
Abstract
A new breast cancer treatment, brachytherapy-based accelerated partial breast radiotherapy (RT), was adopted before long-term effectiveness evidence, potentially increasing morbidity and costs compared with whole breast RT. The aim of this study was to estimate complication rates and RT-specific and 1-year costs for a cohort of female Medicare beneficiaries diagnosed with breast cancer (N = 47 969). We analyzed 2005-2007 Medicare claims using multivariable logistic regression for complications and generalized linear models (log link, gamma distribution) for costs. Overall, 11% (n = 5296) underwent brachytherapy-based RT; 9.4% had complications. Odds of any complication were higher (odds ratio [OR]: 1.62; 95% confidence interval [CI]: 1.49-1.76) for brachytherapy versus whole breast RT, similarly to seroma (OR: 2.85; 95% CI: 1.97-4.13), wound complication/infection (OR: 1.72; 95% CI: 1.52-1.95), cellulitis (OR: 1.48; 95% CI: 1.27-1.73), and necrosis (OR: 2.07; 95% CI: 1.55-2.75). Mean RT-specific and 1-year total costs for whole breast RT were $6375, and $19 917, $4886, and $4803 lower than brachytherapy (P < .0001). Multivariable analyses indicated brachytherapy yielded 76% higher RT costs (risk ratio: 1.76; 95% CI: 1.74-1.78, P < .0001) compared with whole breast RT. Brachytherapy had higher complications and costs before long-term evidence proved its effectiveness. Policies should require treatment registries with reimbursement incentives to capture surveillance data for new technologies.
Keywords
Background
Use of new medical technology may inadvertently increase costs of care or morbidity while diffusing into practice without long-term effectiveness evidence.1,2 This case study of the introduction of a new radiotherapy (RT) modality explores the impact of early implementation. Instead of a standard treatment for early invasive breast cancer that includes lumpectomy with 4 to 7 weeks of whole breast RT,3,4 evidence suggested that a new RT paradigm requiring twice-daily treatment over 5 days could be effective by targeting only the tumor cavity and immediate surrounding area rather than the whole breast;5,6 this new RT was called accelerated partial breast RT. It utilizes more efficiently focused RT to the tumor bed, where most ipsilateral breast recurrences occur; it also reduces the time burden and inconvenience of whole breast RT by requiring fewer treatments over a shorter time period,3,4,7,8 and it may minimize acute side effects such as fibrosis, asymmetry, skin burns, and chronic side effects such as cardiac toxicity, pulmonary fibrosis, and rare secondary malignancies.9,10 However, published guidelines suggested that accelerated partial breast RT should be used on highly selected patients, those with smaller tumors, negative lymph nodes, and low probability of recurrence.11,12 Balloon brachytherapy–based accelerated partial breast RT for early breast cancer is an example of a technology with early uptake prior to published long-term effectiveness evidence.1,13 -16 The treatment requires the invasive surgical implantation of a balloon-like device into the tumor bed after lumpectomy, making the patient susceptible to infection. A high-dose seed of radiation is inserted through a catheter into the balloon-like device twice daily for 5 days. Early follow-up data indicated low local recurrence rates and good cosmetic outcomes,7,10,17 but longer follow-up data were not available when physicians started adopting the technology in the 2000s.7,17 -23
Prior to publication of results of randomized studies with long-term follow-up, we sought to estimate the costs and complications comparing whole breast RT with balloon brachytherapy–based accelerated partial breast RT in Medicare beneficiaries to evaluate whether there were changes in RT costs or morbidity for women with early breast cancer. Previous work estimating complication rates included all patients receiving balloon brachytherapy in large cohorts of Medicare beneficiaries,24,25 and used analytic methods to try to account for selection into treatment. We studied a more homogenous patient cohort with the least extensive invasive breast cancer, to estimate relevant complication rates in a more guideline-appropriate cohort.
