
Abstract
The objectives of this study were to assess the factors which contribute to individuals’ health motivation to address hearing loss and to gather baseline data that could then be used to measure the impact of an awareness campaign. An online questionnaire with 13 closed set questions was completed by 100 subjects in each country including Austria, Germany, France, Sweden, and the United Kingdom. The questionnaire was based around the Health Belief Model, which describes how, in order to take action to address a medical problem, the individual must perceive that the condition presents a threat to their well-being that exceeds any barriers to treatment. Good hearing was regarded as being important in all countries. There was agreement that the main sign of hearing loss was turning up the TV or radio. In most countries, hearing aids were thought to be not particularly visible, not require much maintenance, a hindrance while doing sport, and must be removed before bed. Perceptions of hearing implants were that they were permanently fitted, not externally visible, and do not need to be removed before bed. Medical issues were mostly researched through a doctor and then via the Internet. In this sample, there was a good understanding of the consequences and signs of hearing loss, but although hearing implants were viewed as being different to hearing aids, there was little understanding that the external speech processor was similar to a hearing aid in its physical characteristics. When actions were taken, the key professionals consulted about hearing problems were the general practitioner and ear, nose, and throat specialist.
Keywords
Introduction
In the developed world, cochlear implantation has become a standard treatment option for adults and children with bilateral severe to profound hearing loss when powerful hearing aids no longer provide sufficient benefit. Estimates for the prevalence of hearing loss in the United States indicate that 3.4% of the total hearing impaired population have a severe or profound hearing loss (>70 dB HL). In the United Kingdom, this percentage was estimated as higher, with 6.7% of the clinical population having a bilateral pure tone average hearing loss greater than 70 dB HL.1,2 Taking population figures from 2013 and applying these prevalence figures, based on hearing loss, gives an estimate of 2 million children and adults who could potentially benefit from implantation in the these countries 3 alone. However, as of December 2012, only approximately 324,200 people worldwide had received a cochlear implant (CI). 4 A proportion of this discrepancy may be due to differences between the definition of severe to profound hearing loss in the prevalence studies and the specific CI criteria applied by the clinics, but this still represents a fraction of those who could benefit from this technology. This has led researches to look more closely at the penetration rates for this treatment.
Utilization rates for CI, in both adults and children with severe to profound loss, were reported in Sorkin and Buchman 5 for Germany, Austria, Sweden, United Kingdom, Australia, and the United States. These were based on the known implanted population and prevalence data collected in the respective countries. Pediatric utilization rates ranged from 97% in Australia to 50% in the United States and were considerably higher than adult utilization in all regions. Adult penetration was less than 10%, regardless of geographic region. This is surprising given that utilization rates for adult hearing aid use in people with a severe or profound hearing loss are high, at 70% to 90% and leads us to question why the uptake of CI in the adult population is so poor. 6
Lack of funding has the potential to restrict the number of suitable adults who are implanted. However, CIs have been shown to be highly cost-effective, with low complication rates, and in most developed economies, funding is provided by national health programs, employer-based insurance, or private insurance schemes.7,8 A contributing factor to the low numbers of adults receiving implants is the low numbers of suitable candidates presenting for assessment. We know that some adults decide against being referred for or having a CI, even after being assessed as a suitable candidate, due to concerns around surgery, worries about losing residual hearing, rehabilitation requirements, and the hope that another technology will come onto the market. Poor referral rates may also be due to poor awareness and knowledge of the treatment among professionals and patients, or even a negative perception of implants in the general population, due to the political issues around the impact implantation has on deaf culture and the deaf community. 6 Adults over the age of 65 years have a greater prevalence of hearing loss but an even lower utilization rate for CI than younger adults with acquired loss 9 ; for example, in Australia utilization in this group is 0.3%. 5 The perception of hearing loss as a natural consequence of the aging process, by both patient and professional, acts as an additional barrier to treatment for this group, and people who regarded hearing loss as being inconsequential and accept it passively are less likely to seek treatment. 10
