of Self-managed Organizations of Paraná (ASSEPAS). One of the aims of this association was to negotiate with health care service providers for the self-management sector.
For hospital service providers and clinics that charge daily rates and fees, the greatest difficulty was the classification system of assessment created and implemented empirically by these providers. This classification system ended with a table for the payment of hospitals and clinics using a fee-for-service system. This system is characterized by payment for service providers per item. It encourages the use of services and increases the cost of health care without resulting in better quality health care for patients.30,31
In the 1990s, there were no consolidated programs for patients and private health service providers to evaluate the quality of supplementary care, with performance measurements and specific goals. 31 A systematic review 32 showed that it was only in 2004 in Brazil that publications began to appear regarding the quality of processes in hospitals, the results of health care, the resources for the structure and availability of professionals, and an adequate environment for the provision of health care services.
In 1999, to solve the problem of assessment and payment of health service providers, a group of technicians in the field of health and administration working for the ASSEPAS prepared a quality assessment program for hospitals and clinics for use by self-managed operators. The method was named the Paraná State Health Service Assessment Program (PROPASS PLUS).
From 1999 to 2011, the PROPASS PLUS was implemented at 113 hospitals and clinics accredited by self-managed health insurance operators that were members of the ASSEPAS. The PROPASS PLUS evaluated the hospitals and clinics and established a benchmark of values in the system for an “improved open account.” This improved open account was characterized by the reduction of items that were charged in the form of daily rates and fees, simplifying the billing process and adjusting the distribution of hospital costs.
With the dissolution of the ASSEPAS in 2012, the self-managed insurance companies in Paraná State joined the National Union of Self-managed Healthcare Institutions (UNIDAS). UNIDAS is made up of 130 companies with approximately 4 800 000 beneficiaries all over the country. It has 27 State Superintendent Offices in each state capital in the country.
Step 2: Suggestion Stage of the UNIPLUS Program
When substituting the PROPASS PLUS, it was necessary to construct an artifact called the Assessment Program for Health Service Providers (UNIPLUS Program). The premises for the construction of the UNIPLUS Program include (1) regulatory norms of the National Sanitation Inspection Agency (ANVISA); (2) norms of the Ministry of health and the World Health Organization for patient safety; (3) qualification criteria of health service providers of the ANS and organizations that represent hospitals; (4) goals of the UNIDAS regarding health care and the optimization of costs for its members, 33 and (5) Donabedian’s premises of quality.15,16
As requirements for constructing the UNIPLUS Program, 17 categories of hospitals and clinics were created, as shown in Table 1. A hierarchy was created for the assessment of health service providers, as shown in Figure 1. The category of health service provider allows each provider to be assessed according to the peculiarities of each category.
Requirements for Constructing the UNIPLUS Program by Category of Hospital and Clinic.

Source. UNIDAS, UNIPLUS program. 3

Requirements for constructing the UNIPLUS Program by assessment hierarchy.
The design of the UNIPLUS Program has its own regulations containing all the norms from the registration to the certification of the provider. As shown in Figure 1, the first criterion for defining the evaluation is the categorization of the high complexity, general and specialist hospitals or clinics. From this categorization, the sectors or units are to be assessed, whether compulsory or not, in accordance with the Service Provider Manual available from the Unidas portal (http://www.unidas.org.br/uniplus). Finally, specific evaluation forms were prepared with three domains: (1) structure, (2) processes, and (3) results. In each domain, there are types of questions that represent the standard of compliance to be observed by the evaluating team during the evaluation visit.
Step 3: Development State of the UNIPLUS Program
The main objective of the UNIPLUS Program is to assess and monitor the quality of care and the institutional performance of the health service providers. 3 To standardize the UNIPLUS program artifact, a regimen was created to define the general functioning norms of the program approved by the UNIDAS and its legal team. The actors involved in the UNIPLUS program include the members and administrative team of the UNIDAS, a trained and outsourced assessment team, and the hospitals and clinics that charge daily rates and fees.
Participation in the UNIPLUS Program is voluntary, provided the eligibility criteria are met: (1) License to work as a health service provider issued by the city government; (2) Sanitation license; and (iii) Registration with the National Registry of Healthcare Establishments (CNES). The evaluation of the units of the UNIPLUS Program is conditioned to the sectors or services included on the Registration Form. In accordance with the category of the health service provider, the program has minimum compulsory sectors. Each assessment form was created with standard scripts according to the available units/services of the hospital or clinic. The questions were selected to translate the reality of the health service providers that are assessed in terms of the quality of the care they provide, the performance of each sector, and the performance of the institution.
The scope of each form contains selected questions divided into 3 domains: structure, processes, and results, as shown in Figure 2, with evaluation requirements distributed in questions that assess operational processes, guidelines and clinical assistance protocols, indicators, physical, human, and material resources. The number of forms for assessing the health service provider is conditioned by the category of services available. There is a maximum number of forms according to the category of the health service provider, as shown in Table 2.

