
Abstract
Family caregivers are an important component of the long-term services and supports (LTSS) system. However, caregiving may have negative consequences for caregiver physical and emotional health. Connecting caregivers to formal short-term home- and community-based services (HCBS), through information resources and referrals, might alleviate family caregiver burden and delay nursing home entry for the patient. The aim of this study was to evaluate the early impact of the Program of Comprehensive Assistance for Family Caregivers (PCAFC) (established by P.L. 111-163 for family caregivers of seriously injured post-9/11 Veterans) on Veteran use of LTSS. A two-cohort pre-post design with a nonequivalent comparison group (treated n = 15 650; comparison n = 8339) was used to (1) examine the association between caregiver enrollment in PCAFC and any VA-purchased or VA-provided LTSS use among Veterans and (2) describe program-related trends in HCBS and institutional LTSS use. The comparison group was an inverse-propensity-score weighted sample of Veterans whose caregivers applied for, but were not accepted into, the program. From baseline through 24 months post application, use of any LTSS ranged from 13.1% to 17.8% for Veterans whose caregivers were enrolled in PCAFC versus from 3.8% to 5.3% for Veterans in the comparison group. Participation in PCAFC was associated with a statistically significant increased use of any LTSS from 1 to 24 months post application (over time odds ratios ranged from 2.71 [95% confidence interval: 2.31-3.17] to 4.86 [3.93-6.02]). Support for family caregivers may enhance utilization of LTSS for Veterans with physical, emotional, and/or cognitive conditions.
Introduction
For individuals with chronic disabling physical, emotional, and/or cognitive conditions, long-term services and supports (LTSS) are critical to maintain day-to-day function and independence. Formal LTSS, that is, LTSS provided by a trained and paid provider or organization, comprises (1) services received in residential facilities, such as skilled nursing facilities, assisted living, medical foster homes, and community residential care, referred to as institutional LTSS, and (2) services received in the home, such as homemaker home health aide care, outpatient adult day health care, respite care, and skilled home health care, referred to as home- and community-based services (HCBS).
LTSS use is of great interest to policymakers given the high demand for and high cost of these services. In 2013, the US health care system (all payer sources) spent an estimated $338.8 billion on formal (paid) long-term care. 1 Government programs are the primary funding source for formal LTSS and account for >70% of dollars spent on LTSS.1,2 Of all public payers, Medicaid and Medicare contribute the largest proportion of funds (64.5%), but other public sources, such as the Department of Veterans Affairs (VA), provide 7% of total LTSS spending.1,2 In 2013, VA spent a total of $5.6 billion on LTSS 1 and will face a growing demand for LTSS from both aging Vietnam War era Veterans and the over 1 million younger Veterans of post-9/11 conflicts with disabilities.3,4
Despite immense government spending on formal LTSS, informal care, which is defined as an individual who may have formal clinical training, but is not employed professionally to attend to the daily needs of another person,5,6 is an even greater source of LTSS. For the remainder of this article, we use the term “family caregiver” to indicate a family member or friend who provides care to a Veteran to help with day-to-day function. Among older adults, receipt of informal care was shown to reduce the use of formal home health care,6-8 delay nursing home entry, 7 and lower Medicare expenditures for both home health and skilled nursing facility care. 9 However, while informal care reduces the publicly funded cost of LTSS, it can have negative consequences for the physical, emotional, and financial well-being of the family caregivers. One review that focused primarily on caregivers of adults with dementia or illnesses, such as cancer, found that caregivers who spend more hours providing care are, on average, of lower socioeconomic status, experience more financial stress, feel that they had no choice in becoming a caregiver, and are, generally, at higher risk for experiencing higher levels of caregiver burden. 10 Younger individuals who are disabled may require a family caregiver for decades; long-term caregiving has heightened implications for caregiver burden and other negative outcomes, including poor quality care for the care recipient and financial distress. 