Theories of learning use models to explain and modify behavior patterns. The Health Belief model provides a framework to describe how people can be influenced to change their health-related behavior. 11 The model states that 3 conditions are required to change behavior: (1) the existence of sufficient motivation (or health concern) to make health issues salient or relevant; (2) the belief that one is susceptible or vulnerable to a serious health problem or to the sequelae of that illness or condition (often termed “perceived threat”); and (3) the belief that following a particular health recommendation, at a subjectively acceptable cost, would be beneficial to reducing the perceived threat. Cost refers to the perceived barriers that must be overcome to follow the health recommendation; it includes, but is not restricted to, financial outlays. When this is translated into the area of hearing loss, we can state that people will take action to seek treatment for hearing loss if they view hearing loss as a serious problem, they feel sufficiently concerned about the severity of their hearing loss, and that there are more benefits than barriers to amplification. 12
One way of improving the awareness of hearing loss in the general population, its impact and the treatments available, is to put in place an education campaign. The purpose of any campaign would be to improve individuals’ motivation to take action and seek treatment. The aim of this study was to assess the factors that contribute to individuals’ health motivation to take action and address their hearing loss. The older adult population was targeted as the prevalence of hearing loss is higher in this group. The objective was to gather baseline data, in a range of countries, which would then be used to measure the impact of any future interventions put in place to improve awareness.
Method
An online questionnaire, designed by the authors, to assess subjects’ current health motivation to seek treatment for their hearing loss was provided by a professional market research company (Karmasin Motivforschung, Vienna, Austria). Subjects were asked to complete the online questionnaire at home. Data were collected from Austria, Germany, France, Sweden, and the United Kingdom.
The questions were based around the Health Belief model, as shown in Figure 1 and looked at subject’s perceived susceptibility to hearing loss, its severity (the perceived threat that hearing loss presents), and the barriers to action. Fifteen closed set questions were presented to assess subject’s perceptions in 3 areas: (1) their susceptibility to hearing loss, its importance to them and its impact (the threat); (2) the barriers that may prevent them from seeking treatment; (3) the actions that subjects currently take to address any hearing concerns.

Flow diagram describing the health belief model, showing the factors which encourage individuals to take action to address hearing loss.
Potential barriers to treatment were selected based on the personal experience of the authors, gained from focus groups and talking to existing CI users and CI clinicians. These were identified as being the visibility of the device or cosmetics, convenience of use for all situations, including sports or going to bed, and management of the device. Questions were designed to assess the perception of both implants and hearing aids, as a hearing aid is the alternative treatment option. Respondents were also asked if they thought there was any difference between a hearing aid and a hearing implant and in hearing sensitivity between hearing aids and implants. This was to assess if lack of perceived benefit or differences between implants compared with hearing aids was acting as a barrier to implantation.
The questionnaire was translated from English into the required languages both forward and backward, to check for any translation errors. A pilot study was conducted to ensure the clarity of the questions, with a group of normally hearing subjects; any questions which were felt to be unclear or ambiguous were reworded or deleted. The full questionnaire is provided in the appendix. The questions are grouped according to their relevance to the Heath Belief model.
