
Abstract
Understanding how new Medicaid enrollees are approaching their own health and health care in the shifting health care landscape of the Affordable Care Act has implications for future outreach and enrollment efforts, as well as service planning for this population. The objective of this study was to explore the health care experiences and expectations of new Medicaid expansion beneficiaries in the immediate post-enrollment period. We conducted semistructured, qualitative interviews with a random sample of 40 adults in Philadelphia who had completed an application for Medicaid through a comprehensive benefits organization after January 1, 2015, when the Medicaid expansion in Pennsylvania took effect. We conducted an inductive, applied thematic analysis of interview transcripts. The new Medicaid beneficiaries described especially high levels of pent-up demand for care. Dental care was a far more pressing and motivating concern than medical care. Preventive services were also frequently mentioned. Participants anticipated that insurance would reduce both stress and financial strain and improve their experience in the health care system by raising their social standing. Participants highly valued the support of telephone application counselors in the Medicaid enrollment process to overcome bureaucratic obstacles they had encountered in the past. Dental care and preventive services appear to be high priorities for new Medicaid enrollees. Telephone outreach and enrollment support services can be an effective way to overcome past experiences with administrative barriers.
Introduction
As of June 2016, more than 9.4 million low-income adults had gained insurance coverage through the Medicaid expansion as part of the Affordable Care Act (ACA). 1 The 32 states participating in the Medicaid expansion have seen large reductions in their rates of uninsured residents.2,3 The Medicaid expansion and other ACA coverage provisions have resulted in the lowest national uninsured rate (9.0%) since 1972, when the Centers for Disease Control and Prevention began reporting on the country’s uninsured population. 4
Health insurance serves two key roles—protecting against the financial effects of illness and facilitating health service access. Although gaining insurance coverage provides some immediate financial protection, it is just a step toward securing access to health care. In states that expanded Medicaid early, like Oregon, many new beneficiaries described confusion, including questions regarding services covered and associated costs. 5 In Massachusetts, new Medicaid beneficiaries were more likely than privately insured individuals to report barriers to care. 6 Medicaid officials in other states, early in their expansions, also described the challenge of predicting patients’ needs, service utilization, and associated costs, creating difficulties in program planning and implementation. 7 For Medicaid expansion to both expand coverage and improve health, it will be necessary to enroll more of the uninsured population, reenroll current beneficiaries, and help beneficiaries navigate their benefits and the health care system.
We explored the perspectives of new Medicaid expansion beneficiaries who had enrollment assistance in Philadelphia in the immediate post-enrollment period, using in-depth interviews. Our objective was to understand their motivations for obtaining coverage, perceived health and health care needs, and early experiences navigating the health care system at a time of rapid health system change.
Methods
Study Setting
Pennsylvania received approval to expand its Medicaid program in August 2014 under a Section 1115 demonstration waiver from the Centers for Medicare and Medicaid Services, allowing the state to offer new private managed care plans as an alternative to an expansion of the existing Medicaid program. Following the election of Governor Tom Wolf in November 2014, the state changed course and transitioned to an expansion of the traditional Medicaid program in which citizens with household incomes up to 133% of the federal poverty level became Medicaid-eligible. With this change, comprehensive dental benefits were included in all Medicaid plans; prior coverage of dental services varied by plan.
Participant Recruitment
We recruited 40 recent Medicaid enrollees in Philadelphia to participate in semistructured qualitative interviews between March and July 2015. We identified our sample through Benefits Data Trust (BDT), an organization that assists low-socioeconomic status (SES) adults applying for public benefits, including health insurance. BDT identifies individuals who are likely eligible for but are not currently enrolled in public benefit programs (eg, Medicaid), and conducts mail-based outreach, telephone eligibility screening, and enrollment assistance.
For this study, we recruited a random sample of individuals who had contacted BDT for assistance and completed an application for Pennsylvania’s Medicaid program after January 1, 2015, when the expansion took effect. We included English-speaking adults, ages 19 to 64 years. BDT staff contacted individuals by phone inviting them to participate in the study. The research team then contacted those who agreed to participate for phone interviews and obtained informed consent. Participants were remunerated with a $15 gift card.