Data and Methods
We analyzed physician, inpatient, and outpatient Medicare fee-for-service claims data from the 2004-2008 Chronic Condition Data Warehouse (CCW) for women aged 66 years and older with at least 1 inpatient or 2 outpatient International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes for breast cancer (174.X) 26 and who underwent breast-conserving surgery. We included women with continuous coverage by Medicare Parts A and B and who were not in a health maintenance organization (HMO) during the observation period to ensure we had full claims to assess treatment and preexisting comorbidities. To select patients who had earlier stage disease and would be more likely concordant with professional society selection criteria, we excluded those who had more extensive treatment, assuming they had more advanced breast cancer, because we did not have explicit stage information in claims data. Therefore, we excluded those who received mastectomy, chemotherapy, or an axillary lymph node dissection after a sentinel lymph node biopsy prior to RT. We categorized RT type using Current Procedural Terminology (CPT) codes similar to previous work, 1 using CPT/Healthcare Common Procedure Coding System (HCPCS) codes appropriate to distinguish between brachytherapy-based accelerated partial breast RT and whole breast RT within 16 weeks of surgery for whole breast RT and within 12 weeks following surgery for brachytherapy (Table 1). At the end of RT, the follow-up period began, and we identified complications including any complication (i.e., 1 or more), infection or wound complication, seroma, breast fibrosis, fat necrosis, cellulitis, breast pain, and additional hospitalization within 1 year of the end of RT. Patient age and race were taken from the Medicare eligibility file. We linked US Census tract data for information on rural residence and high poverty (>20%), and calculated the Klabunde comorbidity index 27 for each subject. Our final cohort had 47 969 beneficiaries undergoing RT after breast-conserving surgery from 2005 to 2007, allowing us to calculate preexisting comorbidity burden and have 1 year of follow-up that started at the end of radiation treatment. High poverty was not significant and was removed from our models. This study was approved by the lead author’s institutional review board.
ICD-9 Diagnosis and Procedure and HCPCS Codes Used to Identify Breast Cancer–Related Procedures and Complications.

Note. ICD-9 = International Classification of Diseases, Ninth Revision; HCPCS = Healthcare Common Procedure Coding System.
Complications Analysis
We conducted chi-square tests of differences in complication rates by RT modality. Next, to evaluate the odds of a patient having a complication associated with RT, we estimated a multivariable logistic model for the odds of any complication and for the odds of each complication type separately. We conducted Hosmer-Lemeshow goodness-of-fit tests for each model. This chi-square test was not significant in any models, indicating no evidence of poor fit. Out of concern for selection into treatment (i.e., endogeneity bias, or confounding by indication), we explored using a bivariate probit model analogous to instrumental variables analysis28 -30 and found our point estimates of complications were nearly identical to the nonsimple model results. For ease of interpretation, therefore, we present the logistic regression results.
Cost Analyses
We separately calculated mean RT-specific and 1-year total costs for combined inpatient, outpatient, and physician services, adjusting for inflation using the consumer price index, comparing mean costs by treatment type using a t test, because mean costs are easily interpreted and typically used as inputs for cost-effectiveness analyses. We also calculated mean cost confidence intervals (CIs). We then estimated multivariable generalized linear models with a log link and gamma distribution to explore factors associated with costs. In multivariable analyses, we accounted for whether a subject had 1 or more RT complications (e.g., infection or wound complication, seroma, fibrosis), race, rural residence, age, and comorbidity index. The coefficients are exponentiated and presented as rate ratios, indicating the relative expenditures with and without the covariate effect, or the percentage increase or decrease in costs associated with each covariate. Finally, we estimated the economic burden to Medicare for reimbursing brachytherapy-based accelerated partial breast RT instead of standard whole breast RT in advance of published long-term evidence. All costs are represented as 2008 US$. We conducted sensitivity analyses on all multivariable models to evaluate whether death during follow-up affecting <2% of patients had an impact on model results.
Results
Nearly 11% (n = 5296) of the cohort underwent brachytherapy-based accelerated RT (Table 2). The sample was mostly white (91%), aged 70 to 79 (54%), predominantly nonrural, mostly lived within 10 miles of a brachytherapy provider, and on average had few comorbidities. Of 47 969 women in the cohort, 4510 (9.4%) had at least 1 complication, with 13.6% of brachytherapy patients and 8.9% of whole breast RT patients having at least 1 complication (P < .0001 in unadjusted analysis; Table 2). Individual complications varied by brachytherapy receipt in univariate analyses, with infection/wound complication (n = 1894), seroma (n = 150), breast pain (n = 1558), cellulitis (n = 1298), and necrosis (n = 298) varying by RT type. Receipt of brachytherapy was statistically different by race, ruralness of residence, and distance to nearest brachytherapy provider (Table 2).