Subjects
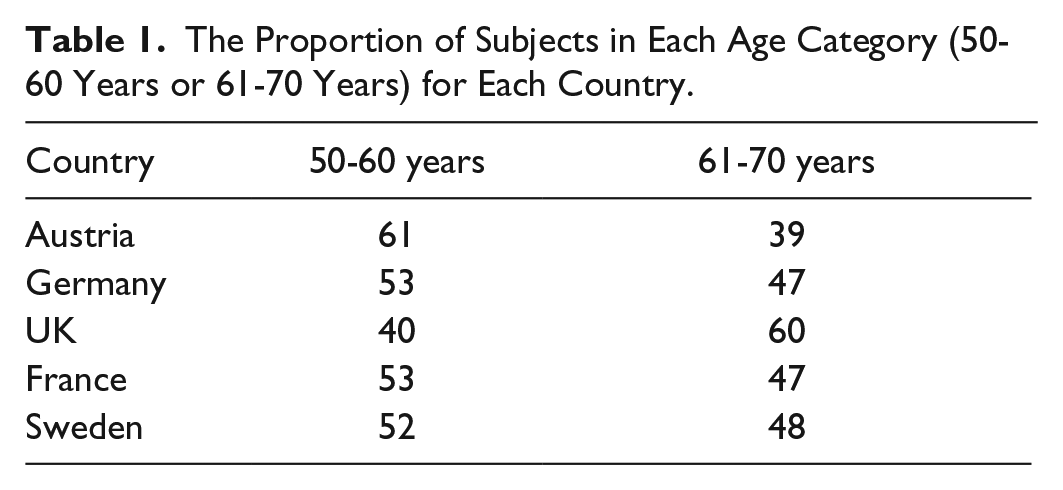
Subjects were recruited from a sample of individuals who were held on the database belonging to the Karmasin Motivforschung market research company and received no reward for taking part. The subjects held on the database had given their informed consent to the company for their data to be used anonymously in studies and publications relating to any questionnaires completed. A subset of individuals were selected from the database to participate in this study to provide a broad sample, representative of the general population of adults in each country. Factors taken into consideration were age and geographic region. Subjects were recruited in 2 age brackets: 50-60 years and 61-70 years. The proportions of subjects in each group, by country, are given in Table 1. There was an equal split between men and women. Subjects were recruited during a period from June 1, 2013, to July 31, 2013, and recruitment continued in each country until 100 fully completed questionnaires were collected. Incomplete questionnaires were discarded. The exclusion criteria were having no access to the Internet and not being able to complete the questionnaire online.
The Proportion of Subjects in Each Age Category (50-60 Years or 61-70 Years) for Each Country.
No ethics approval was required for the study, which was conducted according to the principles laid out in the Declaration of Helsinki.
Statistics
As the purpose of the study was provide baseline data, only descriptive statistics are provided for the percentage of respondents selecting each option for the closet set questions. Where a Likert rating scale has been used, mean values and ranges are given, but statistical comparisons are not made between values.
Results
The first 100 fully completed questionnaires for each country were included.
Perceived Susceptibility to Hearing Loss and Its Impact or Threat Perception
These questions sought to establish how relevant information about hearing implants and hearing loss was to the subjects, as well as the impact of hearing loss.
Question 3
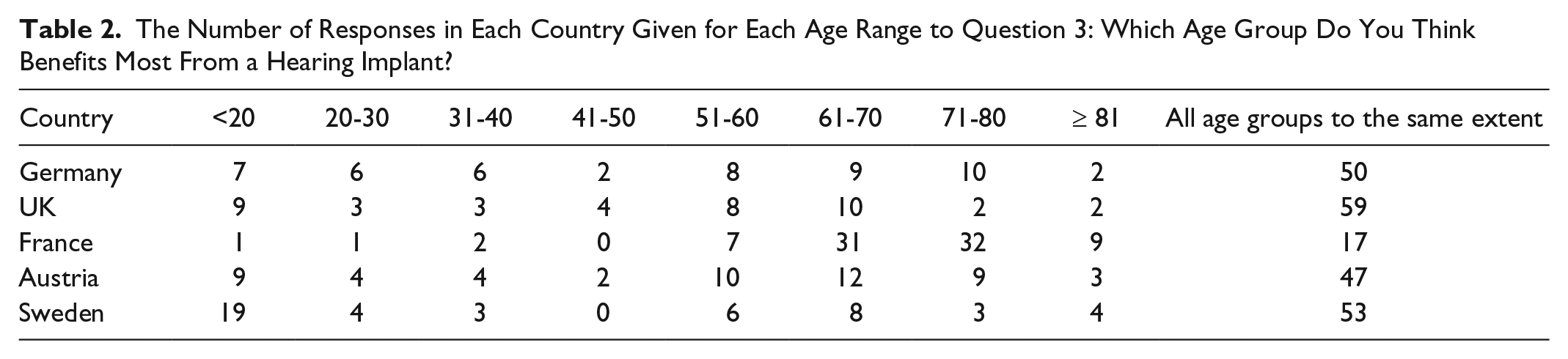
In 4 out of 5 countries, over 40% of respondents thought that hearing implants benefited all age groups equally (Table 2).
