
Abstract
Understanding attitudes toward suicide, especially among healthcare personnel, is an important step in both suicide prevention and treatment. We document the adaptation process and establish the validity and reliability of the Attitudes Toward Suicide (ATTS) questionnaire among 262 healthcare personnel in 2 major public hospitals in the Klang Valley, Malaysia. The findings indicate that healthcare personnel in Malaysia have unique constructs on suicide attitude, compared with the original study on a Western European sample. The adapted Malay ATTS questionnaire demonstrates adequate reliability and validity for use among healthcare personnel in Malaysia.
Introduction
Globally, an estimated 804 000 individuals died by suicide in a year, 1 of which 60% occurred in Asia. 2 Suicide is a rising problem in Malaysia, with a 60% rise in suicide cases during the last 45 years. 3 Suicide is also a significant issue among adolescents, with 12.6% reporting severe suicide ideation. 4 The suicide rate in Malaysia is estimated to be between 1.18 5 and 8 6 per 100 000 population. However, the concern is that these reported rates may be higher due to underreporting and misclassification as undetermined deaths.7,8
In a health care context, approximately half of the individuals who suicided contacted the hospital emergency department at least once within the year of their death, 9 or received health service care within 4 weeks of their death, of which 20% were considered preventable. 10 The number of hospital admissions for suicide attempts in Malaysia is increasing. 11 Meanwhile, one-fifth of suicide deaths occurred in Malaysian hospitals. 4 However, a systematic review revealed that general hospital personnel, in the United Kingdom, the United States, and Australia, held negative attitudes toward suicidal patients. 12 Meanwhile, other studies, including a worldwide systematic review from the patients’ perspective, indicated a perception that healthcare personnel were nonempathetic and exhibited stigmatizing behavior.13,14 This could hinder help-seeking behavior among at-risk suicidal individuals. 15 Considering the importance of suicide prevention and management in a health care setting,16,17 and because suicide attitude is influenced by culture,18,19 it is crucial to adapt and validate a Malaysian suicide attitude questionnaire.
A literature search was conducted to determine the most suitable questionnaire for cross-cultural adaptation and validation in Malaysia (see the “Methods” section for the description of the Attitudes Toward Suicide [ATTS] questionnaire). This study adopted the ATTS questionnaire, as it was considered a valid and feasible instrument during a systematic review by Kodaka et al, 20 was built on existing questionnaires,21-23 and informed by expert knowledge in this field. 24 Furthermore, it was employed in the health care setting25-28 and the Asian context.29-34
The aim of this study was to translate, adapt, and assess the validity and reliability of the ATTS questionnaire for use among healthcare personnel in a Malaysian context.
Methods
Study Design
This is a cross-sectional study of healthcare personnel, from 2 major public hospitals in Malaysia, to establish the validity and reliability of the Malay ATTS.
Phase I: Translation and Cross-Cultural Adaptation Process
The ATTS questionnaire was developed by Salander Renberg and Jacobsson, 24 who aimed to build a feasible instrument that enabled a large-scale measurement of attitudes toward suicide. The second version of the ATTS questionnaire is composed of 37 items, scored on a 5-point Likert scale incorporating “Strongly Disagree,” “Disagree,” “Undecided,” “Agree,” and “Strongly Agree.” The responses were coded as “Strongly Disagree” = 1 to “Strongly Agree” = 5, except for items 4 and 6, which were reverse coded. An exploratory factor analysis revealed 10 interpretable factors as Suicide as a right; Incomprehensibility; Noncommunication; Preventability; Tabooing; Normal/common; Suicidal process; Relation-caused; Preparedness to prevent; and Resignation. Higher scores indicated agreement with the factor or domain. The α coefficients ranged from 0.38 to 0.86.
