
Abstract
Appointment nonadherence is a health behavior that represents a burden to health care systems. On March 1, 2015, a new negative reinforcement intervention involving “service fees” for a visit without appointment was implemented at King Abdullah University Hospital in Jordan. To evaluate the effect of this intervention in improving patient adherence to medical appointment, a retrospective preintervention and postintervention analysis was used, including all patients (n = 65 535) who had scheduled appointments at 39 outpatient clinics. A repeated-measures analysis of variance was first performed. Then, a multivariate linear regression model was used to identify factors that might predict individuals who are likely to attend or miss their appointments and those who have a greater tendency to visit the hospital with or without appointments. Although the average percentage of appointments attended was more than missed preintervention and postintervention, the decrease in percentage of missed appointments was more pronounced postintervention. Also, the average percentage of visits without appointments was less than visits with appointments in both times, but the decrease in the percentage of visits without appointments was more prominent after. The regression analysis revealed that younger, married and male patients were more likely to miss their appointment before and after the intervention. Also, younger patients had a tendency to attend without appointments. Conversely, patients with the lower copayment rate had a tendency to adhere to appointment times. In conclusion, negative reinforcement interventions could improve patient appointment adherence rates. Accordingly, interventions designed that consider evidence and are theory-based are needed to change patient behavior.
Introduction
Over the last years, there has been revived interest in adherence to medical appointments; this was strongly influenced by the high prevalence of no-show behavior and its subsequent impact.1,2 No-show prevalence rates vary across health care settings and populations. In the structured review conducted by Turkcan et al, 1 the mean no-show prevalence across the 62 studies included was 23.8%, with the highest rate occurring in North America (27.1%) and the lowest (14.9%) in Europe, whereas the rate was 24.3% for studies undertaken in Asia. 1
No-show behavior affects all parties involved in the delivery of health care, including patients, families, providers, and insurance agencies. For patients, missed appointments result in poor treatment adherence, disruption of multidisciplinary health care, and difficulty in patient-provider relationship. 3 They are also associated with increased risk of rehospitalization,4,5 poor control of chronic conditions,3,5 and can affect the health of other patients who lose the opportunity to receive timely care. 6 For health care providers, missed appointments reduce the chance of junior physicians to learn from different cases, 7 and could lead to staff underutilization, lower productivity, and increased costs.2,8-11
Several studies were conducted to identify the risk factors associated with no-show behavior and characteristics of those patients who are likely to miss their appointments. Many of these studies reached the same conclusion that being young, from minority racial or ethnic groups, or single, all significantly increased the likelihood of missing appointments.12-19 Other possible predictors were insurance status, gender, lower income, and day and time of appointment.18,19 A wide range of reasons why patients do not adhere to their medical appointments have also been extensively studied.
The most commonly self-reported reason for failure to attend was that patients “forgot” their scheduled medical appointments. This explains why reminding interventions (ie, phone calls, mails, and SMS) have received a substantial amount of attention, though reminders do not necessarily change patient behavior. Other identified reasons included lack of transportation, competing priorities with work time, family problems, difficulties with appointment scheduling systems, and patient’s health status such as feeling better or feeling too ill.20-22
To improve appointment adherence, several interventions have been utilized. Common interventions include appointment reminders, cancellation policy, patient education, and using a financial incentive.6,7,23-26 Despite the availability of these interventions, no-show behavior remains a burden to health care systems. Various policies have also attempted to curb the negative consequences of no-show behavior. Such policies include open-access or same day scheduling, follow-up after a no-show appointment, and overbooking appointments.27-30 Although these interventions and policies have been shown to reduce no-show rates, they are costly and labor-intensive, and their applicability is questionable.13,31
Overbooking, for instance, increases patient wait time and patient dissatisfaction, and might lead to work overload at specific times.24,32 It has also been found that open-access scheduling does not always result in a significant reduction in no-show rates.33-35 Moreover, it is impractical to impose financial penalties on those patients who did not attend their scheduled appointment, as well as ethical and legal issue. Insurance agencies such as Medicaid in the United States do not permit health care providers to charge no-show patients.2,20
New Intervention
Recently, on March 1, 2015, a new intervention was launched at King Abdullah University Hospital (KAUH), which is affiliated with the Jordan University of Science and Technology (JUST). Instead of using financial penalties, this intervention charges 15 Jordanian Dinars (US$21) for a visit without an appointment. If a patient misses a scheduled appointment, he or she has to wait a long time to reschedule a new appointment, and may search for other ways to be seen by doctors. Many patients try to use their social relationships to be seen, which places a heavy burden on hospital resources. Unscheduled appointments are considered overbooking, and negatively affect those patients who already have a scheduled appointment by increasing their wait time. Unscheduled patients also burden doctors by increasing the number of patients in the clinics, which causes doctors to have to rearrange patient time slots for those who have adhered to their appointments. The new policy applies to all outpatient services, irrespective of the nature of the visit. However, individual employees at KAUH and JUST, as well as their dependents, are exempt from the policy.