The Number of Responses in Each Country Given for Each Age Range to Question 3: Which Age Group Do You Think Benefits Most From a Hearing Implant?
Question 4
Hearing loss was most commonly viewed as the reduction in the ability to hear in all countries. Percentages of respondents ticking this box ranged from 80% in the United Kingdom to 43% in Sweden. In Germany and Austria, only 60% and 63% of people selected this box, but 28% and 37% of people, respectively, also selected “hearing loss is the complete loss of the ability to hear.” Between 33% and 18% of people thought hearing loss could be halted (Table 3).
The Number of Responses in Each Country Given for Each Answer to Question 4: Which of the Following Statements About Hearing Loss Are Correct in Your Opinion?

Question 5
The majority of subjects (range, 85%-59%) viewed the terms hearing loss and hearing impairment as being different from each other. The next most common answer was “don’t know” and over 80% of respondents ticked either one or other of these boxes.
Question 10
All countries listed having the volume of TVs and radios turned up very high as the main sign of possible hearing loss. Percentages ranged from 80% of subjects selecting this option in the United Kingdom to 51% in Sweden. The top 4 other indicators in all regions were difficulties hearing high-pitched sounds, problems and difficulties in using a telephone, an inability to locate background sounds, and constant ringing or buzzing in the ears. A much lower percentage of people selected problems using the telephone in Sweden and France than in other countries (30% and 29% vs 50%-62%).
Question 12
The top 4 consequences of hearing loss were restricted communication (when face-to-face and when using the telephone), impaired quality of life, social isolation, and frustration. Four countries listed restricted communication as the top consequence, with percentages ranging from 95% to 73%.
Question 13
When asked “How important is it for you personally to have a good sense of hearing, to be able to hear well?” the mean rating and mode on a Likert scale was 1 for all countries, where 1 represents “completely agree” and 5 “do not agree at all” (Table 4).
The Mean Likert Scale Ratings Given for Question 13: How Important Is It For You Personally to Have a Good Sense of Hearing, to Be Able to Hear Well?
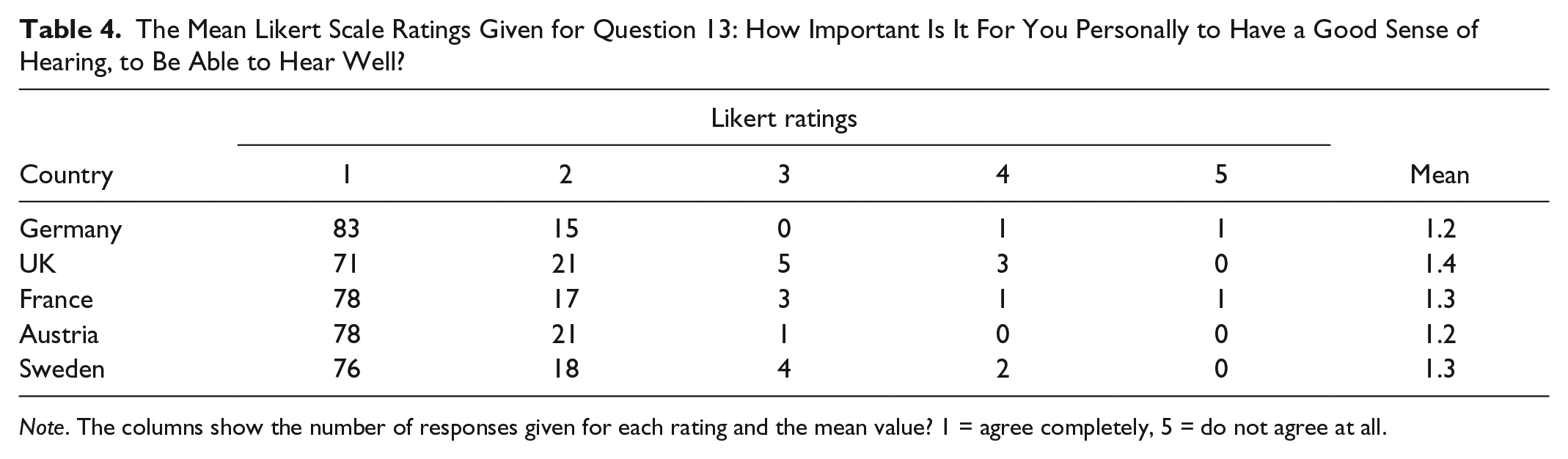
Note. The columns show the number of responses given for each rating and the mean value? 1 = agree completely, 5 = do not agree at all.
Actions Taken
Question 6
Across all countries, people primarily found out about medical issues from their doctor, followed by the Internet. Percentages ranged from 71% to 80% for the doctor and 56% to 77% for the Internet. Less than 10% of people did not inform themselves about medical issues at all.