The English ATTS questionnaire was forward- and backward-translated from English to Malay independently by subject-matter and linguistic experts. The subject-matter experts were a public health specialist (forward translation) and a psychiatrist (backward translation). To ensure content validity, a harmonization meeting was held to combine the 2 versions of the translated questionnaire, comprising of a multidisciplinary team of psychiatric, psychological, behavioral science, public health, and linguistic experts. The adaptation process took into account factors of barriers in linguistics comprehension, contextualized meaning attached to a construct, and possible interpretations of the translated instrument. 35
Two pilot studies were conducted on the translated instrument. Through a convenience sampling from 2 public hospitals, the authors recruited 51 and 49 healthcare personnel for each pilot study, respectively. After reviewing the results of the first pilot study, improvements were made to items with low corrected item-total correlation, which contributed to the low total Cronbach’s α. A second pilot study was implemented to test the improved questionnaire, and, compared with the first version of the translated questionnaire, yielded a higher total Cronbach’s α of 0.53. The Malay ATTS questionnaire was finalized for further validation with a larger sample.
Phase II: Validation Process
Participants
To validate a questionnaire, between 2 and 20 participants per item are needed,36,37 with a minimum of 250 participants. 38 In this study, assuming that 8 participants are needed per item, with a drop-out rate of 10%, 325 participants were targeted for recruitment.
For inclusion criteria, the following core medical and surgical departments were selected: general medical, general surgery, accident and emergency, obstetrics and gynecology, pediatrics, orthopedics, and psychiatry. Doctors, nurses, assistant medical officers, and medical attendant professions were included. All participants were Malaysians, but trainees were excluded from the study.
Procedures
Participants were randomly sampled based on the sampling frame with the names of all staff from the related professions and departments. Participation was voluntary, and strict confidentiality was maintained with no identifier being used in the questionnaires. After giving informed consent, participants filled out the questionnaire, consisting of the Malay ATTS and demographic information, such as age, gender, race, religion, marital status, occupation, education, department, years of service, number of suicidal patients cared for, and training in the management of suicidal patients. The participants returned the questionnaires within a week, sealed in an envelope.
Statistical analyses
Statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS; version 23) and the Analysis of Model Structures (AMOS; version 20). Confirmatory factor analyses, involving principal components analysis (PCA) extraction and promax rotation, were used to assess the construct validity of the Malay ATTS questionnaire. Ten- and 11-factor models were tested based on the findings of past validation studies.24,29 Items with a <0.40 factor loading were excluded from further analysis.
Model fit indices were employed in a confirmatory factor analysis. This included chi-square-value/degree of freedom (χ2/df < 2.00), 39 normed fit index (NFI ≥ 0.95), 40 Tucker-Lewis index (TLI ≥ 0.95), 40 parsimonious normed fit index (PNFI ≥ 0.50), 41 root mean square error of approximation (RMSEA < 0.05), 42 and test of RMSEA significance (PCLOSE ≥ 0.05).
Cronbach’s α (≥0.70)43,44 was employed to assess the overall internal consistency of the scale and its subscales. Items that contributed to low α coefficients were excluded from further analysis.
Approvals
This research obtained ethical approval from the Medical Research and Ethics Committee, Ministry of Health Malaysia (NMRR-14-1805-22032) and the Research Ethics Committee, National University of Malaysia (NN-035-2015). The authors complied with the required ethical standards (see Figure 1). 45

Workflow of the translation, cross-cultural adaptation, and validation process of the English ATTS to the adapted Malay ATTS.
Results
Participant Characteristics
There were 325 randomly selected participants. The final sample size for this validation was 262 participants (80.6%), with 26 (8.0%) dropouts and 37 (11.4%) excluded listwise due to missing data. The researchers did not rectify incomplete samples, due to confidentiality and the absence of identifiers in the responses. Participants’ demographics are listed in Table 1.
Characteristics of Healthcare personnel in the Study (n = 262).