Cohort Characteristics for Female Medicare Beneficiaries with Breast Cancer Treated by Breast-Conserving Surgery and Radiotherapy(2005-2008, N = 47 969).

Multivariable analysis of complication rates showed that the odds of experiencing any complication in the year after RT were 1.62 times higher (95% CI: 1.49-1.76) for brachytherapy compared with whole breast RT (Table 3). Seroma was much rarer (0.3% of patients overall) though occurred 2.85 times more in brachytherapy patients (95% CI: 1.97-4.13) than in whole breast RT patients. Wound complication/infection, breast pain, cellulitis, and necrosis also had higher odds of occurrence following brachytherapy compared with whole breast RT. Odds of burn, hospitalization, and fibrosis were not statistically significantly different by RT modality. (Supplementary Table expands Table 3 to show all covariates.)
Odds of Complication Associated With Brachytherapy-Based Partial Breast Radiation Compared With Standard Whole Breast RT (Reference).

Note. Controlled for age, race, rural, treatment year, and comorbidity burden. RT = radiotherapy.
Mean radiation-specific costs were $6375 (95% CI: $6350-$6400) for whole breast RT, compared with $11 261 (95% CI: $11 137-$11 385) for brachytherapy-based RT, yielding a statistically significant difference of $4886 (P < .0001; Table 4). One-year total mean costs were $19 917 (95% CI: $19 763-$20 070) for whole breast RT, compared with $24 720 (95% CI: $24 317-$25 124) for brachytherapy-based RT, again a statistically significant difference of $4803 (P < .0001). In multivariable analyses, brachytherapy was associated with 76% higher RT costs (risk ratio: 1.76, 95% CI: 1.74-1.78, P < .0001) and 23% higher 1-year costs on average, compared with whole breast RT (risk ratio: 1.23, 95% CI: 1.20-1.25, P < .0001; Table 5). One-year costs were twice as high for women with the highest comorbidity burden (P < .0001). Sensitivity analysis results are qualitatively the same and show a lack of “death bias,” likely because so few died in the year (889 of 47 969; 1.85%).The incremental treatment-specific cost of early adoption of brachytherapy-based accelerated partial breast RT instead of using standard whole breast RT was approximately $4.9 million per 1000 women.
Mean Costs for Whole Breast Radiotherapy Compared With Brachytherapy-Based Accelerated Partial Breast Radiotherapy, Radiation-Specific and 1-Year Costs, 2008 US$.

Note. RT = radiotherapy.
Multivariable Analyses Predicting Ratio of Costs for Whole Breast Radiotherapy Compared With Brachytherapy-Based Accelerated Partial Breast Radiotherapy.