4 Therefore, support for family caregivers including education, health system information, financial support, and health care services could be critical to ensure that younger individuals with disabilities receive high-quality care over time in the home. Yet, over the past 15 to 20 years, national and state-level efforts to support family caregivers have been inconsistent, poorly funded, and limited to modest tax credits offered by a few states, poorly funded National Family Caregiver Support Program training and services provided through Area Agencies on Aging,11,12 and cash and counseling demonstration projects to pay family caregivers instead of a formally trained provider to meet their care needs.13,14 Within VA, there are also national supports for caregivers, including a caregiver support line, peer support mentoring, and freely available programs to reduce caregiver burden. However, advocates argue that existing supports and services for family caregivers are not sufficient and highlight the need to expand these supports through paid leave policies, social security, expanded tax credits, and expanded Medicaid/Medicare waiver programs. 15 One example of such an expansion is P.L. 111-163, Caregivers and Veterans Omnibus Health Services Act, which in 2010 established the Program of Comprehensive Assistance for Family Caregivers (PCAFC), the first nationwide effort to systematically improve care for younger Veterans who are disabled by providing access to a broad range of services. Specifically, PCAFC supports eligible caregivers of post-9/11 Veterans who incurred or aggravated a serious injury (including traumatic brain injury [TBI], psychological trauma) in the line of duty and require ≥6 months of ongoing care because of an inability to perform one or more activities of daily living (ADLs) and/or need supervision or protection based on symptoms or residuals of neurological impairment or injury. These caregivers are provided with caregiver skills training; education about VA resources and services; respite care; mental health services; health care for those without coverage, travel, lodging, and per diem to attend required training or the Veteran’s medical appointments; and a monthly stipend ranging from $600 to $2300/month.
This program is unique because it provides a multitude of services and supports to family caregivers with the goal of improving Veteran outcomes; it therefore has the potential to increase the use of preferred, less expensive community-based services versus more expensive institutional services which has tremendous implications for patient-, family-, and system-level costs. Findings from a recent evaluation of this program suggest that Veterans whose caregivers are enrolled in PCAFC have higher use of VA-purchased and VA-provided outpatient services, including primary, mental health, and specialty care, and thus may be more engaged with VA services. 16 Furthermore, previous rigorous research has shown that older adults who have a family caregiver receive less HCBS and institutional LTSS compared with those without a family caregiver.7-9 However, it is unclear whether there is a difference in use of LTSS if caregivers receive training and other kinds of support, such as the support provided for caregivers enrolled in PCAFC.
The analytical objectives of this study are to describe program-related trends in use of any VA-purchased LTSS and to examine whether family caregiver participation in PCAFC was associated with changes in any VA-provided or VA-purchased LTSS use. We consider trends in use for HCBS and institutional LTSS as secondary outcomes.
Understanding the relationship between family caregiver support and Veteran LTSS use is critical to develop policies that effectively support caregiver needs while maintaining access to high-quality services for Veteran care recipients. Therefore, while this research has important implications for VA policy, future results from this work may eventually inform national and state-level policy agendas, as federal and state governments grapple with how to best assist millions of care recipients with disabilities who reside in their communities and are cared for by emotionally and financially burdened family caregivers.
Methods
Study Population and Design
The study sample comprised Veterans whose caregivers applied to PCAFC. Caregivers self-identified as needing support to provide ongoing personal care services to the Veteran because, due to neurological impairment and/or physical injury incurred or aggravated in the line of duty (eg, TBI, posttraumatic stress disorder [PTSD], amputation, etc), the Veteran was unable to perform one or more ADLs and/or needed supervision or protection. Within this sample, close to 90% of Veterans received VA disability compensation and approximately 70% of the sample received compensation for a high level of service-connected disability (defined as ≥70%). VA awards disability compensation to Veterans who are determined by VA to have a disability due to an injury or illness aggravated or incurred during active military service. A designation of 70% service-connected disability refers to the level of function that a Veteran has for a service-related condition. Common types of disabilities that result in a high rating for service-connected disability include physical (eg, musculoskeletal conditions, amputations, polytrauma) and cognitive disabilities (eg, TBI or PTSD).
