
Abstract
Amyotrophic lateral sclerosis (ALS) is a progressive, fatal neurologic disorder with predictable challenges regarding disease progression and end-of-life care. These include need for respiratory and nutritional support. Little is known about how such choices impact end-of-life health service utilization for these patients. Using OptumLabs Data Warehouse, a large administrative claims database with more than 150 million privately insured, geographically diverse enrollees, we sought to explore outcomes associated with the use of enteral nutrition (EN). Patients were of age ≥18 years, with first ALS diagnosis during calendar years 2006-2012, and 6 months of continuous health plan coverage before first diagnosis. EN use was identified using procedure codes. Data were summarized descriptively. Among 1974 patients with ALS, mean age was 60.0 ± 12.5 years, 41.8% were women, and 9.7% demonstrated use of EN. Median time from ALS diagnosis to evidence of EN was 211 days (interquartile range [IQR]: 70-426). Those receiving EN had greater aggregate comorbidity (47% with Charlson-Deyo Comorbidity Index ≥ 3 vs only 27% in non-EN subset). In total, 38.1% of patients had at least 1 hospitalization, with median time to hospitalization of 162 days. Unfortunately, the EN group ended coverage a median of 155 days after EN started (IQR: 63.5-388), thereby limiting ability to capture outcomes. Although many ALS patients were identified, EN use was lower than expected, due to being earlier in disease trajectory and lost to follow-up with transition from private insurance. As such, databases exclusively including privately insured patients may be suboptimal for detecting late complications of protracted illnesses.
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS) has a progressive and often predictable clinical course leading to consideration of respiratory and nutritional support in most patients. While enteral nutrition (EN) is often considered for weight stabilization and to prevent malnutrition associated with worse clinical outcomes for patients with ALS, 1 no studies have definitively demonstrated that EN improves survival in this population. Although early advanced care planning in ALS is advocated for,2,3 little is known about how utilizing or foregoing EN impacts health services utilization for patients with ALS. Given the difficulty of studying rarer diseases in younger patients who are usually not included in Medicare databases or cared for in high volumes at large institutions, we sought to explore outcome differences for patients with ALS who received or did not receive EN. Given that ALS often can affect patients before they would otherwise be eligible for or enrolled in Medicare, we believed this method of using a large database with many privately insured patients was logical and coherent to answer such clinical questions.
Materials and Methods
We conducted a retrospective analysis of data from the OptumLabs Data Warehouse (OLDW), a large database housing administrative claims data on more than 150 million privately insured enrollees from throughout the United States.4,5 This database includes claims for individuals enrolled in private health care plans as well as Medicare Advantage, 6 and provides a rich diversity of data, as described in Table 1. We identified all patients 18 years or older who had their first ALS diagnosis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code: 335.20) between January 1, 2006, and December 31, 2012 (n = 10 058). We required at least 2 diagnoses of ALS (on different days, made within a 1-year period) and 6 months of continuous health plan coverage before their first diagnosis, as well as valid information regarding birthdate and gender. In all, 1974 patients comprised the cohort analyzed.
Types of Data in the OptumLabs Data Warehouse.