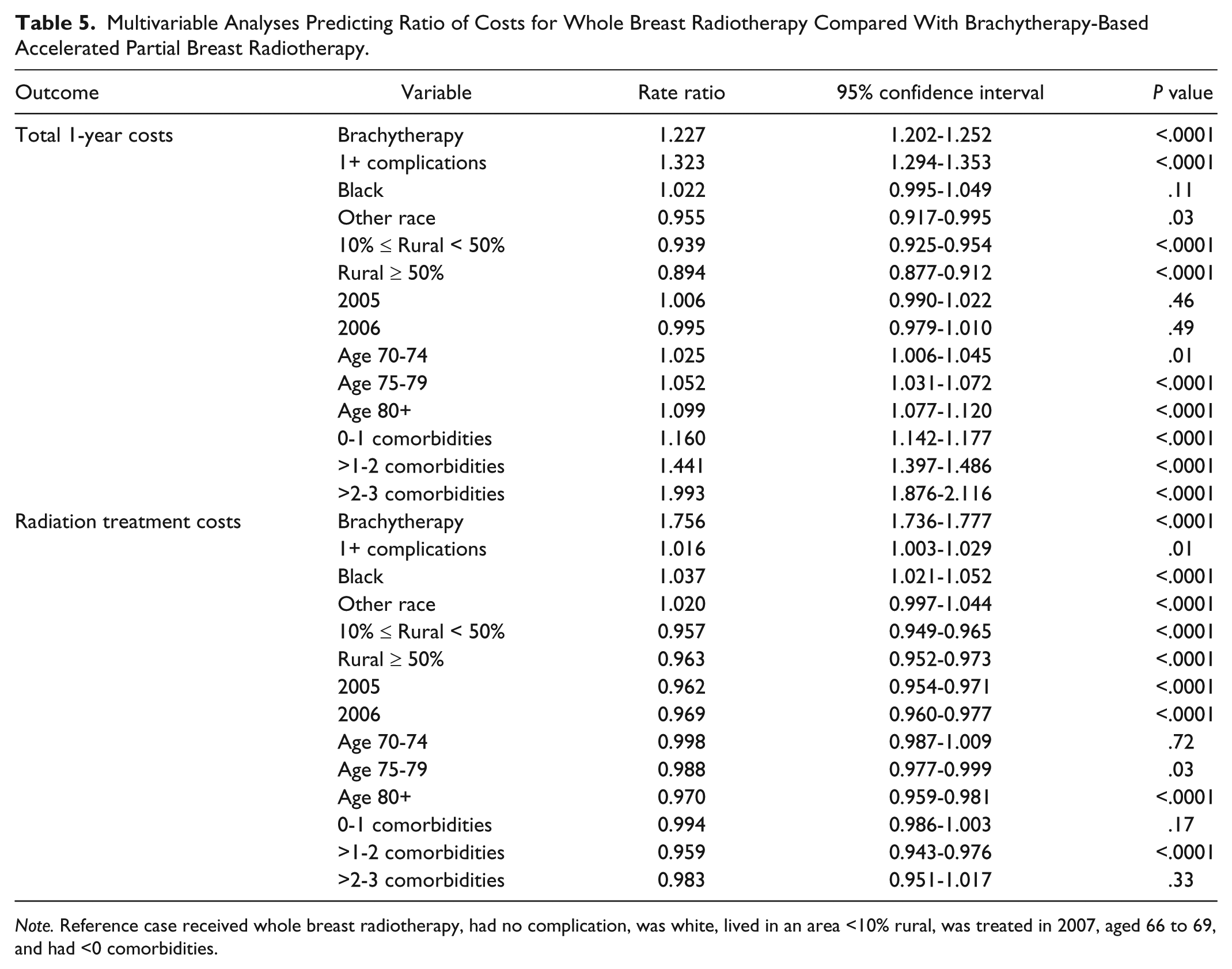
Note. Reference case received whole breast radiotherapy, had no complication, was white, lived in an area <10% rural, was treated in 2007, aged 66 to 69, and had <0 comorbidities.
Discussion
This study showed that the odds of infection and wound complication, seroma, breast pain, necrosis, and cellulitis were higher in balloon brachytherapy patients, and no complications were statistically more likely following whole breast RT. Furthermore, the treatment cost analysis showed that balloon brachytherapy was associated with 77% higher treatment costs compared with standard whole breast RT. Yet in this early time period, balloon brachytherapy–based accelerated partial breast RT diffused throughout clinical care in the United States 1 with limited wide-scale assessment of complications or costs associated with its use compared with standard whole breast RT. Based on our estimates, Medicare spent an additional $28.8 million on brachytherapy-based accelerated partial breast RT treatment for our cohort alone, beyond what standard whole breast RT would have cost (ie, $4886*5898). This new radiation treatment modality increased treatment-related complications and health care costs before long-term evidence proved its effectiveness.