Question 7
Again, the medical doctor and the Internet were the most common sources of information for finding out about hearing impairment. Percentages were generally lower than for general health issues, but similar across countries, and ranged from 50% to 65% for the doctor to 33% to51% for the Internet (France and the United Kingdom). In Germany, France and Austria a high percentage of respondents (26%, 31%, and 23%) did not inform themselves at all about hearing impairment.
Question 8
The general practitioner (GP) and dentist were the most common doctors to visit just as a precaution, and percentages were similar across countries, ranging from 68% to 54% for the dentist and 47% to 68% for the GP, with France being the lowest figure. A low percentage of people visited the ear, nose, and throat (ENT) specialist with percentages ranging from 9% to 10% in Sweden and the United Kingdom to 21% to 28% for Germany France and Austria.
Question 9
When those who had indicated in the previous question that they do not visit an ENT specialist as a precaution were asked why not, the reasons indicated were either never had problems in that area (37%-43%) or, for 4 countries, never thought to do so (32%-39%). The exception was France, where the second reason indicated was “I do not think it’s necessary” (34%) and “never thought of doing so” was the fifth reason given (15%).
Question 11
If suffering from a hearing loss over 96% of people living in Germany would visit an ENT specialist and 40% of them would visit a hearing aid acoustician. The figures are similar in Austria at 91% and 38%, respectively. France and Sweden would visit the ENT specialist (82% and 63%) followed by the GP (31% and 46%) and third a hearing aid acoustician (26% and 36%). The United Kingdom followed a very different pattern with the GP being the first medical specialist to consult (83%), an ENT specialist second (45%), and the hearing aid acoustician fourth at 20%.
Barriers to Treatment
Question 2
When asked if there was a difference between a hearing aid and a hearing implant, the majority answered “yes” (72% UK to 40% France) or “don’t know” (24% UK to 56% France).
The other barriers were addressed with 1 question where respondents were required to rate each statement (shown in Table 5) on a Likert scale from 1 to 5, where 1 represents “completely agree” and 5 “do not agree at all.” Ratings of 1 and 2 are grouped as “agree” and 4 and 5, “disagree.”
The Responses Given in Each Country to Question 1: To What Extent Do You Agree With the Following Statements About Hearing Aids/Hearing Implants?

Note. 1 = agree completely, 5 = do not agree at all. The mean rating is given, with the percent of time this answer was given a score of “1” or “2” indicated in parentheses.