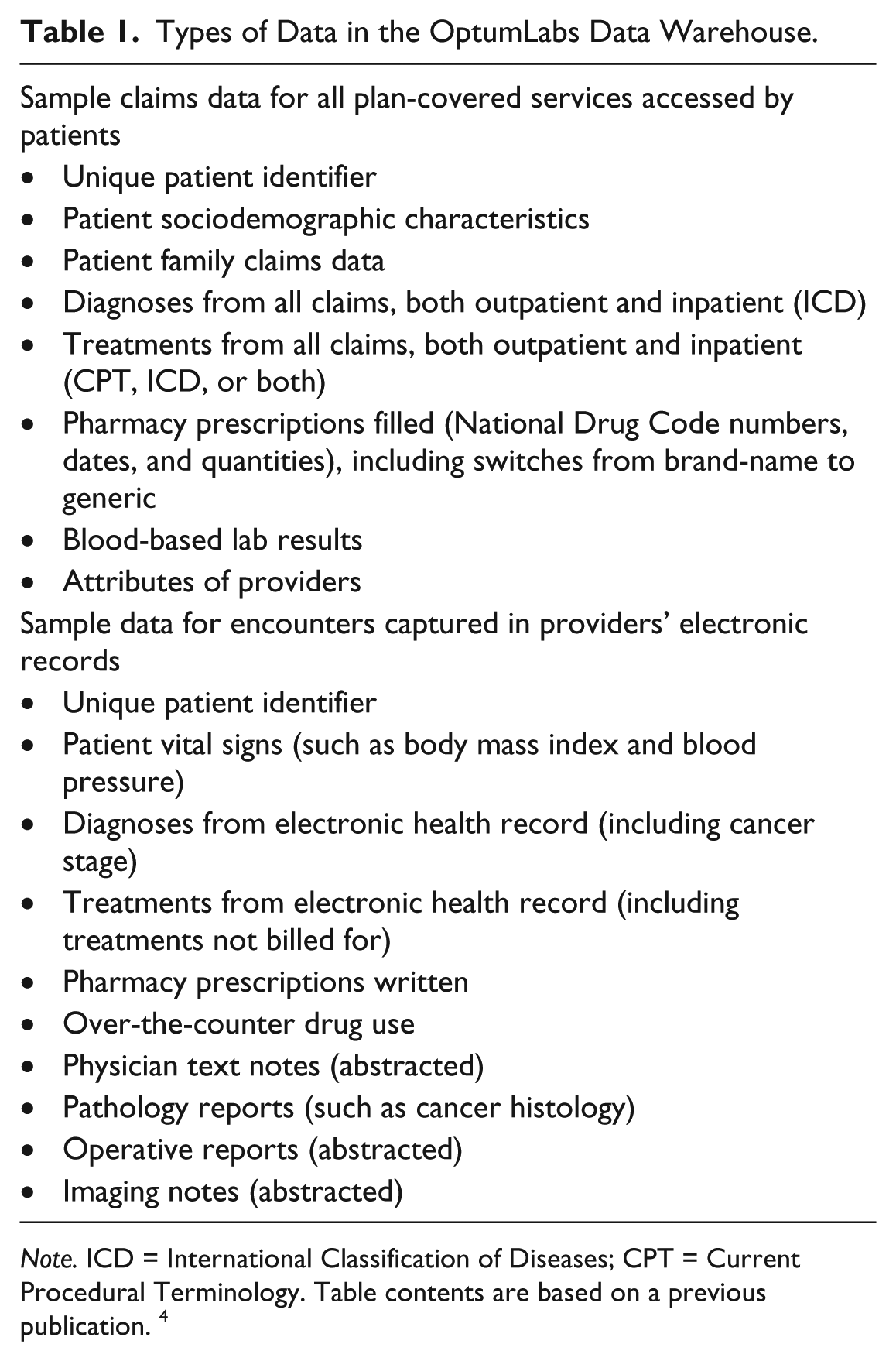
Note. ICD = International Classification of Diseases; CPT = Current Procedural Terminology. Table contents are based on a previous publication. 4
EN use was identified using ICD-9 procedure codes for percutaneous endoscopic gastrostomy/jejunostomy placement or replacement; or infusion of concentrated nutritional substances; or Current Procedural Terminology, Version 4 (CPT-4) procedural codes related to open or closed tube insertion including gastrostomy, jejunostomy, gastrojejunostomy, or replacement of these tubes, regardless of placement method (see Table 2). Data were summarized descriptively; baseline characteristics, by EN status, are presented as mean and standard deviations for continuous variables and as frequencies for categorical variables. Pursuant to the Health Insurance Portability and Accountability Act, the use of de-identified data does not require Institutional Review Board approval or waiver; however, our protocol was reviewed by the Mayo Clinic Institutional Review Board and was approved.