Interviews and Data Collection
Researchers trained in qualitative interviewing (J.K.H., C.S., J.Z.) conducted the study interviews, which lasted approximately 30 minutes. Motivated by Andersen’s Behavioral Model of Health Services Use and applying it to new Medicaid enrollees, we focused our interviews on participants’ past experiences accessing and utilizing health care and health insurance, as well as how they anticipate utilizing health care in the future. 8 The Andersen model describes the contribution of predisposing factors (aspects of social environment related to health, beliefs about health and health services), enabling factors (self efficacy to access care, availability of facilities, and availability and use of health insurance), and need-based factors (perceived and evaluated) on the subsequent use of health care services. The interview guide included prompts that investigated these important domains from the Andersen model and further probed how gaining coverage might influence each of them. Our interview guide was further developed from a review of the literature and revised through the collective input of the study team, incorporating participant input from 5 pilot interviews.9,10
Analysis
Interviews were audio recorded and professionally transcribed. An inductive, applied thematic analysis was conducted, and themes were analyzed using the qualitative software NVivo, version 10.0. 11 We used a concurrent, iterative process of collecting, coding, and interpreting interview transcripts.12-14 One quarter of interviews were independently coded by 2 researchers (J.K.H., C.S.) with high interrater reliability (mean κ = 0.9). Resultant codes were organized into thematic categories, which were discussed by the team to refine data interpretation. Major themes were not selected a priori but identified by the research team via consensus after reviewing all transcripts and memos.
This study was approved by the University of Pennsylvania Institutional Review Board.
Results
BDT provided the study team with contact information of 80 individuals: 3 did not meet inclusion criteria, 17 could not be reached, and 11 subsequently declined. We reached thematic saturation before attempting to contact the remaining 9 individuals. Of those we called and reached, 78% (40 of 51) agreed to participate in the study. Participants were predominantly African American, unmarried, and unemployed, and approximately evenly distributed with regard to age and gender (Table 1).
Demographics of Study Participants and All Benefits Organization Applicants.
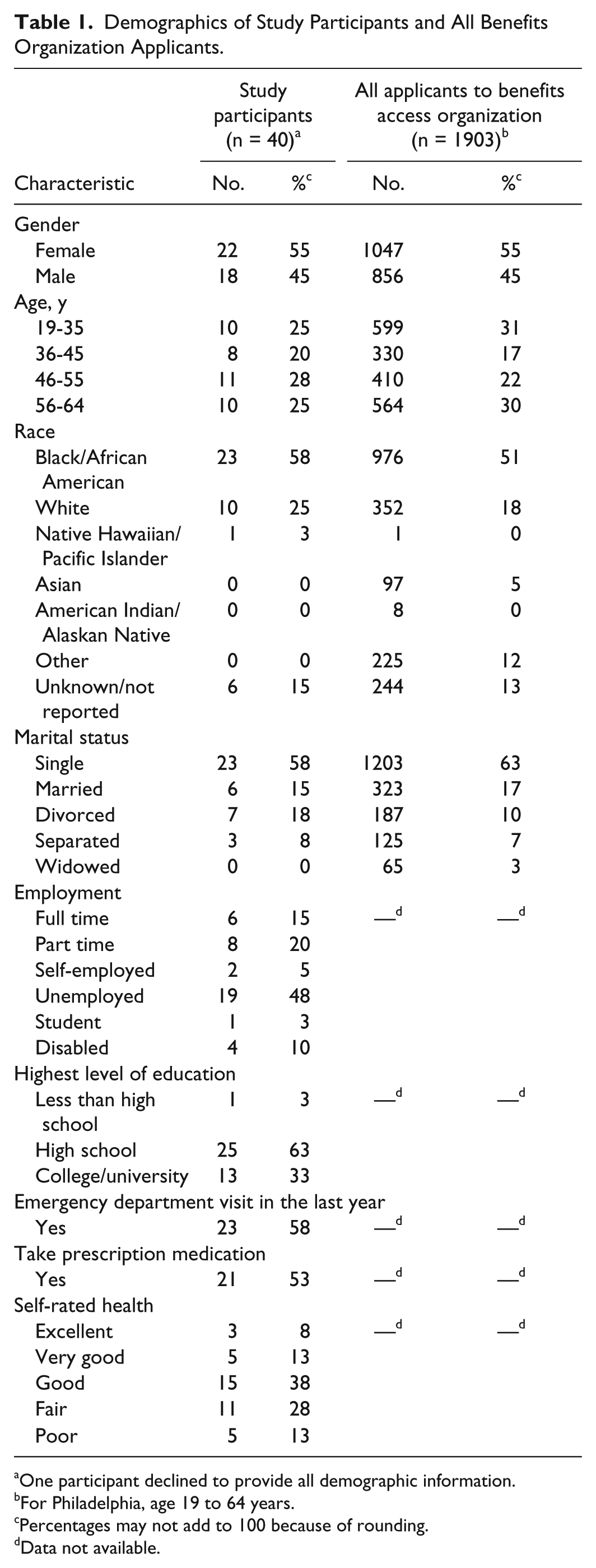
One participant declined to provide all demographic information.