A retrospective pre-post, nonequivalent comparison group design was used to evaluate the impact of the PCAFC on enrolled Veterans’ LTSS use. The treatment group comprised Veterans whose caregivers applied for and were ever approved to participate in the PCAFC from May 1, 2011, to March 31, 2014. For Veterans in the treatment group, caregivers had to be enrolled in the program for ≥90 consecutive days. Information about the program and how to apply is publicly available through a VA Caregiver interactive website, a toll-free Caregiver Support Line, and through community-based resources, including Veterans Service Organizations and other nongovernmental organizations. Caregiver Support Coordinators are located at every VA medical center, and they provide education and outreach to VA providers and the general public. The nonequivalent comparison group consisted of all Veterans whose caregivers had applied to the PCAFC during the same timeframe, but were determined to be ineligible. Caregivers were denied for several reasons that were both administrative (eg, not having served during the post-9/11 era [12%]) and clinical (eg, caring for a Veteran with an illness not related to military service [5%]). In all, caregivers were more often denied entry on the basis of administrative (n = 4656/8339) as opposed to Veteran-related clinical (3683/8339) reasons. It is possible that reasons for denial from PCAFC would make the treatment and comparison groups less equivalent; however, these applicants would have been excluded from our study if they did not meet the study eligibility criteria described below. Veterans were excluded from this study if they (1) had an identification number that could not be matched to VA data (Figure 1); (2) were ≥66 years as of September 11, 2001; (3) were >68 years as of the application date; (4) died within 90 days of the application date; (5) had a non-US or non–Puerto Rico home zip code at time of application; or (6) had a missing comorbidity score. The analytic cohort included 23 989 Veterans (treatment n = 15 650; comparison n = 8339).

Study flow diagram.
Baseline was defined as the application date for each dyad and established the pre-post timeframe in the analytic models. For the treatment group, baseline was the date of submission of the first approved application to the PCAFC; comparison group baseline was defined as the date of the first submitted application.
Data
This study analyzed VA program data and electronic health records that included the use of VA-provided and VA-purchased care from May 1, 2010 to September 30, 2014. Datasets were constructed by the VA Caregiver Support Program Partnered Evaluation Center which examined the impact of the PCAFC on VA and VA-purchased Veteran health care utilization. 16
Outcomes
Any LTSS use, the primary health service outcome of interest, was defined as use of any VA-provided or VA-purchased HCBS or institutional care within a given 6-month interval.
A secondary outcome of interest, HCBS, was defined as receipt of homemaker home health aide services (unskilled home health care), skilled home health care, adult day health care, hospice, or respite care services. While some hospice care and respite care may have taken place in an institutional setting, for the purposes of this report, this care is classified as HCBS. If a Veteran received any of the above types of care during the 6-month interval, the observation was coded as 1 (receipt of HCBS) versus 0 (no receipt of HCBS). Home-based primary care was not included as part of HCBS because eligibility and ongoing in-home assessments required as part of the PCAFC often used these service codes. As such, these types of services were considered to be directly related to routine program administration.
Institutional LTSS, another secondary outcome of interest, was defined as receipt of any care in a VA skilled nursing facility (community living center), a community nursing home, State Veterans Home, or medical foster care home. 17 Medical foster care homes provide services similar to those offered in assisted living facilities but in a smaller home-like setting. If a Veteran received any of the above types of care during a 6-month interval, the observation was coded as 1 (receipt of institutional LTSS) versus 0 (no receipt of institutional LTSS); if a stay crossed 2- or more 6-month intervals, the observation was coded as 1 for each time period to reflect receipt of any institutional care in each interval.
