
Abstract
The provision of professional interpreting services in the hospital setting decreases communication errors of clinical significance and improves clinical outcomes. A retrospective audit was conducted at a tertiary referral adult hospital in Brisbane, Australia. Of 20 563 admissions of patients presenting to the hospital emergency department (ED) and admitted to a ward during 2013-2014, 582 (2.8%) were identified as requiring interpreting services. In all, 19.8% of admissions were provided professional interpreting services in the ED, and 26.1% were provided on the ward. Patients were more likely to receive interpreting services in the ED if they were younger, spoke an Asian language, or used sign language. On the wards, using sign language was associated with 3 times odds of being provided an interpreter compared with other languages spoken. Characteristics of patients including their age and type of language spoken influence the clinician’s decision to engage a professional interpreter in both the ED and inpatient ward.
Keywords
Introduction
Communication and language are essential to the delivery of optimal medical care. 1 The conversation between health care providers and patients is of both diagnostic importance and therapeutic benefit, 2 so it is not surprising that language barriers contribute to health care disparities for people of limited English proficiency (LEP).1,3-8 When professional interpreting services are not engaged, patients receive inferior health care with respect to both decreasing quality and safety.2,3,8-11 They are less likely to adhere to medical treatment and are more likely to have poorer health-related outcomes.2,3,8,9 Errors of clinical consequence are more likely to be made when an ad hoc or no professional interpreting is provided, exposing patients to increased risk of adverse events, and clinicians to greater medicolegal risk.5,10,12
Language barriers for patients with LEP and those who are deaf can be addressed through the provision of language interpreting services. The engagement of professional interpreters for LEP patients is associated with decreased communication errors of clinical consequence, increased patient and clinician satisfaction with care, increased appropriate health care utilization, and improved clinical outcomes.4,5,8,10,13-15
The contribution of provision of professional interpreting services to LEP patients to patient, health, safety and satisfaction is well-evidenced, but the rates of professional interpreting provision in the majority of health care settings in Australia and New Zealand, including hospitals, remain inadequate.12,16,17 Rates of professional interpreting provision of below 40% for LEP patients have also been shown consistently in hospital settings in the United States where much of the research on the health dangers of nonprovision of professional interpreting has been conducted. The use of professional interpreters for Spanish- and Chinese-speaking LEP patients across 2 urban hospitals in San Francisco was shown to be low with 17% provision at admission and 14% since admission with physicians and only 4% provision overall with nurses at any point of the patient hospital journey. 18 Lopez and others reported a rate of professional interpreter provision of 34.2% for hospitalized LEP patients at a large tertiary academic hospital. 11 Based on a survey of physicians practicing in San Francisco, more than two-thirds of respondents (66% of 158) reported that they had not used an interpreter about twice in the prior month but wished they had. 1
There are few published figures available for professional interpreting provision in Australian hospital and health care settings. The figures available show low interpreting provision similar to these reported for US hospitals and health services. A cross-sectional study of interpreter usage in a pediatric emergency department (ED) in New South Wales (NSW), Australia, found that 36% of respondents identifying themselves as requiring an interpreter at the ED received professional interpreting services. 16 Using a combined patient phone survey and medical record audit, Garrett and others showed similar rates of professional interpreter engagement (35.6% and 31.2%, respectively, for each method) for overall stay in an adult hospital (including ED) in NSW. 17 Gray and others reported a rate of provision of professional interpreting services in a primary health care center in New Zealand of 39%. 12
New Contributions
Australia, like New Zealand, the United States, and the United Kingdom, is becoming an increasingly culturally and linguistically diverse society raising the imperative of provision of professional interpreting services for effective hospital care. Nearly 4 million Australians, comprising 19.2% of the population, speak a language other than English at home, and 3.2% of the population speak English either “not well” or “not at all.” 19 In the 5 years between the 2006 and 2011 census, the rates of increase in language diversity and numbers of LEP residents in the population (125% and 117%, respectively) have far exceeded the rate of population increase (108%).19,20 Thus, the need for Australian hospitals to provide effective communication services for safe and quality care of Australians is ever increasing in importance. The integral role of professional interpreters to medical care for LEP patients in Australia has been recognized through the development and implementation of a number of state government policies.21,22 The Queensland (Australia) Government Language Services Policy states that the policy will be delivered through (1) engagement of qualified interpreters in circumstances where people experience difficulties in communicating in English, (2) provision of multilingual information, and (3) training of staff in how to work with interpreters. 21 The aims of the current study were to determine the rates and patterns of interpreter provision for LEP patients admitted through the ED of an academic adult hospital in Brisbane, Australia. We also wanted to investigate any differences in characteristics between LEP patients provided and not provided with interpreting services. We then wanted to explore whether these differences were consistent with the commonly cited reasons for nonengagement of professional interpreters in hospital settings, time, and cost.
