
Abstract
This study explores the recruitment and retention conditions influencing primary health care (PHC) human resources for health (HRH) in Qatar and suggests strategies for their improvement. A qualitative design employing semistructured key informant interviews with PHC stakeholders in Qatar was utilized. Key interviewees were originally recognized, and snowball sampling was used to identify additional interviewees until reaching saturation point. Interview scripts were transcribed and then analyzed thematically using the Nvivo software package. Thematic analysis precipitated a number of themes. Under recruitment, the centrality of enhancing collaboration with academic institutions, enhancing extrinsic benefits, and strengthening human resources recruitment and management practices. Dedicated support needs to be provided to expatriate HRH especially in regard to housing services, children schooling, and streamlining administrative processes for relocation. Findings revealed that job security, continuous professional development, objective performance appraisal systems, enhanced job transparency, and remuneration are key retention concerns. The study provides a number of recommendations for the proper recruitment and retention of HRH. Health planners and decision makers must take these recommendations into consideration to ensure the presence of a competent and sustainable HRH in the PHC sector in the future.
Keywords
Introduction
For years, primary health care (PHC) has been recognized as a key, cost-effective health care component for enhancing public health through preventing the spread of infections and attenuating noncommunicable diseases (NCD).1-4 Literature reports multiple population health benefits for increased availability of PHC services, including reduced child mortality rates; decreased low birth weight; decreased mortality due to strokes, cancer, and heart illnesses; increased life expectancy; and decreased predicted potential years of life lost.2,5-7 From a health systems’ perspective, PHC is regarded as the optimal vehicle for delivering equitable health services, ultimately resulting in improved health outcomes with decreased health expenditure. 6
Human resources for health (HRH) are a critical component of any effective health care system. 8 An indispensable prerequisite to establishing a robust PHC system is the recruitment and retention of an adequate number of well-educated and qualified HRH. The need for effective PHC delivery complemented by a sustainable and competent supply of HRH is more heavily pronounced in the Eastern Mediterranean Region (EMR). In fact, the EMR ranked second to last in HRH densities, despite the established association between nurse and physician densities and better life expectancy with reduced overall mortality rates. 9
PHC Context in the State of Qatar
Supporting the growth of a sustainable PHC system along with required human resources is of particular concern to the Gulf Cooperation Council (GCC) countries.10,11 Qatar is one GCC country that has expressed interest in and launched various initiatives aimed at improving its PHC system’s capacity to enhance the health of the public and address growing population health needs. 12
In fulfillment of the above, “Amiri Decree No. 15” came into effect on February 20, 2012, and bestowed the Primary Health Care Corporation (PHCC) complete administrative and financial autonomy to oversee public PHC in Qatar. 13 PHCC runs 21 PHC centers with the majority located in Doha, Qatar’s capital (n = 13).13,14
To meet the growing health demands and achieve set goals of having PHC as the principal mode of care, Qatari authorities have acknowledged the need for diligent efforts to ensure an adequate supply of qualified primary care HRH, with particular attention to strengthening recruitment and retention strategies. 15
Objective and Significance
This study aims at soliciting the feedback of PHC stakeholders on the current HRH recruitment and retention strategies and the means to strengthening them to enhance HRH availability and tenure in the PHC sector. To the knowledge of the authors, this study presents the first systematic examination of the HRH recruitment and retention strategies in the ever expanding and strategically important PHC sector in the state of Qatar.
Methodology
Ethical Approval
The study obtained ethical approval from the Joint Institutional Review Board (IRB) in Qatar (IRB Number 13-00066), the PHCC’s Research Committee (Reference No: PHCC/RC/13/002, PHCC/RC/14/04/009), and the Social and Behavioral Studies IRB committee at the American University of Beirut (Protocol Number FHS.MA.05).
Study Design
The study utilized a qualitative study design involving a series of semistructured key informant interviews with PHC stakeholders in the state of Qatar.
Study Tool
A semistructured interview schedule, consisting of 13 open-ended questions, was used for interviewing stakeholders. Questions aimed at collecting information on stakeholders’ perception of PHC in the country and the existing recruitment and retention strategies. The interview schedule and subsequent interviews encouraged stakeholders to express additional thoughts and to recommend additional stakeholders relevant to the study utilizing snowball sampling. The original version of the interview schedule was developed in English and later translated into Arabic by a professional translator. Back-translation was carried out to ensure accurate translation of questions.