Compared with other work in this area, we honed in on a focused patient cohort, one that would be more likely recommended for brachytherapy-based RT based on professional society guidelines, because patients receiving, for example, chemotherapy, had more advanced cancer and may have been at differential risk for complications. Our cohort of nearly 48 000 Medicare beneficiaries that was tailored to be as homogenous as possible with regard to disease stage saw much lower rates of complications by RT modality compared with other studies.24,25 Other investigators have found much higher absolute rates of infectious and noninfectious complications compared with our results.24,25 This could be due to their broader sample selection that included all use of brachytherapy RT. We also note that we were comparing complications of a new therapy during a steep learning curve phase with a tried-and-true practice in effect for nearly 30 years, and absolute rates of complications likely will decrease further over time. Others’ analysis of comparable data from 2008 to 2010 showed some improvements in patient selection over time, which might represent physicians learning about optimal selection and could improve short- and long-term outcomes. 31
Many complications were identifiable in Medicare claims data, although complications requiring an intervention or procedure were more likely to be found. Minor complications that can be handled with routine follow-up typically are not billed, and therefore, they will not be apparent in claims data. However, complications requiring additional treatment or diagnostic testing, such as re-excision, intravenous antibiotics, or hospitalization, should be more easily identifiable within 1 year of RT. We did not have information about the use of antibiotics before, during, or after treatment, however. Due to the 1-year follow-up period, we excluded other long-term complications such as pericarditis and pulmonary fibrosis, which could be associated differentially with different forms of RT but are hard to measure and extremely rare in 1 year of follow-up. It is possible that brachytherapy-based accelerated partial breast RT reduces long-term side effects to heart and lung, while increasing short-term side effects that are measured in this study. In general, using claims data and limiting follow-up time may underestimate the number of complications. Furthermore, fully informed patients may have chosen treatment convenience and the risk of a short-term infection or seroma, which are correctable, over a longer treatment course and potential longer term risks of cardiovascular disease or lung fibrosis, which are permanent. In addition, all forms of accelerated partial breast RT will offer patients a second chance at breast RT should they experience a second cancer or recurrence.
Our large, population-based study of older women with early invasive breast cancer indicated that rates of several specific complications were higher in the year following balloon brachytherapy–based accelerated partial breast RT compared with traditional whole breast RT, although hospitalization, burn, and fibrosis were not significantly different from each other by RT modality. A more recent study comparing 2-year complication rates across many types of breast RT in a Medicare sample appears to show overall complications slightly decreasing over time (2005-2011), although annual estimates were not published; 32 this may reflect improved patient selection and physician experience with the new technology over time. With some complications being extremely rare, smaller registries or single-institution studies simply cannot robustly estimate complication risks. Our results showed lower absolute predicted rates of complications in a more homogenous cohort than other early studies.24,25
Medicare covered broad use of this technology before long-term evidence of its effectiveness was shown, yielding a tremendous cost. We know that nonclinical factors partially influenced the use of this new technology.1,33 For example, brachytherapy-based accelerated partial breast RT comes with explicit financial incentives for surgeons to become involved in radiation treatment, because they receive a device implantation fee, which does not happen with traditional whole breast RT, and they may also have pressures from colleagues or patients to use new treatments.1,33 Furthermore, there was no consensus about technology adoption from the medical community, 33 making it difficult to have a “coordinated approach to evidence generation.” 34 It would have been prudent for the Centers for Medicare and Medicaid Services to develop additional RT treatment registries to gather sufficient evidence of effectiveness prior to widespread, open dissemination, as well as tie reimbursement to clinical data collection. This example highlights the need for creating appropriate financial payment models to encourage data collection for evaluation of new treatment modalities, both during the early phase of adoption where there may be steep learning curves for patient selection and technology or treatment application and as the treatment diffuses and experience matures.
Supplemental Material
SuppTable-apbi_cost-comps-2018-01-09-REVISED – Supplemental material for New Breast Cancer Radiotherapy Technology Confers Higher Complications and Costs Before Effectiveness Proven: A Medicare Data Analysis
Supplemental material, SuppTable-apbi_cost-comps-2018-01-09-REVISED for New Breast Cancer Radiotherapy Technology Confers Higher Complications and Costs Before Effectiveness Proven: A Medicare Data Analysis by Heather T. Gold, Dawn Walter, Eleni Tousimis and Mary Katherine Hayes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Gold recieved funding from the National Cancer Institute (R03 CA161752) for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.