For Philadelphia, age 19 to 64 years.
Percentages may not add to 100 because of rounding.
Data not available.
Four unique themes emerged, each reflecting domains of the Andersen model regarding participants’ approaches to their health and health care following Pennsylvania’s Medicaid expansion. First, participants expressed a clear sense of their perceived health care needs including a high level of pent-up demand for dental services and preventive care. Second, new insurance is a potent enabling factor to facilitate accessing care—not only providing financial protection against potential catastrophic events but also offering immediate benefits for their household finances and decreased stress. Third, participants described prior stigma and discrimination while uninsured as a negative influence on access (predisposing factor), but that new insurance would be a social equalizer and allow them to be treated similarly to other insured patients. Fourth, participants viewed telephone-based application assistance as an important enabling factor to enroll in health insurance and by extension, access care. Each of these themes is described further in the sections that follow and in Table 2.
Themes, Representative Quotes, and Key Policy and Research Questions.

High Demand for Dental and Preventive Care
Dental services
While many participants spoke of having deferred a wide range of health care needs, including treatment for chronic medical conditions, filling prescriptions, or undergoing surgical procedures, they overwhelmingly described a need for dental care.
Thirty-three of 40 participants spontaneously discussed a need for dental care, without prompting from the interviewer, revealing a demand that had been building over years of inadequate dental coverage. Participants mentioned dental care in multiple contexts, including their hope regarding dental coverage in their new health plan, their intention to find a dentist, and their desire to have ongoing oral health complaints addressed.
Participants often listed dental care first among their responses to questions about health care more broadly, highlighting oral health as a priority and integral to their overall health. This was reflected in 1 participant’s story about his general health worsening with loss of his dental insurance:
I did have dental, but then when they stopped the coverage and then you couldn’t find as many dental places out here as they used to have. So, my health deteriorated right then and there . . . Some of the overall medical [problems] like my stomach I said that was really hurting. This is probably from teeth decay.
Participants described a desire to seek dental care immediately, often because of long-endured discomfort and the extraordinary steps they had been taking to cope with their oral health concerns. One participant shared,
I feel like I was becoming my own doctor. I hate to say those words, but I’m gonna say that. I have dental tools. I was doing my own dentistry. I shouldn’t be doing that. I don’t know what I’m doing. I was going on YouTube and seeing how to do the dentistry.
These stories were often accompanied by expressions of relief when participants learned that dental services were included in their new benefits.
Preventive care
Despite lacking recent experience with health care coverage, many participants described clear and specific plans for how they intended to use their new insurance. Several participants spoke of wanting to be actively engaged in their health and to remain healthy by receiving primary care, specifically a physical exam, blood tests, and other preventive services. One woman stated that she wanted to use her insurance “to get the medical attention that I need, so that I can live a healthier life . . . I want to make sure that I can get a complete physical of everything from cancer to whatever.”
Other participants stated that they were motivated by anxiety and anticipated negative health outcomes, even in the absence of symptoms. They feared being diagnosed with an illness that could have been prevented with earlier detection. One woman confided, “I’m concerned. I’ve never been this long without intervention. Prevention is the early cure to anything, and being without any insurance—I’m very, very alarmed because I don’t know what’s going on . . . ” Another woman shared that with health insurance, “I don’t have to be worried about that anymore . . . I feel so relieved.”
Decreased Stress and Financial Strain
Several participants described emotional stress and depression from having been uninsured. Their new health insurance offered a reduction in stress and the hope of improved financial security. For one participant, becoming insured promised relief from the profound emotional and physical burden of purchasing pain medications from others to relieve her pain. She was optimistic that having health insurance would help:
Maybe now, I could take those appointments that I was supposed to go to for the pain management, and maybe I can go fill the prescription for the muscle relaxers and see if it works. So I can stop buying narcotics on the street . . . I want to do things the right way. And now having this insurance will allow me to do that.