Explanatory Variables
Baseline variables were used in a propensity score model to control for factors that may have impacted both acceptance into PCAFC and Veteran propensity to use LTSS (Table 1). These variables were defined a priori and correspond to constructs defined by the Anderson-Newman model of health service use. 18 Per the Anderson-Newman model, explanatory variables used in the propensity score model included demographic information (predisposing characteristics) such as age, gender, race, ethnicity, and marital status. 18 Attributes affecting access to care and tendency to seek care (enabling resources and need) were service connection, means test status, enrollment priority group, distance to nearest VA Medical Center, homelessness, and non-VA health insurance. Individual comorbidities, prior health service use, and a comorbidity score were also included to conceptualize need. The Nosos score, akin to a Diagnostic Cost Group score,19-21 is a risk adjustment measure of expected use that is based on past diagnoses, inpatient care, outpatient care, pharmacy utilization, and demographics. 22
Baseline Descriptive Characteristics of Unweighted and Weighted VA Caregiver Support Program Treatment Group and Control Group Veterans (%).

Note. Percentages in table may not add to 100% due to rounding. This table is also presented in Van Houtven et al 16 ; VISN characteristics and complexity of the medical facility (1a, 1b, 1c, 2, 3) also assessed (not shown). 23 VA = Veterans Affairs; Control group = Veterans of caregivers who applied to but were denied entry into PCAFC; Treatment group = Veterans of caregivers approved into PCAFC; PCAFC = Program of Comprehensive Assistance for Family Caregivers; VAMC = Veterans Affairs Medical Center, VISN = Veterans Integrated Service Network.
Overall cohort: n = 8339 and n = 15 650 Veterans in the control and treatment groups, respectively.
The standardized difference for continuous variables is calculated as
Assessed in the year prior to and including application date.
Number of visits in the 6 months prior to and including application date.
Closest VAMC or Independent Outpatient Clinic at time of application, based upon distance from Veteran’s zip code.
Statistical Analysis
Propensity score model and inverse probability of treatment weights
As the PCAFC was implemented by law, we were unable to conduct a randomized controlled trial (RCT). Additional limitations, including rolling application dates, prevented us from using other quasi-experimental study designs (eg, discontinuity in calendar time) that might have accounted for all, including unobserved, differences between the treatment and comparison groups. Therefore, propensity score methods were determined to be the best available method to answer the stated research questions. To address observed differences, which can be seen in the large standardized differences between the treatment and comparison groups in the unweighted columns (Table 1), inverse probability of treatment (IPT) weights derived from propensity score models were constructed. While propensity score methods can account for observed between-group differences (see weighted columns in Table 1), they are unable to account for differences that are unobserved and therefore the primary assumption is that there are no unobserved differences in confounding variables between the treatment and comparison groups. To enhance observed comparability across the two groups, individuals in the comparison group were assigned weights based on how representative their individual characteristics were of individuals in the treatment group. Individuals in the treatment group were assigned a weight of 1 as the outcome of interest was the average effect of program participation on use of any LTSS among those in the program—in other words, the average treatment effect among the treated (ATT). 24
To assess whether balance was achieved on observed baseline covariates after IPT weights were applied, the following were examined: (1) graphical depictions of the propensity score distribution by treatment group (to further improve balance, individuals whose propensity scores did not overlap with scores observed in the other group were removed from the analytical sample prior to statistical estimation of outcome models [n = 186 treatment group, n = 767 comparison group]) and (2) the standardized differences of each covariate between the treatment and comparison groups. Standardized differences are robust to sample size; a standardized difference ≤10 suggests a reasonable level of balance 25 (see Table 1).