Stakeholder Selection and Data Collection
Stakeholders included coordinators, managers, academicians, researchers, primary care providers, health authorities, and parastatal organizations. This diversity in stakeholders offered a multifaceted description and understanding of HRH recruitment and retention.
The authors sought the advice of experienced Qatar-residing medical and public health experts, carried out an online review of PHC providers and authorities, and a review of the PHC context and players in Qatar to identify 5 key stakeholders who were invited to participate in this study . The initial 5 stakeholders included an academic institution dean, a medical college lecturer and educational program director, a semiprivate organization health center manager, a medical residency program director, and a program coordinator at a local health authority. Snowball sampling was utilized to identify additional key informants. Interviewing continued until the saturation point was reached. This was determined when additional interviewed stakeholders were neither providing new information nor suggesting any new key informants. In total, the study involved 11 key informants.
Stakeholders were invited through a package delivered to their offices containing an invitation letter and an informed consent. Out of 18 invited stakeholders, 11 accepted to participate in the interview. The reasons provided for nonparticipation were busy schedule and lack of authority to speak to research entities.
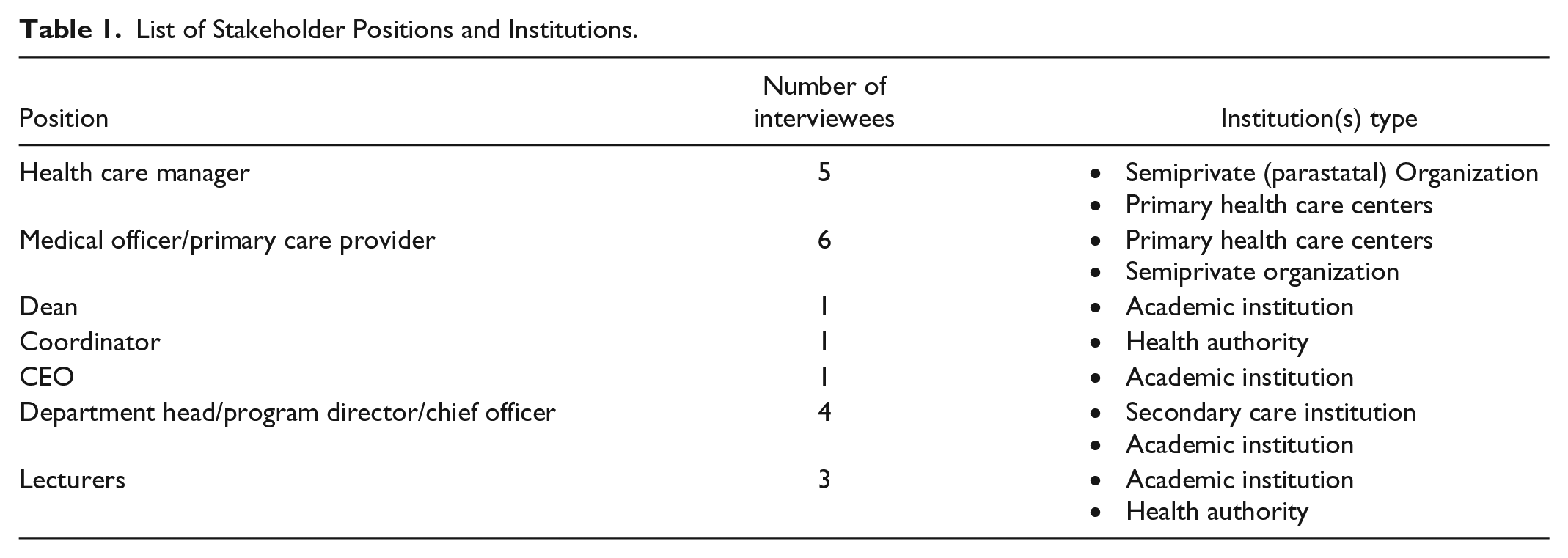
The majority of stakeholders were incumbents of more than 1 influential position, and in many cases at different institutions in the country. Table 1 offers a summary of the positions held by the interviewed stakeholders along with the type of institution they are employed at (the total does not equal to the total number of interviewees as reference is being made to the position rather than individual). Note that for confidentiality purposes, and due to the small size of the country and small number of institutions, the type instead of the name of the institution was included in Table 1. Only one of the stakeholders interviewed was of Qatari origin. All other stakeholders were expatriates of different nationalities (Western and Middle Eastern) working in Qatar. Although only 1 Qatari was included in the study, we believe the study’s findings are representative of the Qatari context, because expatriates constitute the great majority of the Qatari workforce and are the main working segments affected by recruitment and retention strategies and initiatives.