The lowest Likert ratings and therefore highest agreement ratings for Sweden, Germany, Austria, and the United Kingdom were for “hearing implants are permanently fitted and do not need to be removed before bed,” “hearing implants are not externally visible,” and “hearing aids must be removed before bed at night.” Weaker agree ratings were given for “hearing implants require regular maintenance” and “hearing aids can be a hindrance when doing sport.”
The strongest disagree ratings for these 4 countries were given for “qualitatively there is no difference between hearing aids and hearing implants” and “hearing implants can be a nuisance during physical activity” followed by “hearing aids require a great deal of maintenance” and “it is usually possible to immediately identify people wearing hearing aids.”
France has a slightly different pattern of responses; strong agreement ratings are given for “hearing aids must be removed before bed” but also “hearing implants require regular maintenance and adjustments.” Agreement ratings are also given for “hearing implants can be a nuisance during physical activity.” A strong disagreement rating is given for “hearing implants are permanently fitted and do not need to be removed before bed” as well as “qualitatively there is no difference between hearing aids” and “it is usually possible to immediately identify people wearing hearing aids.”
Discussion
The results of the survey provide an insight into the current opinions on hearing loss of the older adult population. The Health Belief model was used as a framework to interpret the data, and the questions were divided into categories to address the 3 key areas. The model describes how, to take action to address a medical problem, the individual must perceive that the condition presents a sufficient threat to their well-being that exceeds any barriers. If utilization of CIs is to increase, awareness of the impact of hearing loss and the treatments available must be improved. To reduce the barriers to cochlear implantation as an effective treatment, knowledge of its benefits and limitations must also be improved and any misconceptions corrected. The data gathered in this survey enabled the authors to assess how individuals perceived their susceptibility to hearing loss, its impact on their lives, and some of the barriers which might be preventing them from seeking a CI as a treatment. It also showed what actions people were taking once they had decided to seek help and provided a baseline to measure the impact of a planned awareness campaign.
When looking at the perceived threat, as expected, good hearing was regarded as being important in all countries. However, the wording of this question lead respondents toward a positive response and a more open format might have produced different results. Hearing loss was viewed as either a reduction in the ability to hear or, to a lesser extent, the total loss of all hearing. This ambiguity in the definition of hearing loss was highlighted when subjects were asked if there was a difference in the terms hearing loss and hearing impairment; most answered either “yes” or “don’t know.” The World Health Organization uses the term hearing loss to cover all levels of hearing impairment and the terms are used interchangeably by many professionals across all the countries surveyed. On reflection, this question was confusing for many respondents, reflected in the high number of don’t knows and should have been removed after the pilot stage.
When asked which age groups would benefit most from a hearing implant, most respondents identified all groups equally. In Sweden, more respondents selected the under 20s compared with the other countries, but over 50% still selected “all groups equally.” However, in France the pattern was different. The older age groups were selected as being the most likely to benefit, with low percentages for the under 20s and “all groups equally.” It is not know why the data were so different in this country. The age categories were set to keep consistency across countries; however, if different age category boundaries were chosen or the age bands given names, then the results could have been different. Prevalence data have shown that hearing loss increases with age, but the provision of implants in the over 65s is lower than in younger people, despite there being no clinical barriers to older adults receiving a CI.5,9,13-15 It was encouraging that in general, respondents identified that older adults could benefit from an implant. However, the lack of access in this group to appropriate treatment is concerning, particularly as recent studies have highlighted the relationship between untreated hearing loss, general health, and dementia.16,17
There was agreement across all countries that the main sign of hearing loss was turning the TV or radio up high and the next 4 most frequent responses were also common to all countries (difficulties hearing high-pitched sounds, problems and difficulties using a telephone, an inability to locate background sounds, and constant ringing or buzzing in the ears). There was also a good understanding across all countries of the consequences of hearing loss, although the exact order of the responses varied slightly.