LTSS use outcome models
Generalized linear models were fit using generalized estimating equations weighted by the IPT weights with a logit link, binomial variance structure, and empirical sandwich standard errors to estimate the effect of the PCAFC over time on the probability of any LTSS use. The same technique was used to model the effect of the PCAFC over time on the probability of HCBS and institutional LTSS use. In the outcome models, 6-month time intervals were defined as the units of observation for each individual. For each individual, two 6-month intervals of service use data prior to the application were included as the “prebaseline” period. Application dates differed among caregivers and ranged from May 2011 to March 2014; therefore, the number of postapplication intervals naturally varied by Veteran. The number of postapplication 6-month intervals ranged from 1 to 4; the latter representing 19 to 24 months after application date. Because of this, Veterans who applied closer to the inception of the program were assessed for more 6-month intervals (see Table 2).
Sample Size for Each Postapplication Time Period. a
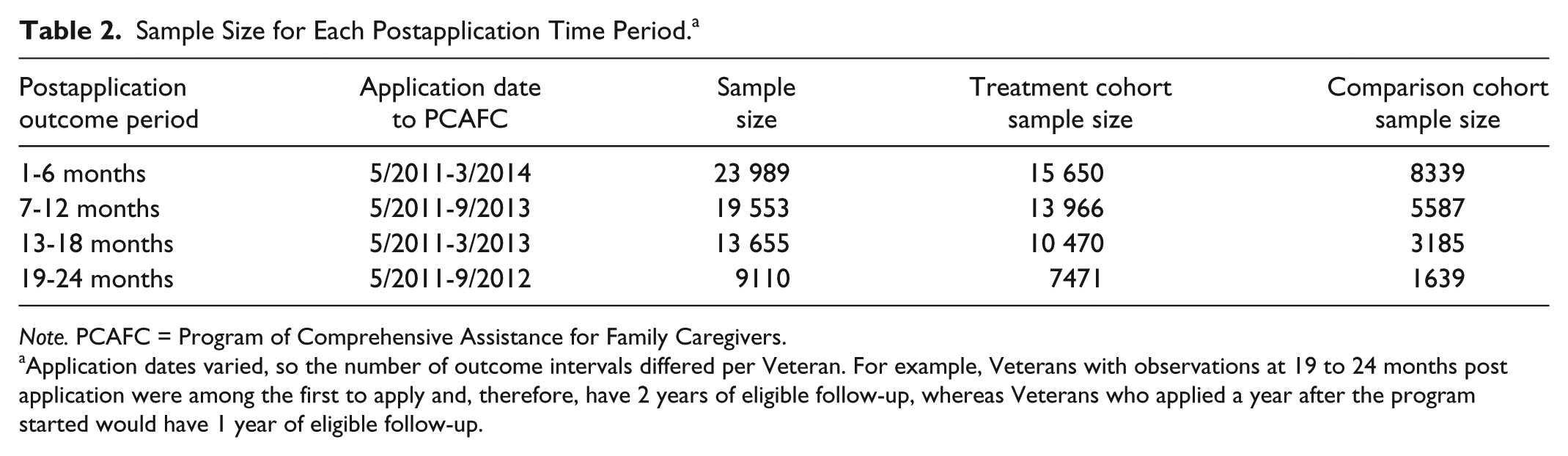
Note. PCAFC = Program of Comprehensive Assistance for Family Caregivers.
Application dates varied, so the number of outcome intervals differed per Veteran. For example, Veterans with observations at 19 to 24 months post application were among the first to apply and, therefore, have 2 years of eligible follow-up, whereas Veterans who applied a year after the program started would have 1 year of eligible follow-up.
The analytical model regressed any-LTSS service use on PCAFC participation and 6-month time intervals. To allow for nonlinear trends over time, each time interval was dummy coded and interactions between time and treatment status were included at all time points. The analyses were planned a priori and conducted in SAS 9.4 and SAS Enterprise Guide 7.1 (SAS Institute Inc, Cary, North Carolina). The cutoff for statistical significance was set at P < .05. This was a quality improvement project for VA operations, so the project was considered nonresearch and, therefore, not subject to institutional review board (IRB) approval.