Domains of the UNIPLUS Program assessment forms.
Maximum Number of Assessment Forms of the UNIPLUS Program Per Category of Health Service Provider.

Source. Assessment forms of the UNIPLUS Program. 3
The number of forms for assessing the health service provider is conditioned by the category of services available. There is a maximum number of forms according to the category of the health service provider, as shown in Table 2.
The forms are completed in the field by the assessment team, and the administrative team of the UNIDAS does the scoring. The assessment data are transcribed onto electronic Excel spreadsheets, prepared to proceed to the scoring of each unit and its respective sectors or services. The scoring criteria have different weights for each type of unit, sector, or service and type of question. The sectors for direct assistance for patients, the questions of the work process domain, quality assessment, and institutional performance indicators carry more weight in the scoring process, as shown in Figure 3.

Example of the general distribution of possible percentage points per domain of the Hospital category.
With the scoring for each form finalized, using Excel software, a comparison is made between the possible points and points obtained in the assessment and the calculation of the Final Sufficiency Index measured in percentages, per sector and service provider, as shown in the example given in Table 3.
Example of the Result of the Final Sufficiency Index of the Health Service Provider.
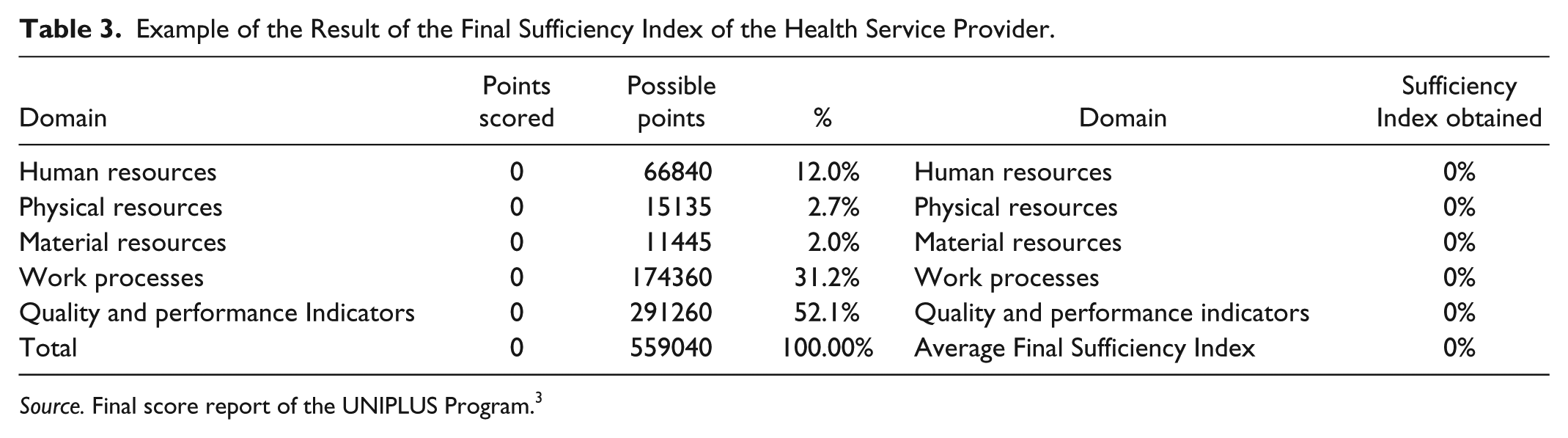
Source. Final score report of the UNIPLUS Program. 3
The Final Sufficiency Index of the Health Service Provider allows it to be included in 1 of the 5 UNIPLUS Program performance levels. The levels range from “A” to “E,” as shown in Table 4. Level “A” service providers have the best performance, while Level “E” providers have the poorest.
Framework of the Sufficiency Index by Category of Hospital or Clinic.