List of Stakeholder Positions and Institutions.
Over the course of 2 to 3 weeks after initial contact, stakeholders were followed up with 2 additional e-mails and a phone call to confirm their reception of the invitation and decision to participate. A favorable decision to participate was followed by arranging a time and place that met the stakeholder’s preferences and ensured their privacy and confidentiality. Interviews ranged between 30 and 60 minutes in duration. Upon receiving consent, interviews were audiotaped for a more detailed and accurate account and analysis of information. When stakeholders did not consent to audiotaping, interviews were conducted by 2 members of the research team; one led the interview while the other was engaged in meticulous note taking. All research members were fluent in both Arabic and English to accommodate for stakeholders’ preferences. Questions were supplemented by detailed probing, catered specifically to stakeholders with an academic and nonacademic background or profession.
Data Analysis
Audiotaped interviews were transcribed verbatim with special attention to accurately translating all Arabic phrases and/or answers into English. All interviews underwent extensive thematic analysis to identify the main themes generated by the study, the corresponding recruitment and retention recommendations, and the parties that are targeted by these recommendations.
The thematic analysis yielded a comprehensive, well-organized document of all responses, relevant quotes, and key recommendations. The document was further analyzed, and the answers were categorized into key themes and associated subthemes (Table 2). Two members of the research team, who later compared results, separately reviewed the final document and shared professional opinions to focus responses into agreed-upon themes, subthemes, and the findings associated with each.
Themes and Subthemes Emerging From the Study.
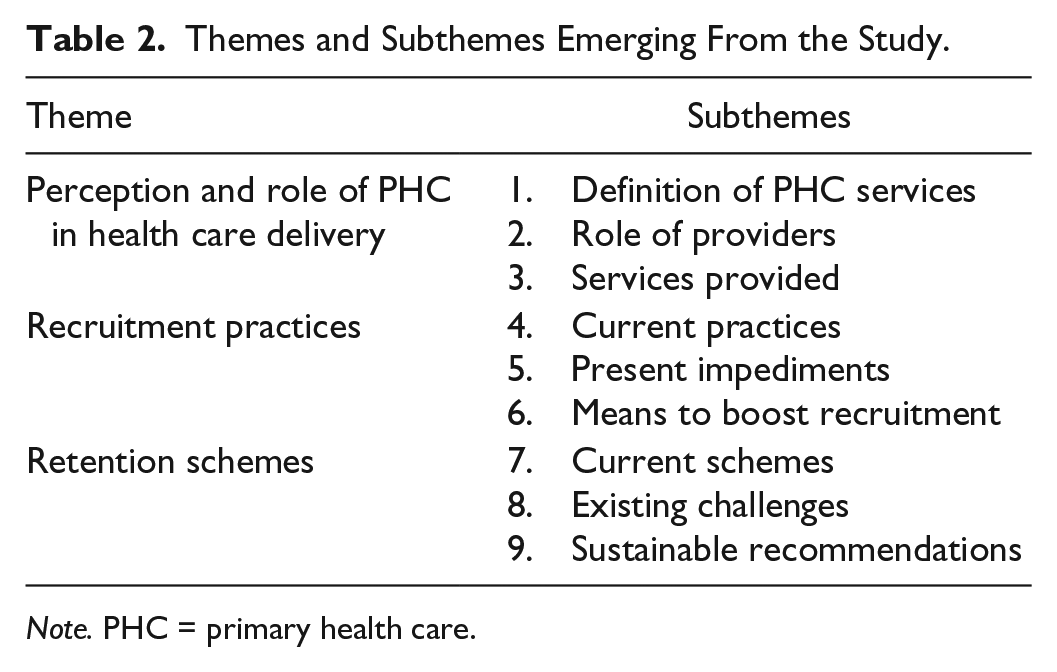
Note. PHC = primary health care.
Note that, unless otherwise stated, each direct quote is attributed to one source/stakeholder.