Results
Sample Characteristics
Table 1 displays the characteristics of the unweighted and weighted samples classified by Veteran treatment or comparison group status. The columns labeled “Unweighted” present the preweighting baseline characteristics of treated (n = 15 650) and comparison (n = 8339) Veterans whose caregivers had applied to PCAFC, prior to incorporating propensity score weights. The large (>10) standardized differences observed in the unweighted cohort demonstrate that Veterans who were treated were notably different from Veterans who were not and indicate the need for IPT weighting to account for baseline differences. In the unweighted cohort, the treatment group Veterans had a lower proportion of women (7.6% vs 10.9%) and were on average 2.4 years younger than Veterans in the comparison group. A higher proportion of Veterans in the treatment group were of white race and Hispanic/Latino ethnicity, while a higher proportion of Veterans in the comparison group were of black race. Furthermore, a descriptively higher proportion of individuals in the treatment group (72.3%) was more than 70% service connected compared with the comparison group (64.0%) prior to applying IPT weights. After applying IPT weighting, all standardized differences were <10. The excellent balance indicates that the effects estimated in the multivariable analysis might approximate the unbiased ATT.
Trends in LTSS Use
The model-estimated prevalence of any LTSS use was much lower for individuals in the comparison group (Figure 2) following program application compared with those in PCAFC. In the first 6-month interval postapplication date, 13.1% (95% confidence interval [CI]: 12.5%-13.6%) and 5.3% (95% CI: 4.6%-6.1%) of treated and comparison Veterans, respectively, used any LTSS (combined institutional LTSS and HCBS). During this same interval, 9.5% (95% CI: 9.1%-10.0%) of treated Veterans and 2.2% (95% CI: 1.7%-2.8%) of comparison Veterans, respectively, used HCBS (Figure 3) and 4.4% (95% CI: 4.1%-4.7%) of treatment and 3.3% (95% CI: 2.8%-3.9%) of comparison Veterans used institutional LTSS (Figure 4). Examining model-estimated means, use of any LTSS was 7.8 percentage points higher for treated Veterans at 1 to 6 months, 13.5 percentage points higher at 7 to 12 months, 9.5 points higher at 13 to 18 months, and 7.7 percentage points higher at 19 to 24 months postapplication date compared with comparisons (Figure 2). Use of any HCBS followed a similar trend to use of any LTSS across the two groups (Figure 3). We found no clear patterns in the overall use of institutional LTSS which decreased overall, but not consistently through time, between application date and 24 months post application for both groups and ranged from 2% to 4.4% for both groups (Figure 4).

Model-estimated proportions and odds ratios (with 95% confidence limits) associated with having any VA-provided or VA-purchased LTSS.

Model-estimated proportions and odds ratios (with 95% confidence limits) associated with having any VA-provided or VA-purchased home- and community-based long-term services (HCBS) and supports.

Model-estimated proportions and odds ratios (with 95% confidence limits) associated with having any VA-provided or VA-purchased institutional LTSS.
Modeled Association Between Program Participation and Any LTSS Use
Results from the analytical model suggest that participation in PCAFC was associated with increased use of any LTSS from 1 to 24 months post application. Odds ratios ranged from 2.71 (95% CI: 2.31-3.17) at 1 to 6 months post application to 4.86 (95% CI: 3.93-6.02) at 7 to 12 months post application (Figure 2). While participants in the treatment group had a higher likelihood of using HCBS in 7 to 12 months prior to application date (odds ratio: 1.54 [95% CI: 1.08-2.18]) and no difference in 1 to 6 months prior to application date, their participation in PCAFC was associated with increased use of HCBS from 1 to 24 months post application (odds ratios ranged from 4.71 [95% CI: 3.66-6.07] at 1 to 6 months post application to 10.30 [95% CI: 7.61-13.94] at 7 to 12 months post application) (Figure 3). Participants in the treatment group had a lower likelihood of institutional LTSS use in the 12 months prior to application date (odds ratio at 7 to 12 months prior to application 0.66 [95% CI: 0.52-0.83] and odds ratio at 1 to 6 months prior to application 0.75 [95% CI: 0.62-0.91]); however, individuals in the treatment group used more institutional LTSS at 1 to 6 months (odds ratio 1.35 [95% CI: 1.11-1.65]) and 13 to 18 months (1.64 [95% CI: 1.10-2.44]) post application. There was no difference in institutional LTSS use between the two groups at any other time points (Figure 4), resulting in an inconclusive overall effect of PCAFC on trends of institutional LTSS use.