Competing financial pressures were common among participants. One woman shared, “We’re buying food, providing for my kids, you know for school and stuff. So it’s kind of hard. That’s why I couldn’t ever take care of my health because every time I had to go, I had to pay.” Another man described that he was “going deeper into debt every day.” He continued, saying that with insurance, “I’m hoping I can get myself out of debt and hopefully maybe even have a few dollars left over at the end of the month.” Participants anticipated an immediate decrease in financial stress upon enrollment in Medicaid.
Health Insurance as a Social Equalizer
Many participants described feeling discriminated against for having been uninsured in previous health care encounters. One participant said, “Those experiences had me feeling as though I came from a certain neighborhood or if I didn’t have no insurance, they don’t really try to give you the best help that they possibly can.” Such experiences served as a motivation to seek coverage, as participants hoped, if not expected, that insurance would be a social and health equalizer. One woman stated that with insurance, “I think it will be a much better visit. Because without insurance, they take care of you, but they don’t take good care of you.”
However, these optimistic statements were tempered by the reflections of participants who had had Medicaid earlier in life and for whom “welfare insurance” was still associated with substandard care. One participant recounted that, while previously covered by Medicaid, her daughter received inappropriate screening for hearing loss. Her pediatrician had explained, “she’s just ignoring you.” “Here my daughter was deaf in both ears . . . I feel, because I had welfare medical, it wasn’t worth checking . . . Some places don’t treat you the same if you don’t have work medical.”
Last, despite being recently enrolled in health insurance, many participants described a persistent feeling of health care insecurity. Several participants feared that their new insurance would be taken away suddenly, particularly if their income increased. One man stated, “I’m going to use that insurance to my full ability. Whatever I can get taken care of—everything. Because you never know when it’s gonna be taken away.” This discomfort was echoed by another participant, who said “I’ve waited for so many years to get it, and it’s like I’m so excited and then—I just feel like the floor’s going to be pulled out from underneath me.” For these participants, despite a hope that health insurance could be a social equalizer, tension remained regarding how much they would benefit from health insurance coverage, and for how long.
Application Assistance to Overcome Enrollment Challenges
In contrast to participants’ prior experiences in applying for medical coverage, which were described as “a headache” and “frustrating,” they universally described a smooth application process with telephone assistance from a benefits counselor. They described this assistance as an important enabling factor that allowed them to overcome significant enrollment barriers. Some participants valued the mail-based notification of their potential eligibility. One participant acknowledged, “I had no idea that we were entitled . . . if it wasn’t for [the benefits organization] informing me, I would have never in a blue moon thought about applying for medical coverage.” Counselors smoothed cumbersome and confusing administrative tasks, and participants praised the “one-stop shopping” application assistance.
Discussion
In this study of new Medicaid enrollees, participants described high levels of perceived need and pent-up demand for health services, particularly dental care and preventive services. They also anticipated that their new health insurance could alleviate stress and financial strain and reduce social inequities. Finally, participants highly valued the support of telephone application counselors in the Medicaid enrollment process.
The finding that dental coverage was a top health service priority was a surprise. Although poor oral health among low-income adults has been well documented, the perceived importance of dental care to our participants in the context of obtaining health insurance is noteworthy.15,16 Many perceived oral health as integral to their overall health, and their perceived dental needs may predict future dental service use. If this finding generalizes to other populations—as reports increasingly suggest it does—then dental benefits may be a salient and persuasive motivation for uninsured adults to obtain health insurance. 17 Dental services could also be leveraged as an overall entry point to the health care system, particularly for low-income adults.