Methods
Approval to undertake this audit study was granted by the relevant hospital Human Research Ethics Committee.
The setting is an inner city tertiary referral adult hospital in a major metropolitan area of Australia. It is part of a larger hospital complex, including private and public inpatient facilities with a full range of medical, surgical, and obstetric specialties. A retrospective audit of all LEP patients admitted as inpatients through the ED was conducted for 2 calendar years (2013-2014). This population was chosen because they most likely represent the sickest patients presenting to the ED and thus the most likely to benefit from access to a professional interpreter. There were a total of 20 563 admissions of patients through the ED to the adult hospital over the 2 years.
Patients requiring an interpreter who were admitted to the adult hospital were identified using the Emergency Department Information System (EDIS) database.
The “interpreting required” field of EDIS is based on the combination of (1) patients’ existing electronic administrative hospital record (iPatient manager [iPM]) that includes 3 interpreter fields (a tick box for interpreter required, an interpreter alert flag, and language required) and (2) a question asked verbally at ED admission about the patient’s need for an interpreter. For all admissions of patients identified as LEP (based on “interpreter required” field), demographics (gender, age, and language spoken), admission and discharge date and time for both ED and ward, length of stay, and readmission within 30 days were obtained from the hospital iPM database using the patient identification number and date/time of admission for data matching.
All booked professional interpreting occasions at the hospital are recorded in an external interpreter services database, “the Interpreter Service Information Service (ISIS),” managed by the State of Queensland health department (Queensland Health). Using patient UR numbers, admission and discharge dates, and patient name, interpreting records were manually matched to all LEP patient admission occasions. Date and time of each interpreting request, language, and duration and mode (telephone or face-to-face) of interpreting were recorded for each admission.
All 3 data sources were merged for each LEP admission onto an Excel spreadsheet. The specific data variable examined were gender, age, language spoken, length of stay (both ED and ward), duration and mode (telephone and face-to-face) of interpreting, occasions of interpreting service, and 30-day readmission. The results of the relationship between interpreting provision, length of stay, and readmission rates are reported in a separate publication. 23 The data were analyzed using IBM SPSS Statistics 22.
The retrospective audit design restricted the investigation to provision of formal professional interpreting and did not ascertain informal interpreting from family members and bilingual staff.
Results
During the 2-year period from January 1, 2013, to December 31, 2014, of a total of 20 563 patient admissions to the adult hospital through the ED, 582 (2.8%) were identified as LEP and requiring an interpreter. This LEP admission total included 218 admissions in 2013 and 364 in 2014, an increase of 67.0% from the first to the second year. A total of 458 patients comprised the 582 admissions.
The demographics of the 458 patients are summarized in Table 1. More than two-thirds (67.9%) of LEP patients were female. The average age was 59.1 (SD = 23.0). A total of 63 different languages were spoken by the LEP patients. The most frequently spoken 10 languages only comprised 62.0% of patients.
Characteristics of Patients Identified as Requiring an Interpreter.

Table 2 shows the pattern of interpreting provision for the 582 hospital admissions. Of the 582 total admissions, 115 (19.8%) were provided professional interpreting services during their ED stay and 152 (26.2%) were provided this during their ward admission. In all, 366 (62.9%) of patients were not provided professional interpreting services at any point of their hospital stay. Table 3 shows the distribution of numbers of occasions of professional interpreting provided per admission. For those patients provided professional interpreting services, the average number of occasions provided was 1.91 (SD = 1.24).