Discussion
Veterans whose family caregivers participated in PCAFC had significantly higher relative rates of any LTSS use between 1 and 24 months post application compared with Veterans whose caregivers were not enrolled. There are several plausible explanations for this. Due to education, training, and interaction with Caregiver Support Coordinators and other program staff, family caregivers enrolled in the PCAFC, compared with those not enrolled, may have become more knowledgeable about and received referrals to VA and community resources and services, such as respite care and adult day care. Also, these interactions may have encouraged caregivers to recognize their own need for time away from caregiving tasks and connected them with options for short-term HCBS for their Veteran.
Rates of HCBS use were consistently higher among PCAFC participants over time in the postapplication period. Institutional LTSS use was higher in some post application time periods, but these effects were inconsistent. This finding might suggest that those enrolled in PCAFC may be more likely to consistently use HCBS instead of institutional LTSS to meet the additional care needs of the Veteran that the caregiver cannot meet on his or her own. Relatedly, caregivers may choose HCBS to supplement the care they provide to remain eligible for PCAFC benefits. This is because permanent entry into institutional care would render the caregiver ineligible to participate in PCAFC as institutional care providers would assume the main caregiving responsibility for the Veteran. Given the young age of Veterans whose caregivers are enrolled in the PCAFC, from the patient and family perspectives, institutional LTSS might also be a less appealing source of care.
While more research is needed to understand the interplay between HCBS and institutional LTSS, if participation in PCAFC increases the use of HCBS and not institutional LTSS, this finding would have important implications for the VA. From a payer and health system perspective, use of HCBS is more desirable than institutional LTSS because it provides care in the least restrictive setting possible, the Veteran’s home or community, and may cost less. 26 Increased use of short-term HCBS may be an important strategy to improve caregiver well-being as limited research suggests that caregivers who use some type of LTSS may have fewer psychological symptoms and reduced caregiver burden.27-29 Furthermore, increasing the use of HCBS aligns well with VA’s commitment to provide patient-centered care because this is consistent with patient preferences to remain in the home 30 and engaged with their families and communities. 31 In turn, remaining in the community may facilitate long-term recovery for Veterans with physical, emotional, or cognitive conditions and disabilities resulting from their post-9/11 service. This perspective is also consistent with the Millennium Act that extended the home care benefit to qualifying Veterans in VA and stipulated rebalancing of long-term care services from the institutional setting to the home.32,23 Despite VA policy to extend home care services, such as respite, for Veterans who qualify clinically, not all eligible Veterans have access to or use this benefit.33,34 Yet, our findings suggest that providing education, knowledge, and resources to family caregivers may help to connect eligible VA users to LTSS. Mechanisms to connect Veterans to high-quality, lower cost HCBS care may be particularly salient for the cohort of post-9/11 Veterans whose caregivers are enrolled in PCAFC—the Veterans are young (mean age: 36 years) and may continue to need LTSS in the coming decades. 35
While additional research is needed, the results from this analysis may have broader implications for LTSS funded by both other public programs and consumers. There is an increasing need for LTSS in younger populations. Research suggests that obesity and its resulting sequelae, advances in medical technology (which allow individuals with significant health concerns to live longer), and the rising prevalence of disability among young people in the general population will drive up demand for LTSS. 36 Unfortunately, many in the civilian population face a more fragmented, difficult to navigate LTSS system than Veterans using VA LTSS. While the civilian and Veteran populations in need of LTSS differ, if trends similar to those observed in this analysis are also observed in the civilian population, supportive services for family caregivers through public and private insurers might improve access to formal HCBS LTSS which could, in turn, have positive implications for caregiver and patient outcomes.10,27,28
Several limitations to this study must be considered. First, it is possible that the statistical approach of IPT weighting did not address all residual unobserved confounding, including unobserved confounding related to PCAFC eligibility criteria. Statistically significant baseline differences were observed in LTSS service use between the treatment and comparison groups. However, a sufficient balance on observed variables was achieved which suggests that residual unobserved confounding might have been minimized through IPT weighting. 37 Second, as longer term follow-up was only available for those who applied close to PCAFC inception, effects after 24 months were not examined. Third, administrative data used by this study did not contain information about patient ADLs, instrumental activities of daily living (IADLs), or cognitive function. Fourth, we only consider use of LTSS provided or purchased by the VA health care system; these rates could differ across treatment and comparison group Veterans if we expanded our frame to other payers (eg, Medicaid, private pay services). Future research that takes a broader societal perspective, rather than the VA perspective, could inform the full picture of program impacts on LTSS.