This intervention adopted by KAUH uses negative reinforcement to change patient behavior. In operant conditioning learning theory, negative reinforcement is defined as the removal, reduction, or escape of an unpleasant stimulus contingent upon a behavior, which results in an increased future rate of responding (behavior frequency).36,37 Negative reinforcement and punishment are often confused, because both involve the removal of an aversive stimulus. However, they differ from each other in how response is triggered and the effect on governing individual behavior.36,38 First, negative reinforcement entails avoiding a negative result when a desired behavior occurs, whereas punishment implies applying a negative consequence when undesired behavior is exhibited.36,39 Hence, by attending scheduled appointments, patients escape the negative consequences of a visit without an appointment. This in turn would decrease the appointment no-show rate. Second, negative reinforcement enhances the frequency of desired behavior, while whereas punishment reduces undesired target behavior.36,39,40 Instead of punishing those who do not attend their appointments, the intervention was introduced to increase the attendance rate.
Accordingly, the primary objective of this study is to identify whether the implementation of “service fees” for outpatient visits without a previously scheduled appointment as a negative reinforcer can improve patient attendance at scheduled appointments with the hospital. The study also aims to identify the main predictors of no-show behavior and visits without appointment.
Methods
Study Design and Data Collection
This is a preintervention and postintervention study 41 of all patients who had scheduled appointments from September 1, 2014, till September 1, 2015—6 months before and 6 months after—at KAUH. KAUH is a multispecialty teaching hospital with 527 beds; it provides a wide range of health services and is considered as a referral hospital for 4 cities in the North of Jordan. Services provided by KAUH are in high demand, especially the outpatient clinics, which are renowned for their competent medical staff and availability of advanced technology.
The data of the study were extracted retrospectively from the database of the 39 outpatient specialist clinics at the hospital. For each patient, the following data were obtained: attended appointments 6 months before, missed appointments 6 months before, total appointments 6 months before, attended appointments 6 months after, missed appointments 6 months after, and total appointments 6 months after. Similarly, the data included numbers of total visits 6 months before, visits with appointments 6 months before, visits without appointments 6 months before, total visits 6 months after, visits with appointments 6 months after, and visits without appointments 6 months after. In addition, data on demographic variables and patient characteristics such as fee exemption status, patient age, gender, marital status, and copayment status were also collected.
Ethical approval
This study received ethical approval from the institutional review board (IRB) committee at KAUH and JUST (No. 20160098).
Data Analysis
Descriptive statistics are reported for appointments showed up and visits with appointments before and after the intervention. As the data before and after the intervention were observed on the same patients, a repeated-measures analysis of variance (ANOVA) was conducted to examine the effect of the intervention on appointment adherence and visits without appointments. The significance of collected factors and covariates on the probability of attending appointments and the probability of visits with appointments was tested. Factors considered included intervention, exemption status, gender, marital status, and copayment. Age of the patient was treated as a covariate.
To identify factors that may predict individuals who are likely to miss their appointments and those who have a greater tendency to visit the hospital without prescheduled appointments, a multivariate linear regression model was used to relate the probability of adherence to appointments and probability of visits with appointments to the significant factors found in the repeated-measures ANOVA. The analysis was performed using SPSS 20.0.
Results
A total of 65 535 patients who had scheduled appointments during the study period were identified. The mean age of included patients was 36 (SD = 21) years of whom 37 487 were females (57.2%), 36 541 were married (55.8%), and 7431 of them had exemption (11.3%). Table 1 shows that the mean percentage of missed appointments decreased from 45.12% during the preintervention period to 41.27% during the postintervention period. This difference reflected a reduction of 8.53% and was statistically significant (P < .001). Interestingly, the mean percentage of visits without appointments reduced by 38.64% (P < .001), from 30.61% to 18.78% postintervention.