Characteristics of Entire ALS Cohort and Subset Receiving EN.

Note. ALS = amyotrophic lateral sclerosis; EN = enteral nutrition; ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification; CPT = Current Procedural Terminology.
ALS diagnosis made using ICD-9-CM diagnosis code 335.20.
EN subset defined indirectly by evidence of placement of feeding tube (gastrostomy, open or percutaneous ± endoscopic, jejunostomy, or enteral nutrition). Included ICD-9-CM procedure codes for percutaneous endoscopic gastrostomy or jejunostomy or replacement (43.11, 43.19, 46.32, 97.02) or infusion of concentrated nutritional substances (96.6); or CPT codes for procedures related to open or closed tube insertion including gastrostomy, jejunostomy, or gastrojejunostomy, or replacement of these tubes (43653, 43760, 43830, 49440, 49446, 44186, 49441, 49451, 49452, 43246, 44187, 44015).
Results
Of the 1974 patients with ALS, mean age was 60.0 ± 12.5 years, 41.8% were women, but only 192 (9.7%) demonstrated the use of EN (Table 2). The median time from diagnosis of ALS to evidence of EN was 211 days (interquartile range: 70-426). Those receiving EN had greater aggregate comorbidity (47% with Charlson-Deyo Comorbidity Index ≥ 3 vs only 27% for the non-EN subset). In total, 38.1% of all patients had at least 1 hospitalization, with median time to hospitalization of 162 days (Table 3). The top 3 reasons for hospitalization related to the clinical nature of this disease entity: namely, the diagnosis of ALS and occurrence of either respiratory failure or aspiration pneumonia which were the most commonly encountered diagnoses and related to the hypothesized situations in the “Introduction” section.
Hospitalization-Related Issues in ALS Cohort.

Note. ALS = amyotrophic lateral sclerosis; IQR = interquartile range.
While the overall mean follow-up after ALS diagnosis was 1.6 ± 1.4 years, patients in the EN group ended coverage (and thus inclusion in the OLDW) a median of 155 days after EN started (interquartile range: 63.5-388), thereby markedly limiting our ability to longitudinally capture their outcomes from EN commencement moving forward. Direct statistical comparison between the EN and non-EN group was not performed and was deemed to be an invalid comparison, as the time from ALS diagnosis to when EN was actually started could not be determined in this dataset. The summary information from each group is included in Table 2. When grossly comparing the EN with the non-EN groups, it appears that those who received EN or did not were fairly similar except the incidence of cerebrovascular disease was substantially higher in the EN subset (39% vs 26% in non-EN set).
Discussion
While equipoise may exist regarding benefits of EN in ALS, 7 the American Academy of Neurology recommends early EN, noting that EN’s impact on quality of life has not been definitively studied to date. 1 One benefit associated with early EN utilization is that the substantial amount of time that it takes for patients with ALS to eat and be fed their food has been associated with caregiver burnout and fatigue and increased frustration by patients. Even though periprocedural respiratory complications had been a concern in the past, it appears that perioperative risks are manageable and that EN tube placement can be done safely for most patients with ALS. 8 At our institution, it is typical to have patients electively admitted for placement of a percutaneously inserted gastrostomy (PEG) tube, with follow-up observation of respiratory status overnight as an inpatient, suggesting the possibility that the index hospitalization for EN commencement is not due to other comorbid conditions.
As the overall disease incidence of ALS is low, we opted to leverage use of a large claims database versus utilizing smaller single-center experiences which has been the basis of most extant literature. 7 This seemed to be a reasonable baseline assumption, because ALS diagnosis is often made between ages of 45 and 65 years. We hypothesized that using OLDW, which includes patients of all ages 18 years or older, would enable us to capture more patients with ALS than a Medicare-based approach. Although this did introduce an element of selection bias, the goal of using OLDW was to obtain the largest yield overall of patients with ALS. Despite the fact that a large number of patients with ALS were identified, EN use rate appeared to be much lower than expected (<10%) which suggested some unforeseen challenges and difficulties exist in studying a disease such as ALS with the OLDW.