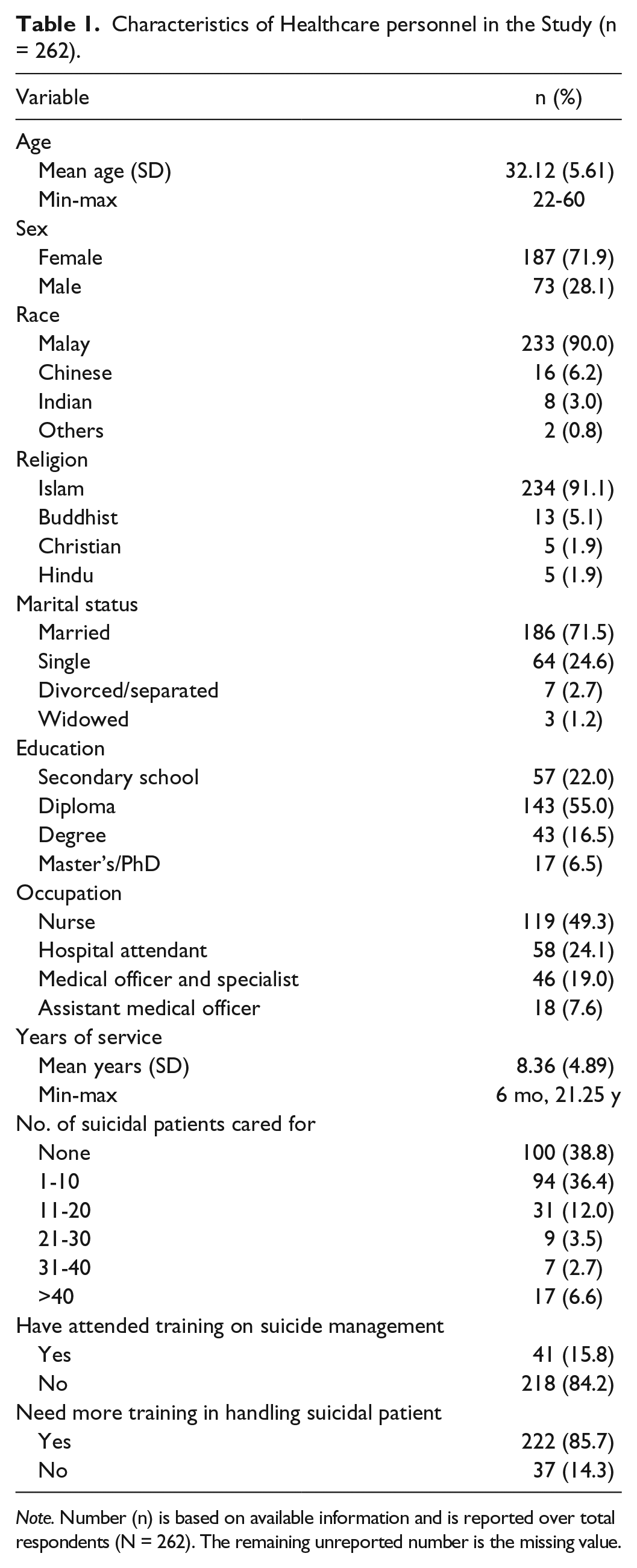
Note. Number (n) is based on available information and is reported over total respondents (N = 262). The remaining unreported number is the missing value.
Validity Analysis
The minimum amount of data required for factor analysis was met, with more than 7 cases per questionnaire item. Factorization, through the use of PCA using promax rotation, revealed an acceptable Kaiser-Meyer-Olkin measure of sampling adequacy (KMO = 0.73), which is above the recommended value of 0.60. Bartlett’s test of sphericity was significant, χ2(666) = 2210.97, P < .001. The diagonals of the anti-image correlation matrix of all items were above 0.50, thus supporting the inclusion of each item in the factor analysis. In addition, the communalities for all items were above 0.40 (see Table 2), suggesting reasonable factorability. Given these overall indicators, factor analysis was performed on all 37 items of the Malay ATTS questionnaire.
Explained Variance, Factor Loadings, and Communalities Based on a Principal Components Analysis With Promax Rotation for 30 Items From the Adapted Malay ATTS Questionnaire (n = 262).

Note. ATTS = Attitudes Toward Suicide.
PCA examined the solutions for 10 and 11 factors using promax rotation. The initial 11-factor solution was preferred, as it explained a higher percentage of cumulative variance (57.55%) compared with the 10-factor solution (54.63%), and more items with insufficient primary loadings (>0.40) were found for the 10-factor solution.
PCA was conducted again on the 11-factor solution using promax rotation after eliminating 7 items from further analysis due to (1) primary factor loadings of less than 0.40 (items 24, 30, and 37) and (2) contribution to low α coefficient in the subfactors (items 4, 6, 22, and 35). The results revealed that the 11 factors explained 63.24% of the variance. All items had primary loadings above 0.40 (see Table 2).
Confirmatory factor analysis was performed to test the model fit for the 11-factor solution, and compare it with the 10-factor solution. The results demonstrate that both models met the fit values with a χ2/df ratio (1.79 and 1.58, respectively) and PCLOSE (0.39; 0.92) indices. The 11-factor model also demonstrated a goodness-of-fit according to the RMSEA (0.04) and PNFI (0.53) indices. However, it failed to meet the cutoff values required for NFI and TLI indices (see Table 3).
Goodness-of-Fit Indicators for the 10- and 11-Factor Solutions for the 30-Item Adapted Malay ATTS (n = 262).

Note. ATTS = Attitudes Toward Suicide; NFI = normed fit index; TLI = Tucker-Lewis index; PNFI = parsimonious normed fit index; RMSEA = root mean square error of approximation; CI = confidence interval.
p < .001.
Reliability Analysis
The Cronbach’s α for the domains ranged from 0.32 to 0.76. The overall Cronbach’s α for the adapted Malay ATTS questionnaire was 0.72 (see Table 4), thus indicating that these items measured the same construct or content. 46 Descriptive analysis of the questionnaire’s items and factors is shown in Table 4. The least endorsed item was “People do have the right to take their own lives,” while the most endorsed item was “It is a human duty to try to stop someone from committing suicide.” Items 7, 10, 11, 12, 15, 23, 32, and 33 had more than 20% of the respondents choosing the “Undecided” option.
Descriptive Statistics for the 11 Adapted Malay ATTS Factors (n = 262).
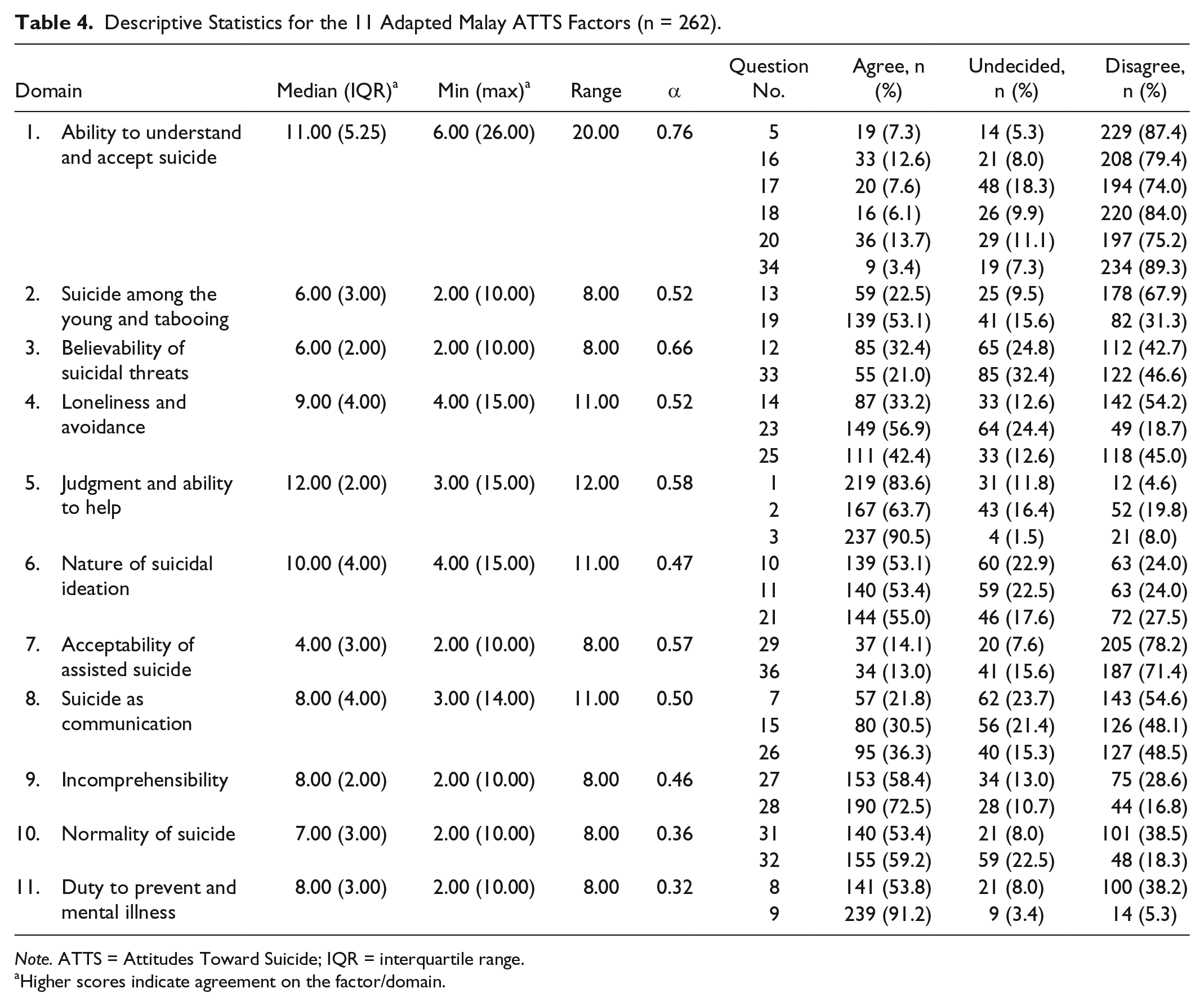
Note. ATTS = Attitudes Toward Suicide; IQR = interquartile range.
Higher scores indicate agreement on the factor/domain.
Discussion
The study findings demonstrate that healthcare personnel may have different categorical constructs on suicide compared with previously tested populations.24,29,33,47 It also sets a milestone in the development of a suicide attitude questionnaire in Malaysia.
In terms of its validity, the item loadings of the adapted 11-factor Malay ATTS questionnaire varied widely from previous studies. Constructs in the adapted Malay ATTS questionnaire suggest a distinctive health care viewpoint on suicide attitude, when compared with studies tested on a Western European general population, 24 and college students in Asia 29,33 and Uganda. 47 For example, the items “People who make suicidal threats seldom complete suicide” and “Those who talk about suicide will not do it” were grouped under the “Common/Normal” factor in the original ATTS questionnaire, but emerged as a distinctive factor in the adapted Malay ATTS questionnaire under “Believability of Suicide Threats.” This may reflect on the experience and decisions that healthcare personnel need to undertake when encountering suicidal patients, compared with the general population. The factors “Acceptability of Assisted Suicide,” “The Nature of Suicidal Ideation,” and “Duty to Prevent and Mental Illness” also emerged to indicate issues that surround the health care establishment.
Cultural and religious differences may contribute to the factor loading patterns of the adapted Malay ATTS questionnaire items. The factor “Loneliness and Avoidance” may be indicative of isolation and the taboo surrounding suicide in Malaysia, especially among Muslims,33,34 who comprised the majority of respondents. The factor “Ability to Understand and Accept Suicide” in the adapted Malay ATTS questionnaire merged items from the “Resignation” and “Right to Suicide” factors in the original ATTS questionnaire. This may indicate that those who disagreed with the right to suicide could also be less understanding toward suicidal patients’ reasons for wanting to die. Further explorations into the right-to-die issue are important, as healthcare personnel who expressed a permissive right-to-die attitude reported less competency in suicide-related interventions 48 and were associated with personal factors, such as suicide ideation history 25 and lower/nonendorsement of a religious belief.49,50
Confirmatory factor analysis yielded mixed findings, where requirements for absolute fit indices, such as χ2/df, RMSEA, and PCLOSE, were met, but the cutoff values recommended for relative fit indices, such as TLI and NFI, were not. This may be due to the relatively large number of variables 51 resulting in poor fit values. The multidimensional nature of suicide attitudes 24 may also contribute to this.