General Comparison Before and After the Intervention.

Effect of the Intervention on Appointment Adherence and Visits With Appointments
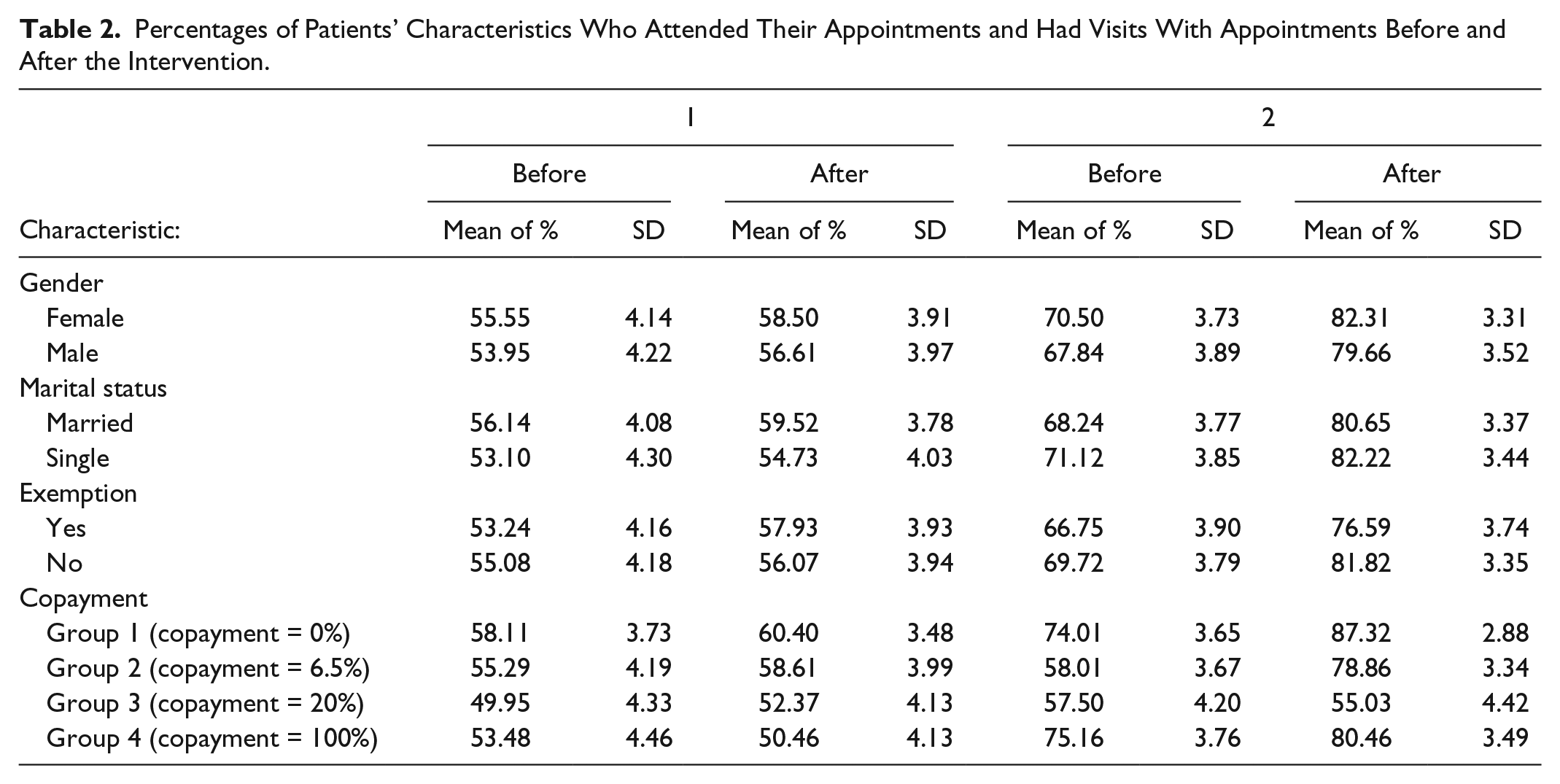
Based on the patients’ characteristics, means and SDs for percentages of attended appointments and percentages of visits with appointments before and after the intervention are shown in Table 2. A repeated-measures ANOVA with intervention (before and after the intervention) as within-subjects factor and gender (male, female), marital status (single, married), exemption status (yes [with], no [without]), and copayment group (groups1 through 4) as between-subjects along with patient age as a covariate was conducted. Two response variables were considered; the first was the probability of a show-up in an appointment calculated as the percentage of appointments the patient showed up of the total appointments (Table 3). The second response variable was the probability of a visit with appointment obtained as the percentage of visits with appointments of the total visits (Table 4).