Results
Thematic analysis unearthed 3 major themes: (1) perception and role of PHC in health care delivery, (2) recruitment practices, and (3) retention schemes. Each of these themes was associated with a number of subthemes relevant to the objectives of the study (Table 2). Discussion of each themes and subthemes is presented below.
Perception and Role of PHC in Health Care Delivery
This theme sets the context of how PHC settings, personnel, and patient care are regarded, approached, and provided in Qatar. In regard to PHC definition, analysis revealed a variety of opinions as to what primary care is in the state of Qatar. A number of stakeholders described PHC by level of care and duration of treatment, as well as the extent of community involvement and participation. It was acknowledged as care throughout the cycle of life. Using the words of one of the interviewed stakeholders, PHC is defined as follows:
“PHC is care from birth to neonates to pediatrics to adolescent to adults to senior and geriatrics . . . ” and “effectively total care for the patient from cradle to grave.” (Family physician, medical lecturer, and program director at a primary health center and academic institution)
Other stakeholders defined PHC by the range of health care professionals delivering health care services, with a particular emphasis on family medicine (FM), internal medicine, obstetrics and gynecology (OBGYN), and pediatrics. In terms of role of the provider, suggestions were made that qualified nurses can attend to minor cases, which, aside from yielding cost and time-savings, enhances equitable access to care. Related to this subtheme was the definition of PHC care as the system that has a “gatekeeper for health services” (department head and lecturer at a secondary care institution and medical college). This was deemed by most interviewees as a cost-effective and time-efficient system for care delivery.
The third subtheme focused on boasting more comprehensive PHC services, for example, mental health services and screening, rehabilitation care, and family planning services. Shortcomings in the provision of such services were attributed to physicians lacking the time needed to perform a full screening and care procedures, as well as mental health illnesses being a cultural taboo. Furthermore, more emphasis on OBGYN preventive services was recommended. Such shortcomings are delineated in the following statement:
The only service available is screening for cervical and breast cancer. Other services for women . . . osteoporosis . . . obesity or wellness and health promotion services are not there. (Lecturer and coordinator at a health authority)
Greater efforts were also recommended to strengthen health promotion activities targeting children, parents, and students, as well as improved public acceptance of “taboo” diseases such as autism. Overall, more action at the community level was advised with PHC to encompass palliative and long-term care for NCDs.
Recruitment Practices
Although strategic recruitment measures are currently employed across PHC organizations in Qatar, many opportunities to strengthen capacities for meeting growing HRH demands were identified by interviewed stakeholders.
With respect to existing recruitment strategies, academic stakeholders described curricular restructuring in nursing and medical programs aiming at boosting future recruitment in the PHC sector, for example, holding more clinical practices and core rotations in community settings for medical and nursing students. Sponsorship of students by health care organizations was also recognized as a key approach to increasing the enrollment in specialties that would feed into the PHC system of care. Other recruitment strategies mentioned by the stakeholders included a plethora of benefits to attract professionals to the PHC sector, such as generous salaries, tax-free employment, health and dental coverage, and generous family benefits.
Present impediments
Interviewed stakeholders identified a number of impediments undermining effective HRH recruitment efforts. Such limitations were classified as those that fall under the control of the PHC sector and those that go beyond that control. With respect to the former, a number of impediments were identified including having no HRH recruitment strategy, inadequate recruitment skills, poor job descriptions, poor recruitment practices, and ineffective outsourcing of human resources recruitment services. Of particular concern for the stakeholders were the bureaucratic strains that delay or hinder the recruitment process. The quote below clearly highlights the magnitude of this problem:
After I applied, I took almost a year and half to join . . . from the beginning of submitting my CV until I got a final acceptance and joined . . . (Health care manager and primary care provider at a semiprivate organization)
However, certain limitations go beyond the control of the PHC sector. These include market shortages in HRH, specifically nurses and female physicians; strong competition for competent HRH within Qatar and among GCC states; and lack of competent HRH that can speak Arabic. Another issue that emerged relates to fresh graduates, specifically Qataris, seeking only managerial positions. The following stakeholder’s quote documents the intricacies of such hindrances:
. . . Graduates want to directly go into director positions even before gaining experience. (Chief officer at secondary care institution)
Means to boost recruitment
Stakeholders proposed multiple contextualized strategies to boost HRH recruitment (Table 3). A key recommendation entailed strengthening the degree of coordination among academic institutions to better satisfy market needs. This would entail Qatari universities and other academic institutions to collaborate on planning and implementing medical and health care education programs. Such collaboration could help fine-tune the HRH supply to the needs of the country (recommendation for recruitment) and ensure the offering of proper continuous education programs to in-service HRH (recommendation for retention). Furthermore, stakeholders suggested enhancing the sponsorship of students in health and medical majors that could feed into the PHC sector.