When addressing the barriers to treatment, the questions focused on the visibility of the device, the convenience of use for all situations, specifically sports or going to bed, and general management of the device. As not all barriers to treatment were explored, the conclusions relating to this area of the survey can only be drawn based on the questions asked. Barriers such as fear of surgery, losing residual hearing, and identity considerations were not considered as they were not identified by the focus groups as key areas of concern at the time. Since the study was conducted, there is more awareness among professionals of some of these barriers to implantation, and if the study were to be repeated, they should be included.
In general, subjects knew that there was a difference between hearing aids and hearing implants (72% to 40%) and when asked if there was no qualitative difference (in terms of hearing sensitivity) between them, median scores tended toward disagree, indicating that a difference is perceived. However, we do not know if the respondents understood what the differences were. For the questions about hearing aids, there was general agreement across countries that hearing aids are not seen as being particularly visible and can be a hindrance while doing sport and must be removed before bed. They were also thought not to require much maintenance, except in France where a slightly higher agreement rating was given for this statement. Perceptions of implants were the opposite. Four out of 5 countries thought implants do not have to be removed before bed, are not externally visible, need little maintenance, and are not a hindrance for physical activities. Only in France were implants correctly viewed as externally visible, needing to be removed before bed, a hindrance for physical activities, and requiring regular maintenance and adjustment. Interpretation of these results is complicated using the word “implant” when referring to a CI. The implanted part of the device cannot be removed and is not visible. However, to work the implanted device must be connected to an externally worn microphone and speech processor resembling a hearing aid, which can be removed. Although the respondents may not know what a cochlear implant is, an implant of any kind is not normally removed and only someone knowledgeable about CIs would know that the external speech processor can be removed. If some respondents in the sample were aware of this distinction, they might still have answered, correctly, that the implant cannot be removed. When initial discussions about hearing implants are taking place, the realization by patients that the external parts of a hearing implant are not very different practically from a hearing aid and retain the same perceived stigma may deter patients from even agreeing to be referred for an assessment.
Medical issues were mostly researched through a doctor and then via the Internet, including those relating to hearing. This would support the use of an Internet-based awareness campaign, although, because it was an Internet based survey, the sample selected was clearly already comfortable with Internet use. Internet use among older adults is known to decline over the age of 75 years; nevertheless, survey data have shown that around 70% of people in their early 70s go online. 18 In Germany, France, and Austria, a high percentage of respondents (26%, 31%, and 23%) did not inform themselves at all about hearing impairment.
The current precautionary health actions taken were most commonly visits to the GP. Not many subjects said they would visit an ENT specialist as a precautionary measure, with the reasons given as never having had problems in this area or never thought to do so.
When asked who they would visit if suffering from a hearing loss, patterns of behavior were dictated by country specific guidelines. In the United Kingdom, for example, the National Health Service Web site advises people to visit the GP as the first person to consult for hearing issues and it is mandatory to consult a GP before going to see an ENT specialist. 19 In Germany and Austria, over 90% of people would visit an ENT specialist and then a hearing aid acoustician. In France and Sweden, people would first visit the ENT specialist followed by the GP and third a hearing aid acoustician. In research looking at hearing aid uptake in the moderate to severely hearing impaired group, the GP’s management of age-related hearing impairment was found to be a barrier to seeking help for hearing impairment, and this would be a factor against initially consulting a GP. 12 In practice, those people within the audiometric criteria for implantation are likely to be fitted with a hearing aid and already under the care of an audiologist or hearing aid acoustician, who are often best placed to make an appropriate referral to a CI program. It was decided not to distinguish between audiologists and hearing aid acousticians in the survey. Hearing aid acousticians are present in all countries included in the study and are more numerous than audiologists. Training for audiology varies widely in level and availability in the different countries. There are hardly any audiology training programs in Austria and France and a few in Germany and Sweden; thus, access to audiologists in these regions is limited, and hearing aid acousticians are the most likely professionals to be consulted.