Finally, these analyses do not capture information about Veteran preferences for HCBS versus institutional LTSS or how LTSS service use impacts critical caregiver outcomes. However, this analysis is part of a larger evaluation of the PCAFC and findings from other aspects of the evaluation might improve the understanding of Veteran and Veteran caregiver preferences for specific LTSS services. Despite these limitations, these analyses attempt to address an important gap in knowledge about a high-needs Veteran population with substantial rates of disability compensation through the use of a strong pre-post, two-cohort group design, and applied propensity score weights to limit observed baseline heterogeneity between groups.
Conclusions
These analyses are some of the first to examine the impact of comprehensive support for caregivers on any LTSS use and specific types of LTSS use (HCBS and institutional LTSS) among a cohort of young Veterans who were seriously injured in the line of duty. VA recognizes that family caregivers are already in place and committed to caring for their loved ones in their home environment. By engaging family caregivers in the VA system, caregivers can aid Veterans to access high-quality services that improve the quality of life for both the Veteran and caregiver. More research is needed to understand (1) the longer term impact of support for family caregivers on Veteran LTSS use and costs, (2) Veteran preferences for informal versus formal care and HCBS versus institutional LTSS, and (3) the impact of supports for family caregivers on civilian populations that likely face a different set of health concerns and system supports. Furthermore, additional work is needed to assess how reliance on HCBS versus institutional LTSS impacts family caregivers. If these services reduce caregiver emotional and financial burden, they may provide an important societal benefit. However, if the opposite is true, LTSS may require restructuring to better support family caregiver needs.
Footnotes
Acknowledgements
The authors gratefully acknowledge Ted Berkowitz for graphical design and the contributions of Drs. Eugene Oddone, Matthew Maciejewski, and John McCarthy. The contents of this report are solely the responsibility of the authors and do not necessarily represent the official views of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: While, the authors declare no conflicts of interest, as stated in the cover letter and “Acknowledgements” section, this research was funded by the VA Caregiver Support Program as part of a broader evaluation of the program on caregiver and Veteran health and health service use outcomes. The funding partners are coauthors (Margaret Kabat, Jennifer Henius, and Margaret Campbell-Kotler) and have reviewed and approved this paper. However, the funders were not involved in the analysis and interpretation of the data. As authors, the funders provided information about the structure of the program to inform the evaluation design, they reviewed drafts of the paper, and have given their approval for it to be published.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Veterans Affairs; Caregiver Support Program; Quality Enhancement Research Initiative (PEC 14-272); the Durham VA Center for Health Services Research in Primary Care; Geriatrics Research, Education, and Clinical Center; and the VA Quality Enhancement Research Initiative (QUERI) (grant IP1 HX002258-01). Megan Shepherd-Banigan is funded through the VA OAA HSR&D PhD Fellowship TPP 21-000.