Source. UNIPLUS Program 3 .
Note. HAC = high complexity hospital; HG = general hospital; HE = specialist hospital; HEPsiq = hospital specializing in psychiatry; CG = general clinic; CE = specialist clinic; CEPsiq = clinic specializing in psychiatry.
With the result of the performance level, UNIDAS awards a UNIPLUS Program Certificate, valid for 3 years. During this time, annual monitoring takes place, using performance indicators. The monitoring focuses on the maintenance of care quality and performance. The results of the current evaluations are available for public access under the heading “Certified Providers,” available at http://www.unidas.org.br/uniplus.
The UNIPLUS Program also has reports for internal monitoring of the performance of the evaluating team and the evaluated health service providers. The communication of the UNIPLUS Program includes 2 groups of actors: (1) the clinics and hospitals receive an assessment certificate from the UNIPLUS Program and a detailed Final Assessment Report with the “non-conformities” identified; (2) the self-managed companies are advised of the Sufficiency Index and category of the hospital or clinic. The communication for the recognition of the academic community and society in general includes a scientific publication, such as this article. The UNIPLUS Program was tested previously at 2 volunteer High Complexity Hospitals, enabling adjustments to be made to the definitive implementation of the program.
Results
Step 4: Assessment and Results Stage of the UNIPLUS Program
To evaluate the artifact, the observational and analytical evaluation proposed by Lacerda et al 25 were used. The observational evaluation consists of monitoring the use of the artifact in multiple projects. This was done between 2013 and 2015 with 25 health service providers in different cities and categories, as shown in Table 5 and Figure 4. The data were collected from the Registration Forms of the Scoring Reports and Final Assessment Reports of each health service provider. The quantitative analysis of the results was conducted following the compilation of the Excel data. It was concluded that the UNIPLUS Program complies with the initially projected metrics and objectives.
Distribution of the Category of Health Service Providers Assessed by the UNIPLUS Program.

Source. Assessment Forms per sector and final score report for each health service provider evaluated by the UNIPLUS Program. 3

Distribution of hospitals and clinics evaluated by the UNIPLUS Program by city.
The hospitals and clinics that were evaluated had different performance levels according to the level of sufficiency achieved, as shown in Figure 5. The standards of compliance in the structure, processes, and results showed that the health service providers being evaluated, although grouped in the same category, achieved different performance levels. For example, Level A highly complex hospitals accounted for 44% of the hospitals that were evaluated, while Level B high complexity hospitals made up 4%. This was also the case for the general hospitals, specialist hospitals, and clinics.

Level of performance of the health service providers assessed by the UNIPLUS Program by category of provider.
Figure 6 shows the results of health service providers evaluated in 2 domains: (1) structure: human resources, physical resources, and material resources; (2) processes and results: operational processes, protocols, and clinical guidelines and results indicators and institutional performance.