First, we suspect the low detected rate of EN use may reflect that some patients with ALS were still at an early illness stage at the study’s end and did not require EN yet. Next, despite a broad range of ICD-9 and CPT-4 procedure codes used to capture EN use, it is possible capture was suboptimal and not all patients using EN were captured appropriately. Third, some patients likely ended being covered by private insurance as their disability progressed; thus, OLDW capture also ended when the patient switched to a government-sponsored disability coverage during their protracted illness. With this, the length of follow-up was suboptimal. Collectively, these reasons could potentially explain the low rate of EN and the shorter-than-expected time from EN to death observed in this cohort. As such, databases exclusively including privately insured patients may be ideal for early event identification affecting younger patients less likely to be covered by government-based insurance; however, this approach may be suboptimal for detecting late complications of chronic protracted illness.
As this was a retrospective review of de-identified data, the ability to further abstract more granular variable focused on individual patient outcomes was not possible. This limited our ability to report on specifics such as clinical status during index hospitalization when EN was begun (elective or in context of complications or clinical decline), or more detailed stratification of patients by pulmonary status (based on forced vital capacity, as is recommended by the American Academy of Neurology). OLDW reports the data in a de-identified fashion and in aggregate, so specific clinical data such as would be derived from clinical notes are not available to investigate.
Also, as this clinical question involves a question of morbidity in one group versus another, being aware of when disease progress and eventual death occurs is an important consideration. Unfortunately, we were unable to determine exactly why enrollees ended their coverage—whether this was related to death, change in coverage, or a change over to a government-based insurer—and this limits the utility of the OLDW for illnesses where death may be an outcome of particular interest. Last, there are further limitations to the generalizability of OLDW across all populations, as the dataset contains only privately insured and Medicare Advantage enrollees; thus, the conclusions may not necessarily be generalizable to Medicaid, Medicare fee-for-service, or uninsured populations.
To date, the OLDW has sought to bring together diverse practitioners to collaborate on agenda-setting related to clinically relevant questions and translation of these results into practical changes that directly impact patient care. From the outset, the OLDW has encouraged clinical questions that promote observational studies that could “achieve results as close as possible to the estimate one would get from a randomized trial designed to answer the same question.” 4 Indeed, investigations of patients with heart failure,9,10 stroke,11,12 diabetes, 13 and atrial fibrillation,14,15 among others, have been successfully completed, and such results have been valuable at informing clinical practice patterns. As a major goal of the OLDW is promoting translation of research into practice, the clinical question regarding EN use in ALS seemed to be an ideal one to be answered by OLDW. However, the above limitations unexpectedly yielded suboptimal results that did not allow us to answer our clinical questions as intended. Furthermore, as the commencement of EN is an elective or optional intervention, retrospective analysis of such interventions may be hampered by the fact that the reasons for proceeding with the intervention (risk factors) are also the same as risk factors of the intervention itself.
Conclusions
Determining best practice for recommendations regarding EN in ALS is an aspirational goal to promote patient-centered outcomes. To date, the OLDW has been consistently successful in answering clinical questions related to chronic and serious illness. Despite a thorough search strategy and identification of almost 2000 patients with ALS, questions still exist about how to best operational care for patients with ALS and nutritional challenges. We hope that lessons learned by this analysis inform future researchers that despite having a large robust database, that big data, in and of itself, do not guarantee a successful outcome of a given research question. Future studies of questions like the one posed here may require the ability to link multiple data sources to optimize the ability to longitudinally follow patients across the illness spectrum from diagnosis through death.
Footnotes
Acknowledgements
The authors thank Ms April E. Horne for her thoughtful assistance with data acquisition and review, Ms Dora M. Gibbs for her assistance with billing and coding clarification, and Dr Eric J. Sorenson for his assistance with initial concept refinement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by Clinical and Translational Science Awards (CTSA) Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH.