
Abstract
The term “palliative care” has a negative connotation and may act as a barrier to early patient referrals. Rebranding has thus been proposed as a strategy to reduce the negative perceptions associated with palliative care. For example, using the term “supportive care” instead of “palliative care” in naming palliative care units has been proposed in several studies. In Taiwan, terms other than “palliative” and “hospice” are already widely used in the names of palliative care units. With this in mind, this study investigated the characteristics of palliative care unit names in order to better understand the role of naming in palliative care. Relevant data were collected from the Taiwan Academy of Hospice Palliative Medicine, the National Health Insurance Administration of the Ministry of Health and Welfare, and the open database maintained by the government of Taiwan. We found a clear phenomenon of avoiding use of the terms “palliative” and “hospice” in the naming of palliative care units, a phenomenon that reflects the stigma attached to the terms “palliative” and “hospice” in Taiwan. At the time of the study (September, 2016), there were 55 palliative care units in Taiwan. Only 20.0% (n = 11) of the palliative care unit names included the term “palliative,” while 25.2% (n = 14) included the term “hospice.” Religiously affiliated hospitals were less likely to use the terms “palliative” and “hospice” (χ2 = 11.461, P = .001). There was also a lower prevalence of use of the terms “palliative” and “hospice” for naming palliative care units in private hospitals than in public hospitals (χ2 = 4.61, P = .032). This finding highlights the strong stigma attached to the terms “palliative” and “hospice” in Taiwan. It is hypothesized that sociocultural and religious factors may partially account for this phenomenon.
Introduction
The World Health Organization (WHO) defines “palliative care” as an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, including physical, psychosocial, and spiritual problems. 1 Most cancer patients, for example, experience multiple forms of physical and psychological distress at all stages of their illness, with cancer-related symptoms significantly impacting their daily activity and quality of life. 2 According to the WHO, palliative care is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications. 1 Multiple studies have shown that integrating palliative care early in the disease trajectory improves symptom control, quality of life, patient and caregiver satisfaction, end-of-life care, costs of care, and, potentially, survival.3-7 Despite the increased use of palliative care, however, most patients only receive the service late in the disease trajectory or not at all.8-11 Prior research has suggested that the term “palliative care” itself might be a deterrent to early referrals and that the term “supportive care” may be more favorable for some hospital-based palliative care programs.12-14 The term “palliative care” carries a stigma for physicians, patients, and their caregivers, who regard it as synonymous with death and dying, loss of control, hopelessness, and abandonment. “Supportive care,” in contrast, has been regarded as a more favorable term.15,16 According to previous studies, the term “supportive care” is associated with better understanding, more favorable impressions, higher future perceived need, and earlier referrals.16-19
In Taiwan, palliative care services include inpatient care, home care, and outpatient services. The National Health Insurance (NHI) program reimburses the cost to service providers of home care, outpatient services, inpatient care, and shared care, a service for patients in nonhospice wards. The NHI program was established in 1995 to provide health care to all residents in Taiwan. Currently, 99.9% of Taiwan’s population is covered by the NHI program. It is a government-administered insurance-based national health care system. As of September 2016, there were 55 palliative care units, 141 inpatient consultation teams, 93 home care teams, and 155 community service teams in Taiwan. 20 In Taiwan, palliative care is defined as specialized medical care that focuses on providing patients relief from pain and other distressing symptoms of a serious illness, regardless of the diagnosis or stage of disease. The palliative care units defined in this study are palliative care wards in hospitals. Actually, all the palliative care units in Taiwan are hospital-based inpatient units. Hospice care is difference from palliative care. Hospice care focuses on supportive care to people in the final phase of a terminal illness. In Taiwan, there are no residential facilities to provide hospice care. Hospice care is provided in the settings of hospital-based inpatient care, outpatient services, and home care. Although inpatient palliative care services in Taiwan have increased from 1 ward in 1990 to 55 palliative care units with more than 756 beds in 2016, the term “palliative care” itself is not commonly used in palliative care units. This study is the first to examine the naming patterns of palliative care units from a nationwide prospective. In this study, nationwide data on palliative care units in Taiwan were collected and analyzed to examine (1) the naming pattern used in the naming of palliative care units; (2) the associations, if any, between the names of palliative care units, the numbers of beds, the levels of medical facilities, and the population sizes and degrees of urbanization in the areas served by different units; and (3) the common themes for naming palliative care units.
Material and Methods
Data Collection
The nationwide data were collected from the Taiwan Academy of Hospice Palliative Medicine, the National Health Insurance Administration of the Ministry of Health and Welfare, and the open database maintained by the government of Taiwan (http://data.gov.tw/). The services provided by the palliative care units in Taiwan are covered by the National Health Insurance. Therefore, the database from the National Health Insurance Administration of the Ministry of Health and Welfare included all the information of palliative care units in Taiwan. These data included the names of palliative care units, and the variables analyzed included the level of medical facilities, the number of beds in each palliative care unit, and the degree of urbanization and the population of the area served by each unit. The degree of urbanization was defined using the categorizing methods of Liu et al, which divide the degree of urbanization into 7 types, namely, highly urbanized towns, medium urbanized towns, emerging towns, general towns and cities, aging towns, agricultural towns, and remote towns. 21
Statistical Analysis
The data were analyzed using the statistical software SPSS version 22.0 (IBM Corp, Armonk, New York). The samples were separated into 3 groups (with 2 groups made up of unit names that included either “hospice” or “palliative,” and a third group made up of unit names that included neither of those 2 terms). Descriptive statistics were used to summarize the names of the palliative care units, the level of medical facilities, the number of beds in each palliative care unit, and the degree of urbanization and the population of the area served by each unit. An analysis of variance F test was conducted to compare the number of beds in each unit and the population served by each unit for the 3 aforementioned groups. A chi-square test of independence was performed to compare the level of medical facilities for the 3 groups. A Fisher’s exact test was used to evaluate only the highly urbanized towns and medium urbanized towns against the type of name, because of the small numbers of palliative care units in emerging towns, general towns and cities, aging towns, agricultural towns, remote towns, and outlying islands. A P value < .05 (2-tailed) was considered statistically significant.
Qualitative Analysis
The first part of the analysis consisted of enumerating the words used in the different units’ names. Second, using the approach of thematic analysis, the words were grouped in terms of their denotative and connotative meanings to capture the key themes. Denotative meanings are what a word literally refers to, and connotative meanings are the associations, values, and judgments that surround this. 22 The frequencies of occurrence for each category were calculated to derive the dominant concepts. This study was approved by the institutional review board of Taipei Veterans General Hospital according to Republic of China law.
Results
Characteristics of Study Samples
At the time of the study (September, 2016), there were 55 palliative care units in Taiwan. Among the hospitals having palliative care units, 38.2% (n = 21) were public and 61.8% (n = 34) were private. Religiously affiliated hospitals accounted for 27.3% (n = 15) of all the hospitals, including 4 Buddhist hospitals, 5 Catholic hospitals, and 6 Christian hospitals. The basic characteristics of the palliative care units are summarized in Table 1. Only 20.0% (n = 11) of the palliative care unit names included the term “palliative,” while 25.2% (n = 14) included the term “hospice.” One palliative care unit used both “palliative” and “hospice” in its name. It is noted that although the term “hospice” is used, the units with “hospice” in their names are actually palliative care wards. Finally, neither “palliative” nor “hospice” was used in more than half of the palliative care unit names (56.4%, n = 31).
The Characteristics of Palliative Care Units in Taiwan.
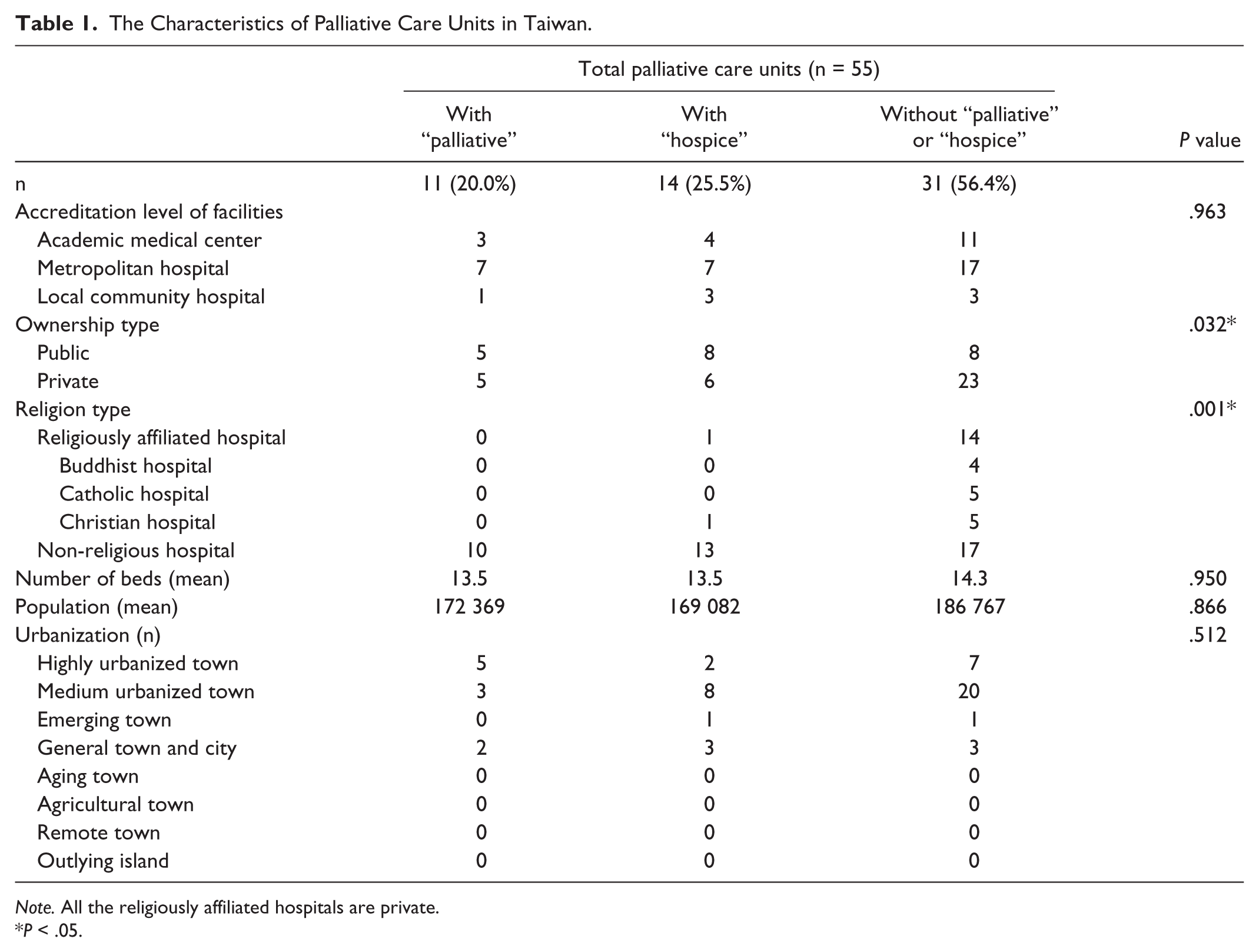
Note. All the religiously affiliated hospitals are private.
P < .05.
Bivariate Correlations
Table 1 shows the bivariate analyses of the level of medical facilities, the number of beds in each palliative care unit, the degree of urbanization, and the population size, along with possible associates. A tendency toward avoiding the terms “palliative” and “hospice” was found in religiously affiliated hospitals (χ2 = 11.461, P = .001). There was also a lower prevalence of use of the terms “palliative” and “hospice” for naming palliative care units in private hospitals than in public hospitals (χ2 = 4.61, P = .032). In terms of the levels of medical facilities, the numbers of beds in the palliative care units, the population sizes, and the urbanization levels, there was no statistically significant association with use of the term “palliative” or “hospice” in palliative care unit names.
Qualitative Analysis of Clinic Names
Among the palliative care units that did not use “palliative” or “hospice” in their names, 22.6% (n = 7) used people’s names in their names, for example, “Saint Francis home.” Apart from people’s names, Table 2 lists the frequency with which certain words occurred in those unit names not including the terms “palliative” or “hospice.” The most frequently occurring word was 心 (xin), which means “mind” or “heart” in Chinese. The second most frequently occurring words were 愛 (ai), meaning “love,” and蓮 (lian), meaning “lotus.” The third most frequently occurring words were 聖 (sheng), meaning “saint”; 恩 (en), meaning “grace”; 寧 (ning), meaning “peace”; and 德 (de), meaning “virtue.” Three themes were identified from the words used in the palliative care unit names, as shown in Table 3. The first theme, which we have called kindness and love, accounted for 6 occurrences. The second theme was described as religion and accounted for 5 occurrences. The third theme was peace and accounted for 4 occurrences.
Frequencies of Specific Words in the Names of Palliative Care Units Not Including “Palliative” or “Hospice.”.

Superordinate Categories of the Words Used for Clinics Names.

Discussion
This study is the first systematic analysis of nationwide data regarding the naming of palliative care units. In this study, we found that the terms “palliative” and “hospice” tend to be avoided in naming palliative care units. Instead, words reflecting the themes of “kindness and love,” “peace,” and “religion” were frequently used. This finding suggests the hypothesis that less stigmatizing names were used to generate more positive impressions, higher perceived need, and more referrals.
The stigma attached to palliative care is known to be associated with death, hopelessness, dependency, and end-of-life care.12-14 Erving Goffman, a sociologist, defined stigma in terms of undesirable and deeply discrediting attributes that disqualify one from full social acceptance and motivate efforts by the stigmatized individual to hide the mark when possible. 23 Link and Phelan proposed that stigma exists when elements of labeling, stereotyping, separating, status loss, and discrimination co-occur in a power situation that allows these processes to unfold. 24 Previous studies suggested that the term “palliative care” evoked more negative perceptions in physicians, patients, and their caregivers, compared with the term “supportive care.” It is associated with death, hopelessness, dependency, and end-of-life care for inpatients.13,14 Prior research suggests that stereotypical images of palliative care among patients and their caregivers were derived in large part from their interactions with the medical system, with patients stating that their health care providers delayed referral to palliative care and equated it with end-of-life care.14,15 Many oncologists delay referral to palliative care until all disease-modifying treatments have been exhausted.8-11 Oncologists are gatekeepers of palliative care referral and, therefore, are of paramount importance in improving the integration of palliative care services. The decision to refer to palliative care is a highly complex process, and assessing the timing of referral is not straightforward.25,26 It depends on national and regional health care policies, local resources, the comprehensiveness of the palliative care teams, patient characteristics, and the level of palliative care provided by primary care teams. 27 There are various factors that can impede the referral process. Negative attitudes toward palliative care are one of the most frequently cited barriers to palliative care access. 28 In this study, the finding of avoiding use of the terms “palliative” and “hospice” in the naming of palliative care units reflected the negative attitudes toward palliative care and hospice. Rebranding palliative care has been proposed as a strategy to reduce the negative perceptions associated with palliative care.16-19 The finding of this study suggests the hypothesis that words other than “palliative” or “hospice” are used might be to reduce the negative perceptions of palliative care and enhance patients’ acceptance of admission to these units or of oncologists’ referral of patients to these units. This finding also suggests several possible directions for future research, such as research into the degree of patients’ understanding of the informed consent process when they are being admitted to palliative care units. In this study, avoiding use of the terms “palliative” and “hospice” reflects the stigma associated with palliative care, which relates to a larger societal attitude toward death. 29 In a cross-cultural study, 70% of the Taiwanese physicians reported that they often or very often experienced families as being reluctant to discuss end-of-life issues, while the corresponding figures were 50% in Japan and 59% in Korea. 30 Reluctance to participate in end-of-life discussions is common all over the world, especially in Asia. The most hypothesized interpretation is that Confucianism does not systemically refer to life after death, and death has been a taboo for long periods. 31 The beliefs about Taoism, Confucianism, and Buddhism have influenced Chinese people for thousands of years, particularly in relation to death and dying. 32 In Taiwan, 35% of the population is composed of Buddhists, 33% of Taoists, 3.9% of Christians, and 18.7% of people who identify as not religious. 33 In this study, 14 of the 15 religiously affiliated hospitals did not use “palliative” or “hospice” in the name of their palliative care units. Prior research showed that culture and religious beliefs affect one’s perception of palliative care and the decision making that occurs at end of life.34-36 However, future research is needed to further understand the role of religious beliefs in attitudes toward palliative care in Taiwan.
This study has several limitations. First, while we found the phenomenon of avoiding use of the terms “palliative” and “hospice” in the naming of palliative care units, the determinants of choosing names for palliative care units are still unclear. The choice of names may rest with stakeholders other than oncologists and palliative care providers (eg, key administrators, funders). Second, this study only shows that the terms “palliative” and “hospice” are avoided in the names of palliative care units, but it is not able to directly reflect the perceptions of patients and palliative care providers. Third, the study was conducted in Taiwan. The findings in this study thus may not generalize to other countries with different cultures and languages. Finally, the effects of palliative care unit naming on perceived stigma and perceived service need among patients were not clarified due to a lack of related data. Further study is thus needed to further evaluate the effects of palliative care unit names on attitudes toward palliative care among both physicians and patients.
Conclusion
The findings of this study offer novel insights into our understanding of the stigmatization and elements of labeling associated with palliative care. There is a strong stigma attached to the terms “palliative” and “hospice” in Taiwan. The tendency toward avoiding use of the terms “palliative” and “hospice” in the names of palliative care units is especially significant among private hospitals and religiously affiliated hospitals. Sociocultural and religious factors are hypothesized to partially account for this phenomenon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.