Stakeholders’ Recommendations for Enhancing HRH Recruitment and Retention in the PHC Sector.

Note. HRH = human resources for health; PHC = primary health care.
Expanded definition of certain recommendations:
Unified definition: Adopt a universal theoretical and working definition for PHC that would help providers set specific roles and differentiate between primary and more advanced levels of care and assist patients to better understand the level of care they need to seek based on the type and extent of their health issue.
Enhanced role for HRH: Nurses may assume certain responsibilities currently under the delegation of physicians as one means to improve efficiency.
Expanded services: Add services to PHC centers, such as initial mental health diagnosis and care services.
At the level of human resources departments, recommendations focused on improving the capacity of human resources departments both by recruiting additional officers and by training existing ones on recruitment techniques.
One key suggested strategy to boost recruitment, specifically for expatriate HRH, included offering better support for relocating HRH, such as ensuring appropriate accommodation and reserving places in educational institutions for children. These recommendations emanate from the difficulties experienced by some HRH regarding matters such as the one described in the quote below:
When I first came to Qatar, I went around for schools and I said I’ve got three children, they all just laughed at me and said “well you’ll never get places.” And that’s what happened. It took us 18 months to get all our kids into school. (Health care manager and primary care provider at a semiprivate organization)
Retention Schemes
Interviewees shared experiences in regard to existing retention schemes and offered advice on how they could be strengthened.
Current schemes
Stakeholders described existing retention schemes including a combination of intrinsic and extrinsic rewards. Intrinsic rewards suggested by stakeholders included professional development and continuing medical education (CME) opportunities, promotion and training, and conference participation.
Despite the importance of intrinsic recognition strategies, the majority of retention schemes identified fall under extrinsic rewards. The provision of housing, travel and transportation allowances, and bonuses are well-recognized and prevalent HRH retention strategies.
Present challenges
Stakeholders elaborated on an assortment of challenges that jeopardize employee retention in the PHC sector. Such challenges include lack of clear job description, heavy workloads, skyrocketing cost of living, and lack of a standardized salary scale. Lack of job stability and suboptimal retention strategies were affecting turnover rates, with a stakeholder commenting,
. . . People come and go and come and go. They don’t settle down, and . . . when they find a better offer they leave. (Program director at secondary care institution)
In addition, the shortage of intrinsic rewards and the subjectivity of some HRH performance management systems pose additional strains on the length of HRH employment. One stakeholder reflects on this by stating,
Intrinsic awards are available . . .yet are not supported by adequate budget . . . and programs are not consistent across centers. (Health care manager and primary care provider at primary health care center)
Recommendations
Interviewed stakeholders offered an assortment of suggestions and recommendations that may lead to better employee retention (Table 3). Recommendations included implementing a career ladder that allows for the recognition and growth of HRH based on their performance; providing childcare assistance, maternity and parental leave, and retirement plans; and allowing for continuous professional development through participation in national and international conferences. The importance of professional development for retention is highlighted in the following quote:
If you don’t make an effort to make job professionally satisfying, then you’re definitely going to have some people say, “I’ve been doing this for too long, it’s same old thing, and it’s just become so routine . . . my heart is not in it” . . . . and then you lose people. (Primary care provider, program director, and lecturer at primary health care center and academic institution)
In terms of working conditions, flexible hours and workplace gender equality, as well as improving job security and stability, were highly recommended initiatives.
Furthermore, stakeholders recommended that the management of PHC institutions implement initiatives that would identify current and future HRH needs, oversee activities of CME committees, and conduct “exit interviews” to gather feedback from leaving HRH.