Percentages of Patients’ Characteristics Who Attended Their Appointments and Had Visits With Appointments Before and After the Intervention.
Repeated-Measures ANOVA Within and Between Subjects for Shown Appointments.

Note. ANOVA = analysis of variance.
Repeated-Measures ANOVA Within and Between Subjects for Visits With Appointments.

Note. ANOVA = analysis of variance.
For the probability of a show-up in an appointment, ANOVA results revealed that intervention (P < .001), age (P = .018), gender (P < .001), and copayment (P < .001) were the significant factors along with the 2-factor interactions: Intervention × Age (P < .001), Intervention × Copayment (P = .002), Gender × Copayment (P < .001), and Marital status × Copayment (P = .004). Exemption status was a marginally significant factor with a P value of .093.
For the probability of visits with appointment, the effect of intervention (P < .001), age (P < .001), gender (P < .001), marital status (P < .001), and copayment (P < .001) were all significant. The following 2-factor interactions were also significant: Intervention × Gender (P = .051), Intervention × Copayment (P < .001), Gender × Copayment (P = .056), Marital status × Copayment (P = .003), and Exemption × Copayment (marginally significant, P = .062).
Predictors of Appointment Adherence and Visits With/Without Appointments 6 Months Before and 6 Months After
To mathematically identify the size of the effect for the significant factors found in the ANOVA, multiple linear regression was utilized to build models that relate probability of show-up in appointments and probability of visits with appointments to their predictors. Table 5 shows the estimated regression parameters along with their 95% confidence intervals (CIs). Based on the parameter estimates, we found that female patients had a higher probability of adherence to appointments than males, with increased probability after the intervention. In contrast, married patients were more likely to miss their appointments than single patients. Married patients have shown a slight improvement in the adherence after the intervention. Among copayment groups, group 3 patients had the lowest probability of adherence compared with other groups (before and after). This means that patients within the lower range of copayment rate had a tendency to attend their appointments. However, all groups have shown a significant increased probability of adherence after the intervention. Patients with no exemption have shown a slightly reduced probability of adherence to appointments after the intervention compared with that before the intervention. The results also indicated that older patients had a tendency to attend appointments, particularly after the intervention.
Multiple Linear Regression Estimates for Predicting Probability of Shown Appointments and Probability of Visits With Appointments Before and After the Intervention.

Note. CI = confidence interval.
In concordance with the above findings, female patients had a higher probability of visits with appointments than male patients. Also, the probability of visits with appointments for married patients has improved after the intervention. Patients with the lower copayment rates were less likely to attend without previous appointment, whereas younger patients were much more likely to attend without appointments. Finally, a substantial improvement in the probability of visits with appointment has been achieved after the intervention for patients with no exemption.
Discussion
Appointment adherence is a health behavior that remains a challenge for health care systems because of its detrimental effects on patient treatment and outcomes.3-5 However, appointment adherence has received little attention as a behavioral issue, compared with, for example, treatment adherence, or immunization uptake. 42
This study examined whether an intervention implementing fees for unscheduled visits would result in improving appointment adherence. Although reducing visits without appointments has been an objective of the intervention, the ultimate aim is to increase the rate of appointment adherence. The study found that the mean percentage of visits without appointments decreased significantly from 30.61% to 18.78%, and that the mean percentage of the no-show rate dropped from 45.12% to 41.27% after the introduction of the intervention. In addition, our results demonstrated that both visits with appointments and attended appointments have improved after introducing the new intervention.