In terms of reliability analysis, the adapted questionnaire demonstrated an acceptable overall Cronbach’s α of more than 0.70, thus indicating the internal reliability of the instrument. When compared with Salander Renberg and Jacobsson 24 and Ji et al, 29 the Cronbach’s α value was slightly higher. However, there was a large variation in the internal consistency of factors, ranging from 0.32 to 0.76. This variation also surfaced in other suicide attitude instruments (e.g., α coefficient range of 0.26-0.83 in Domino et al, 52 0.48-0.85 in Rogers and DeShon, 53 0.38-0.86 in Salander Renberg and Jacobsson, 24 0.57-0.74 in Xiang et al, 33 and 0.31-0.78 in Ji et al 29 ), suggesting that attitude toward suicide could be a highly sensitive issue resulting in conflicting and varied responses from participants, 24 especially in a cultural setting where suicide is stigmatized. 47
Finally, analysis of response proportions to each item revealed that 8 items consisted of at least one-fifth of the participants choosing the “Undecided” option. Response fatigue, or low motivation, could be ruled out as the reason, because the position of these items ranged from the beginning, middle, and end of the questionnaire. 54 Perhaps healthcare personnel in this study felt a lack of knowledge or information to assess the believability level of a suicidal patient’s communication (items 12 and 33) and the private nature of suicidal thoughts (items 7, 10, 11, and 15), and experienced a conflict between sympathizing with a terminally ill patient’s wish to die and disagreement with the right to die (item 32), or were ambivalent about suicide as a taboo topic for discussion (item 23).
Strengths and Limitations
As the first study in Malaysia to cross-culturally adapt and validate a suicide attitude questionnaire, this study demonstrated methodological vigor by employing random sampling to ensure representativeness of the data. Participants’ heterogeneity was also achieved, as is attested by the participants’ age range, department, occupation, and experience in the health care sector and in handling suicidal patients. As for its limitations, the drop-out rate and missing data could have contributed to the response bias, which was not examined. Nearly half of the respondents were inexperienced in managing suicidal patients; therefore, their attitudes may not be shaped by concrete encounters with suicidal individuals. However, we still consider their responses to be valid, as attitudes could constitute preconceived ideas, which may or may not be modified by experience. This study focused on healthcare personnel from 2 general hospitals, while providers from community and private settings were not represented. Future studies employing different settings and target groups are needed to further explore and improve the psychometric rigor of the adapted Malay ATTS questionnaire, so that comparisons can be made.
Conclusion
The adapted Malay ATTS questionnaire demonstrated adequate psychometric properties for use among healthcare personnel in Malaysia. Underlying factors that are distinctive to healthcare personnel were revealed, thus indicating the questionnaire’s suitability for administration to this population.
Footnotes
Acknowledgements
The authors wish to convey their gratitude to the Director General of the Ministry of Health Malaysia for permission to publish this article, and the director, heads of departments, and staff of the UKM Medical Centre and Putrajaya Hospital. In addition, we would like to thank Dr Ellinor Salander Renberg (Umeå University, Sweden) for permission to use the Attitudes Toward Suicide (ATTS) and for clarifications given during the translation process, and Ms Lee Shoo Thien, a statistician, for statistical advice.
Author Contributions
LHW proposed the study to be carried out. CSS conducted the data collection and undertook the statistical analyses. CSS and LHW wrote the first draft of the manuscript with advice from a statistician. All authors edited, contributed to, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research University Grant, National University of Malaysia (Grant No.: GUP-2014-065).