Discussion
Qatar has recently established a profound commitment to boosting the public health of its people through realizing “a comprehensive world-class health care system” with a particular emphasis on PHC.12,16-18 Successful outcomes of this initiative are already being realized with PHCC receiving platinum-level accreditation from Accreditation Canada International, among other manifestations. 19 Local authorities have identified PHC as the optimal solution and HRH as the core component for improved PHC delivery. 17 This study highlighted several existing PHC recruitment and retention practices and delineated additional strategic and operational initiatives for a sustainable supply of HRH and continued PHC performance development. Analyses of stakeholders’ responses revealed that Qatar’s PHC sector currently lacks satisfactory mental health, family planning, and overall screening services. These concerns are well founded with mental illnesses having a prevalence rate of 20% and accounting for 3 out of the 5 factors leading to disability in the country. 20
The need for advanced PHC screening and services is further marked as studies reveal that consanguineous marriages constitute half of all marriages among Qataris. The prevalence of marriage between relatives adds to the country’s need for qualified HRH stationed at PHC centers to provide premarital education on the health implications of marriage between relatives. In addition, proper dietary and weight monitoring care is available in only 5 of PHCC’s health centers, while services assisting smokers to quit are provided in a single center.15,17,21,22 Initiatives to address such shortcomings are underway with ongoing efforts aiming to include mental health as a regular PHC service. Yet, such a strategic expansion of services needs to be well supported by an adequate number of properly trained mental health HRH should the 5-year national mental health strategy be successfully unfolded. 17
One interim solution to address the mental health needs of PHC patients is to train currently employed physicians on caring for mental health issues. Such a measure, while necessary on the short run, is suboptimal taking into consideration the limited role of practitioners in attending to mental health cases and their already busy schedule that prevents them from delivering proper screening services, including mental health. 23 While it is expected that excessive reliance on expatriate human resources will continue for the next few years, it is essential to work on building local training capacity to boost local supply of HRH and ensure that service providers are culturally savvy.
Offering HRH employed in the PHC sector an assortment of intrinsic and extrinsic rewards would enhance recruitment and contribute to prolonged employee tenure. 24 The centrality of these rewards is underscored in existing national strategies; nonetheless, they need to be properly operationalized by provider organizations, such as PHCC. Such a task is daunting taking into consideration that, to satisfy national health objectives, PHCC needs to add 1900 HRH by 2017. In addition, PHCC reports that only 27% of its workforce is Qatari. 17 Therefore, it is imperative for any successful recruitment and retention strategy to consider that the majority of PHC providers are expatriates. Such strategies need to devote attention to the needs and aspirations of expatriate HRH, including offering support with housing, facilitating children schooling requirements, and streamlining the administrative processes so that the relocation and settlement would be possible within a reasonable time frame.
One key reward that was expressed by virtually all public, academic, and parastatal stakeholders was the availability and fairness in the selection of candidates to participate in CME and professional development activities. Access to such opportunities is pivotal because they are a prerequisite for job promotion and career advancement, as well as a requirement to maintain licensure with professional colleges, orders, and syndicates. The outcomes of CME activities may also exceed the organizational level to influence community health outcomes. 25 PHCC, in its national PHC strategy, has committed to continuously advancing and training its HRH. 17
The current study has a number of shortcomings that are worth mentioning. First, the interviewed stakeholders may not be representative of all PHC employers in the state of Qatar. Second, the research team could not ascertain whether the identified interviewees who declined the request for interview held views different from those who accepted to be interviewed. Third, it cannot be confirmed whether the interviewed stakeholders were biased in their responses in fear of disclosure.
Conclusion
Multiple internal and external factors currently influence Qatar’s sustainable supply of PHC professionals. Encouragingly enough, Qatar’s PHC strategy recognizes and commits to addressing the majority of the discussed HRH concerns. The study provided guiding mechanisms to assist PHC decision makers in translating knowledge by implementing recruitment and retention strategies. PHC authorities are advised to approach developments from a consultative, bottom-up approach, with HRH feedback as the initial and main input for improvement. Future investigations would focus on evaluating the impact of implemented strategies and identifying areas for improvement. Studies on specific determinants of HRH retention are also recommended for more targeted efforts.
Footnotes
Acknowledgements
The authors acknowledge the support of Mr Sylvain Touati at Fikra Research and Policy. Deep gratitude is also extended to each of the interviewed stakeholders for their generous sharing of experience and recommendations. The authors also thank Mrs Nariman Chamoun for her editorial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported financially by the Qatar National Research Fund’s (QNRF) National Priorities Research Program (award number NPRP 5-1559-3-314). QNRF requested regular updates regarding progress of research activities and associated outcomes, yet had no say in regard to data collection, analysis, write-up, or publication.