Results of hospital and clinical evaluations in the structure and process/results domains.
It is noteworthy that of the health service providers evaluated, 17 presented higher percentage results in the domain structure when compared with the domain processes and results. Considering that the domain processes and results is directly related to the quality of the service provider and performance, it is possible to realize that the investment in the structural domain is prioritized to the detriment of the domain processes and results. For buyers, these results are relevant when they decide to buy/contract services. For providers, these same results contribute to the definition of investment strategies in areas that may affect the quality of the assistance offered. This is just one of the possible analyzes that can support decision-making.
Step 5: Conclusion and General Formalization of the Process of the UNIPLUS Program
For the analytical evaluation of the UNIPLUS Program, 613 forms were complete in the process to identify “non-conformities.” The UNIPLUS Program and its respective forms are applied to the proposed categories of health service providers. and the peculiarities of each provider are confirmed. The UNIPLUS Program does not assess the protocols and clinical directives adopted by the medical teams in question. The program scores the health service providers on these questions if they are evaluated by other certifying organizations such as the Joint Commission International and the ONA.
Recommended adjustments of the UNIPLUS Program include a technical view that increases the number of quality, performance, and process indicators of the multidisciplinary health care team.
The UNIPLUS Program is limited to hospitals and clinics that charge daily rates and fees. It is not applicable to doctors’ surgeries and clinics that provide diagnostic and therapeutic support services.
Conclusions
This article aimed to present an artifact for assessing the quality and performance of health care service providers, the UNIPLUS Program. For this purpose, an approach found on the literature review was used that presents the UNIPLUS Program in detail and adapted to the set of steps recognized by the academic community for the construction of scientific knowledge and to project artifacts to solve problems as recommended by DSR.
From a practical viewpoint, the artifact was tested on 25 hospitals and clinics in Paraná State and proved to be adequate for evaluating the quality of care and the performance of service providers that charge daily rates and fees. The main contribution of the study is the presentation of the artifact and its possible application to any health insurance company in Brazil and other countries, as it accurately meets all the norms of current legislation. In the same way that the program was created to comply with the norms of the Brazilian Ministry of Health, the National Health Surveillance Agency, and the National Health Agency, health care professionals and companies can implement the program by adapting it to the norms of each country. This study also the evaluated helps health service providers, supporting them with information that identifies shortfalls and possible improvements in each aspect analyzed in the assessment process.
The UNIPLUS Program artifact facilitates the selection and negotiation of self-managed health insurance companies with the accredited network. The artifact also identifies different levels of quality of care and the institutional performance of health care service providers. Furthermore, it enables a reduction in expenditure on technical professionals to evaluate the level of the health care service providers in accordance with requirements, promoting strategic alliances between self-managed operators the evaluated providers of health care services.
With the UNIPLUS Program, the Union of Self-management Healthcare Institutions (Unidas) was recognized as a Managing Entity of Other Quality Programs in the QUALISS (Qualification Program of Healthcare Service Providers of the National Health Agency). The QUALISS consists of establishing relevant qualification attributes to improve the quality of care offered by health service providers. It is available at http://www.ans.gov.br/prestadores/qualiss-programa-de-qualificacao-dos-prestadores-de-servicos-de-saude.
This study makes important contributions to the business practices of health service providers. The first contribution of this work is to examine an issue that has not been evaluated in the literature, highlighting the possibility of applying the artifact to any health insurance company in Brazil and other countries to generate better practical results. The second contribution is a proposal for health service providers, by providing information identifying shortfalls and possibilities for improvement for every aspect analyzed in the evaluation process. Therefore, this study shows the possibility of reducing expenditure on technical professionals to evaluate to what extent service providers meet requirements, promoting strategic alliances between self-managed companies and health service providers to serve the organization as a whole and enable a good cost-benefit relationship. Finally, the third contribution is that the article is the first to use DSR to prove that the quality assessment artifact for health services can play an important role in creating a competitive advantage for the organization. Consequently, it should be incorporated into business plans. DSR is a rigorous process for projecting artifacts to solve problems and assess what has been projected or what works and report the results. The results of this study provide an empirical basis for new resources of the artifact to be tested on the health services sector to obtain better performance and practical applicability for the sector. Any provider certified by the UNIPLUS Program can use it as a Quality Assurance Seal, allowing buyers (Health plan operators and beneficiaries) to have the power to choose the best service. As a strategy for maintaining UNIPLUS certification, it is necessary for the health service provider to submit annually the results of the indicators required for their category. Failure to comply with this requirement will result in the loss of certification.
The systematic monitoring of the application of the artifact in health service providers must be carried out, ensuring that it remains in line with current legislation, as well as in identifying corrective needs and improvement opportunities. The applicability to any operator has the observation of the norms and legislation in force in each country as the fundamental requirement.
Research Limitations
A limitation of this study from a theoretical viewpoint is its contemporary nature, and the approach requires a more careful and detailed analysis in relation to the development of further studies in the field of health in terms of DSR. The lack of comparison with other certifying organizations impedes the identification of advantages and disadvantages of the UNIPLUS Program artifact in relation to the other quality assessment methods of health services. Future comparative studies with other certification organizations are recommended to provide evidence of advantages and shortfalls in the use of the proposed Program. Moreover, it is necessary to update the technique of the UNIPLUS Program periodically, ensuring it remains adapted to the reality of the Brazilian health services and current legislation.
Suggestions for Future Research
In the literature, no records were found of previous research with a method to evaluate the quality and performance of health care service providers 5 that generate daily rates and fees, using the approach developed from the perspective of DSR. As this research question has yet to be fully answered and there is no proof of the existence of functioning artifacts, studies are required to prove the applicability or possible developments that enable new critiques, comparisons, and contributions that are of interest at the national and international levels. This is the first article to analyze the UNIPLUS Program artifact as a program for assessing the quality and performance of health service providers based on DSR.
Footnotes
Acknowledgements
The authors would like to thank the anonymous reviewers for their helpful suggestions and comments during the research for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.