The authors have made every attempt to control for bias in the study results. However, bias may still be present in the study sample selected. The subjects who completed the questionnaire were clearly technically competent enough to fill out a questionnaire online and were sufficiently interested in the topic to take part in the survey. There was no information provided on whether subjects had an existing hearing loss or wore a hearing aid, and this may have had a large impact on the levels of knowledge of the sample. There was also no data gathered on the education levels or socioeconomic group of the participants. The questions asked were closed set and did not provide an opportunity for comment; this may be particularly relevant for the barriers to treatment suggested.
Future research will focus on the use of online, media based advertising campaigns designed to raise awareness. The use of the Internet as a source of medical information is becoming commonplace, and the results of this survey support this finding, even in the older age groups. The advertising will direct users via a click through, to a Web site providing comprehensive information on implantable hearing devices. From this point, the individual is free to access as much or as little information as they choose. The media outlets chosen will cover both mainstream media and publications aimed at health care professionals and related to hearing. There is currently more awareness within the CI community that more training need to be provided to hearing professionals and that hearing aids users need to be made aware that a CI may be a suitable treatment for them. This has resulted in some regional awareness activities and other media campaigns funded by implant manufacturers. The intention of this activity is to increase awareness of cochlear implantation, and thus, it will be difficult to establish the impact of this individual campaign on behavior. However, all of these activities are welcome and necessary as without action to improve awareness of this treatment, many individuals who could have benefited from a CI will not receive one.
Conclusions
In this sample of 50 to 70 years old, taken from multiple countries, hearing loss was perceived as a problem. There was a good understanding of the consequences and signs of hearing loss, but knowledge was limited. Cochlear implants were viewed as being different to hearing aids, but not always in the correct way, and there was little understanding that the external speech processor was similar to a hearing aid in its physical characteristics. Medical issues, including those relating to hearing, were mostly researched through a doctor and then via the Internet. It was encouraging that when motivated to do so, people sought information from medical professionals, mostly GPs and ENT specialists, about their hearing problems. The data collected in this first phase of the awareness campaign will be used as a baseline to measure changes in the data, using the same sample population and questionnaire, following an Internet awareness campaign aimed at referring ENT clinicians and older adults.
Footnotes
Appendix

| Perceived susceptibility to hearing loss and its impact (threat) |
|---|
| Question 3: Which age group do you think benefits most from a hearing implant? |
| Question 4: Which of the following statements about hearing loss are correct in your opinion? |
| Question 5: Is there a difference between hearing loss and hearing impairment? |
| Question 10: What are the signs of possible hearing loss? |
| Question 12: What are the consequences for people suffering from hearing loss? |
| Question 13: How important is it for you personally to have a good sense of hearing, to be able to hear well? |
| Perceived negatives of treatment options (Barriers) |
| Question 1: To what extent do you agree with the following statements about hearing aids/hearing implants? |
| Question 2: Do you think there is a difference between a hearing aid and a hearing implant? |
| Current actions taken to address health issues (Actions) |
| Question 6: How do you find out about medical issues/illnesses? |
| Question 7: How do you find out about the subject of hearing and the possible associated impairments? |
| Question 8: Which of the following doctors do you visit without an acute condition just as a precaution? |
| Question 9: Why do you not visit an ear, nose, and throat (ENT) specialist as a precaution? (for those who indicated in the previous question that they do not) |
| Question 11: Assuming that you suffer from hearing loss yourself. Which of the following medical facilities would you visit? |
Acknowledgements
The authors would like to thank Paula Greenham of Greenham Research Consulting Ltd, who was funded by MED-EL GmbH, Innsbruck, Austria, for her writing assistance in providing the first draft of the manuscript.
Authors’ Note
All authors contributed the planning, study design, interpretation of the data and/or review of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Patrick D’Haese is an employee of MED-EL GmbH, Innsbruck, Austria. Prof Van de Heyning receives grants to the institution from MED-EL and Cochlear.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MED_EL GmbH provided funding for the study.