Although most states provide some level of emergency dental services, less than half include comprehensive dental care. 18 With Pennsylvania’s transition to the traditional expansion of Medicaid, comprehensive adult dental coverage was included in all Medicaid plans. Dental coverage has been shown to increase utilization of dental care, while the elimination of dental coverage has been associated with increased emergency department visits for dental care.19,20 As new Medicaid enrollees gain dental and medical coverage, their pent-up demand may lead to significant early increases in use that stabilizes over time. 21 However, ensuring adequate availability of dental services will be an important next step to meet the immediate oral health needs of new enrollees. 22 Pennsylvania, like many states, is considered a “dental shortage area,” a problem compounded for Medicaid enrollees as not all dentists accept Medicaid reimbursement.23,24
Newly covered adults in our study expressed relief from both financial pressure and the significant stress associated with being uninsured, a finding also seen in the Oregon Health Insurance experiment that expanded Medicaid. 25 In a recent national survey, Medicaid enrollees reported fewer problems paying medical bills or incurring debt compared with both privately insured individuals and the uninsured. 26 Financial distress and being uninsured have been associated with increased stress and worse health outcomes.27,28 By mitigating financial barriers to care, health insurance is likely to serve as an important enabling resource for this population. Our findings may help explain why, following the Medicaid expansion in Oregon, there were reductions in the levels of depression among new enrollees, a finding that may spill over to other household members and should be explored. 29
Participants perceived that health insurance could serve as a social equalizer. Though discrimination in health care has been previously shown, this is a relatively new framing of health insurance’s influence on social structure, a predisposing factor in the Andersen model.30,31 Participants anticipated that their newly insured status would lead to improved social standing within the health care system, which in turn would lead to better care and less discrimination. This expectation may be fulfilled based on recent studies, one conducted following Michigan’s Medicaid expansion, in which Medicaid enrollees reported having sufficient access to a regular source of care and perceived their care to be of high quality.26,32 Participants in our study also perceived a multitiered status hierarchy among patients, such that privately insured patients received the highest quality care, with intermediate services afforded to publicly insured individuals, and the lowest quality care reserved for the uninsured. Whether Medicaid expansion will improve social equity for new enrollees warrants study.
The participants in our study described outreach and application assistance as an important community enabling factor to gaining coverage. Participants’ enrollment experiences contrasted sharply with barriers they encountered in the past, including onerous visits to welfare offices, the confusion of multiple forms, and challenges due to low health insurance literacy.33,34 Our study supports prior work on the ACA, arguing for the importance of preserving funding for insurance navigators, certified application counselors, and other enrollment assisters.35,36 The targeted outreach approach used by the organization in our study may be an important model for identification and enrollment of people unaware of their eligibility, who are disproportionately minorities.37,38
There are limitations to our study. First, our sample included Philadelphia residents newly enrolled in Medicaid. Although Philadelphia is similar to other urban areas with large minority populations and high rates of poverty, our results may not be generalizable to other geographic areas. Second, our results may be susceptible to selection bias. People electing to use assistance from a community organization or participate in a study may be different than those who do not. However, we are reassured by the similar demographics between study participants and the overall population seeking health insurance assistance from BDT (Table 1). Sampling from a benefits outreach organization that is identifying individuals from other public benefit programs also has advantages over sampling from a health care setting where individuals have already accessed care. Third, the structure and inclusion of dental benefits changed during our study period. Although we are unaware of any specific efforts that were made by either the Medicaid program or the benefits access organization to inform potential applicants of the addition of dental benefits, this change may have led participants to discuss their oral health needs. Fourth, our results do not quantify experiences. Instead, they identify and describe participants’ views about enrolling in Medicaid and how they intended to utilize their new benefits—insights that would be hard to uncover in close-ended survey questions.
As more states opt-in to the Medicaid expansion, enrolling the uninsured and meeting the expectations of new beneficiaries will be paramount. This is a unique population whose predisposing characteristics, resources, and needs may differ from preexpansion Medicaid enrollees. In addition, their enrollment experiences may differ as Medicaid moves to pure income-based eligibility and as new enrollees seek care amid a relatively large “surge” in covered individuals. Our study provides insights for policymakers and researchers on what these low-income adults may be seeking with their new coverage and the support they may need to enroll. Access to comprehensive dental coverage and preventive services are top priorities. Our study also points to other important areas for future research that could directly inform policy including how expanded coverage impacts mental health, financial strain, and perceived or actual discrimination in health care settings (Table 2). These factors may determine the degree to which Medicaid expansion achieves its goal of greater access and improved health for low-income Americans.
Footnotes
Acknowledgements
The authors thank Brian Gilmore and Evelyne Kruger for their assistance with participant recruitment, and Judy Shea for her guidance and input.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rachel Cahill is employed by Benefits Data Trust, the organization from which participants were recruited.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was made possible by grant number 6CPIMP141079-01-01 from the Office of Minority Health, Partnerships to Increase Coverage in Communities Initiative and by the Robert Wood Johnson Foundation Clinical Scholars Program at the University of Pennsylvania. The contents are solely the responsibility of the authors and do not represent the official views of the Department of Health and Human Services or the Department of Veterans Affairs.