Although there are a number of other interventions that have been shown to decrease the rates of no-show behavior, these interventions may have limited impact and lead to dysfunctional consequences. For instance, overbooking and open-access policies might increase the risk of overloading the schedules of health care providers, which requires careful observation and management, and accurate prediction of demand.24,43 In addition, many previously discussed interventions have only been used in research studies, and have not necessarily been applied in health care facilities, or used to motivate individuals to change their behavior.24,26,44,45
Nonetheless, the effectiveness of using financial incentives (rewards/penalties) in changing individual behavior has been theoretically substantiated and empirically supported in different health care settings.46,47 In a recent study, Kubanek et al 38 tried to address whether Thorndike’s law of effect is symmetric or qualitatively distinct in regard to monetary reinforcement and punishment. They found that reinforcement and punishment play a distinct role in guiding individual behavior. Punitive policies might be effective in reducing the no-show rate but are difficult to implement and can affect access to health care service, particularly among those patients with limited income. 17 Also, it might be unfair to charge those who had inevitable reason for not attending.2,13,48 In their qualitative study, Martin et al 20 argue that imposing financial penalties would have some effect in reducing missed appointments but would not be significant; furthermore, it might be not acceptable to providers to fine nonattending patients. In addition, such policies might encourage patients to cancel or reschedule their appointments. 49
Instead of fining those patients who missed their scheduled appointment, KAUH introduced the “service fees” as a negative reinforce to those who want visits without appointments. Thus, if the patient attends his or her scheduled appointment, he or she will not need to pay for a visit without appointment. In addition, negative reinforcement enhances the frequency of desired behavior, whereas punishment reduces undesired target behavior.36,39,40 In this regard, the main reason for the intervention is increasing the rate of appointment attendance rather than punishing those who do not adhere to their scheduled appointments.
Identifying the main characteristics associated with appointment adherence can also inform the development of interventions to reduce the occurrence of no-show behavior. 19 Our results confirm what has been previously found that younger patients are more likely to no-show than older patients.17-19 Older adults have more chronic conditions and long-term illnesses and missing scheduled appointments could adversely affect their health. They are more attentive to their health, and have enough free time compared with young adults. 26 Moreover, and in accordance with several previous studies,14-16 this study showed that male patients were more likely to no-show to their appointments before and after the intervention, though this has not been found consistently.1,50,51 Some previous studies also indicated that being married is associated with a low no-show rate,1,17 while we found that single patients were more likely to attend their appointments. Singles usually have less family commitments and it is easier for them to manage their time. Interestingly, having full insurance coverage was found to be significantly associated with a tendency to attend appointments. A possible explanation is that most patients with 0% copayment had government insurance and were referred from other government hospitals, or they had full insurance coverage from the Royal Court or from other agencies. However, in both cases, full coverage is usually time limited. So, such patients try to enjoy the greatest possible benefits, especially as most of the patients are from lower income families.
Finally, there are other patient characteristics and predisposing factors that have been identified in previous studies as potential influences on patient adherence to prescheduled appointments including health status, income, and race and ethnicity.1,52 However, as most inhabitants in Jordan are Arabs, Jordanian ethnicity and culture are characterized by uniformity and there are no racial and ethnic differences in Jordan. Other factors such as health status (chronic vs. acute) could also influence adherence to appointment. Chronic disease patients might be more apt to attend their appointments than patients with acute illnesses, because patients with chronic diseases usually have a good relationship with their caregivers, and they are more compliant with their treatment plan.1,17 In addition, the severity of health conditions might be associated with adherence to appointments; for instance, it has been shown that more ill patients are less likely to miss their appointments.1,17 Therefore, it is worthy to consider and examine the effect of these factors in future works to predict and improve appointment adherence.
Conclusion
This study demonstrates the ability of negative reinforcement to modify patient behavior and increase patient appointment adherence rates. Appointment adherence enhances the efficacy of health services. Besides using the scheduled appointment to provide adequate and timely patient care, health care settings maximize the utilization of existing resources. The study also highlights that developing an effective and socially appropriate intervention that could improve appointment attendance requires a clear explanation of the impact of such interventions from theoretical perspectives. Hence, health managers and policy makers need to consider evidence and theory-based interventions that go beyond merely the managerial practical issues. Further studies should focus on the empirical link between theory and practice in governing patient adherence behavior. Finally, we expect that visits without appointments and no-show rates could be further reduced than our reported results if the intervention is continued, as the current study examined impact only in the first 6 months of implementation.
Footnotes
Acknowledgements
We would like to thank Deanship of Research at Jordan University of Science and Technology for their keen help and support. Also, we are very grateful to Anas Matalkah, Manager of Information Systems Department at King Abdullah University Hospital (KAUH), for his technical support in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.