Patterns of Interpreting Provision—ED and Ward.
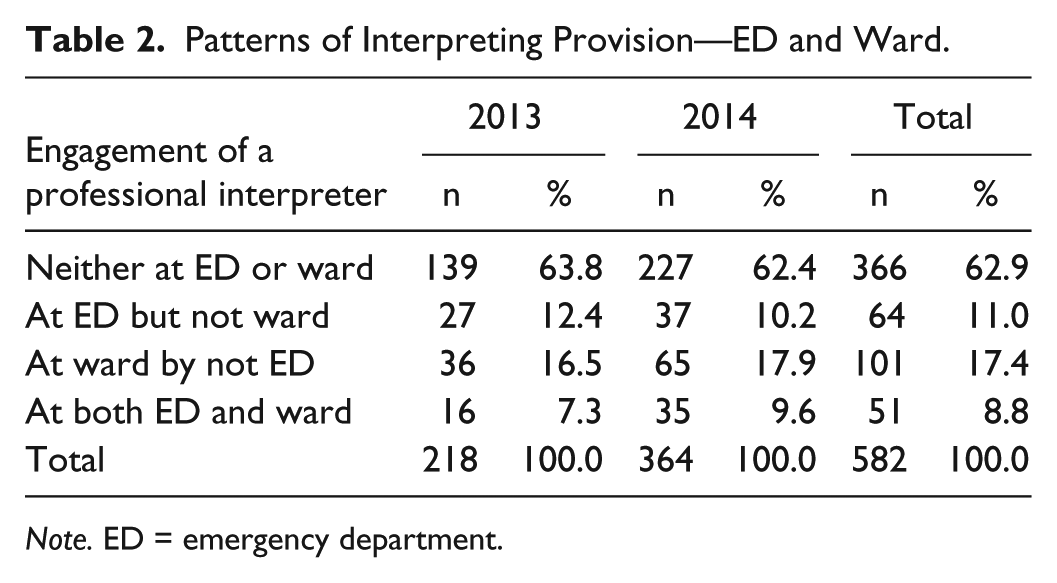
Note. ED = emergency department.
Distribution of Numbers of Occasions of Interpreting for Admissions.

Patients were more likely to receive interpreting services in the ED if they were younger (odds ratio [OR]: 0.98, confidence interval [CI]: 0.97-0.99, P = .003), spoke an Asian language (OR: 1.9, CI: 1.0-3.5, P = .04), or used sign language (OR: 7.0, CI: 2.2-21.6, P = .001). On the wards, using sign language was associated with 3 times odds of being provided an interpreter compared with other languages spoken (OR: 3.2, CI: 1.1-9.5, P = .04).
Discussion
As one of the few published rates of interpreting provision in a hospital setting in Australia, the findings of this study are important for a number of reasons. Our results show that the rates of 37.1% of LEP patients having a professional interpreter engaged to aid their communication throughout their hospital journey in this Australian setting are similar to rates between 34% and 39% reported for other hospitals and health care settings in Australia and the United States.4,11-13,17 Similar to the situation for hospitals in the United States, even with government and hospital policies and guidelines in place and professional interpreter services available on site and via phone, the majority of LEP patients experience their entire hospital stay without encountering a professional interpreter.
Of major concern is the lower rates of professional interpreting provision found in the ED. Important communication in ED includes eliciting sufficient patient history for making time-critical, effective, and safe clinical decisions. 24 Miscommunication between patients and providers has been shown to be a common occurrence in emergency medicine and in the United States has been identified in more than 70% of malpractice allegations. 25 Given that 80% of diagnosis depends on oral communication, 26 communicating without a professional interpreter significantly increases this risk.5,10
Our results showed that less than 1 in 5 LEP patients, 19.7%, were provided professional interpreting services at ED. Again, this rate is comparable with other rates of ED professional interpreting provision in Australia, the United States, and the United Kingdom with reported rates varying from 4% to 36%.16,27-29
So why in a hospital setting where interpreter engagement is encouraged through policy and availability of hospital in-house and contract interpreters and information on engaging other interpreters face-to-face or by phone is readily accessible, is there such an underuse of these services? This finding of underuse of interpreters even when they are available is consistent with the literature1,30 making reasons often cited by physicians for underuse such as time and limited interpreter availability insufficient. 31 In a qualitative study exploring physician decision making for interpreter engagement, Diamond and others found that physicians (1) know how to access interpreters and contribute to better care but weigh these benefits up with competing demands on their time, (2) are enticed by the convenience of using untrained interpreters such as family members and are often unaware of the difficulties associated with this until learning from their own experience, and (3) normalize the underuse of professional interpreters despite recognizing that patients with LEP are not receiving equal care. 31
Overestimation of patient’s language skills or “false fluency” of the patient has been shown to be a barrier when there is uncertainty in general of the understanding of communication in the context of ED, even when patients speak fluent English. 26 The availability of family members to interpret in the context of a hectic and chaotic setting where time pressures are high and the engagement of ad hoc interpreters is the norm appears to be an even greater obstacle to professional interpreter engagement in the ED.24,26 Older Greek, Italian, or Spanish patients may be more likely to be accompanied by adult children to the ED who may be more willing to interpret. Our finding that older people speaking European languages such as Italian, Greek, and Spanish are significantly less likely to be provided with a professional interpreter through their hospital journey is consistent with availability and willingness of family members to interpret, which can influence clinician decision making more than cost. Although sign-language interpreters are costly and take more time, patients needing sign-language interpreting are 7 times as likely to be provided professional interpreting services. This different approach lends support to the argument that availability of willing ad hoc interpreters and “false fluency” are greater obstacles to professional interpreting services than time and cost. 26
The association between language required and provision is consistent with the interpreting available through hospital employed interpreters available for the 2 most commonly spoken Asian languages (Mandarin and Vietnamese). The data support the hypothesis that interpreter use is higher if support is provided by an in-house rather than a contract interpreter. The availability of in-house interpreters makes face-to-face interpreting more available and relationship building between clinicians and interpreters more possible.
A limitation of this study is that complexity or severity of patient condition, likely influencing interpreting provision, was not included in measurement. The retrospective design means that only those encounters that were recorded were included, and analyzed. The study was conducted in one academic hospital in Australia and may not be generalizable to other settings throughout Australia and the world.
There are a number of national and state laws, policies, and standards relevant to the provision of accessible and equitable health care such as the Commonwealth Racial Discrimination Act 1975, the Queensland Anti-discrimination Act 1991, the Department of Health Agency Multicultural Plan 2013-2015, and the National Safety and Quality Health Service Standards.32-35 Provision of professional interpreting services to those patients who require it to enable communication for equitable access to safe health care is required for effective implementation of these current laws, policies, and standards.
Although policy and guidelines in health care settings are important, they typically do not refer to the complexities and logistics of interpreter engagement and on their own have been shown to have limited impact on rates of provision.12,28 Consistent with the literature, our findings suggest that increasing professional interpreter engagement will require interventions at both the level of the individual and the unique environments of the ED and wards. 31 Establishing cultural norms, structural changes, and training for clinicians in working effectively with interpreters is needed.1,8,12,31
Cultural change means a shift away from the barrier of perceived costs of interpreting and education around the costs of potential medical errors associated with the nonprovision of professional interpreters.5,10 It also means not “getting by” with the use of ad hoc interpreters such as family members or bilingual staff. 36 Structural changes require environments that are conducive and practical for interpreter engagement. These include wireless speakerphone availability in both ED and wards. 37 Training clinical staff in understanding the interpreter role as well as the evidence-based benefits of their engagement is critical—both for improved patient outcomes and decreased medicolegal costs.5,10,38,39 Finally, it is important to give clinicians confidence in interpreter quality by increased training in medical knowledge.
Conclusion
Our study shows an underuse of professional interpreters for LEP hospital patients consistent with the Australian and international literature,11,12,16-18,27-29 The patient characteristics associated with interpreting provision are consistent with findings that clinician decision making is influenced by availability of ad hoc interpreters and the normalization of underuse of interpreters in the hospital setting. 31
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an internal Mater Foundation grant.