
Abstract
Size of primary health care (PHC) practices is often used as a proxy for various organizational characteristics related to provision of care. The objective of this article is to identify some of these organizational characteristics and to determine the extent to which they mediate the relationship between size of PHC practice and patients’ experience of care, preventive services, and unmet needs. In 2010, we conducted population and organization surveys in 2 regions of the province of Quebec. We carried out multilevel linear and logistic regression analyses, adjusting for respondents’ individual characteristics. Size of PHC practice was associated with organizational characteristics and resources, patients’ experience of care, unmet needs, and preventive services. Overall, the larger the size of a practice, the higher the accessibility, but the lower the continuity. However, these associations faded away when organizational variables were introduced in the analysis model. This result supports the hypothesized mediating effect of organizational characteristics on relationships between practice size and patients’ experience of care, preventive services, and unmet needs. Our results indicate that size does not add much information to organizational characteristics. Using size as a proxy for organizational characteristics can even be misleading because its relationships with different outcomes are highly variable.
Keywords
Introduction
Current developments in primary health care (PHC) organizations tend to favor large practices.1-3 It is argued that larger facilities foster implementation of information technologies such as electronic medical records, and recruitment of personnel such as nurses and other health professionals, which enhance patients’ access to a broader scope of services.3-6 Economies of scale are believed to result from such arrangements, thus increasing productivity and efficiency.7-9 Some researchers opposed this view, particularly in Europe 10 ; the main argument supporting this position is based on experience of care which, in many regards, is better rated by patients attending smaller practices and on possible diseconomies of scale as size gets larger.11-14 A recent review addressed this controversial issue and concluded that the evidence supporting the association between size and quality of care in primary care is limited.4,15 The situation is even less clear as practice size seems to be associated with the attainment of variable results, depending on the type of outcomes assessed. For example, larger practices have been found to improve accessibility, but at the expense of relational continuity. 16 The reverse is true for smaller practices, which achieve better relational continuity, but lower accessibility.17,18
Size is often used as a proxy for other organizational characteristics as it is posited to be associated with several organizational processes and structural features that, in turn, may impact on clinical and patient outcomes.19,20 It is important to identify organizational correlates of PHC organization size to understand more clearly the underlying mechanisms that explain the relationships between the size of PHC practice and patients’ outcomes, such as experience of care, preventive services, and unmet needs.
This article intends to address that question. It aims specifically to identify organizational characteristics associated with the size of PHC practice and to determine the extent to which the influence of size on experience of care, preventive services, and unmet needs is mediated by these organizational characteristics.
Methods
Our study consisted of 2 surveys conducted in 2010, in the 2 most populated regions of the province of Quebec: Montréal and Montérégie. 21 Each region was divided into territories, 12 in Montréal and 11 in Montérégie, under the governance of a Health and Social Services Centre. The two regions accounted for 43% of the total province’s population.
Population Survey
The first survey, a population-based telephone survey, involved 9180 randomly selected adults, aged 18 or older. 21 The sample was non-proportionately stratified (about 400 respondents in each of the 23 Health and Social Services Centre territories). Data were weighted by attributing the inverse probability of selection of participants resulting from the stratified 2-stage sampling (local area and intra-household). A post-stratification adjustment was applied for age and sex, based on 2010 estimated Canadian census data. The response rate to the survey was 56%.
The population-based questionnaire focused on respondents’ attachment to a practice, use of PHC services, experience of care, unmet needs, and preventive services received prior to the survey. The questionnaire was constructed mainly from 2 validated instruments designed to assess experience of care: the Primary Care Assessment Survey and the Primary Care Assessment Tool.22,23
Practice Survey
The second survey, conducted through the mail, included all PHC practices (N = 606) in the 2 regions. 21 We achieved a response rate of 62%. In every practice, a key informant, usually the physician responsible for professional and administrative matters, completed the questionnaire. As we had basic information on all practices, including the ones that did not respond, we applied a hot-deck imputation method to non-responding organizations, conditional on the area, the type, and the size of the practice group to which they belonged.24,25 The organizational questionnaire included 4 domains that characterize organizations26,27: vision refers to the goals, values, and policies shared by members of an organization; resources concern availability, quantity, and types of resources that can be mobilized by the organization; structure includes governance rules, and procedures that govern the behavior of organizational actors; and administrative and professional processes concern coordination mechanisms that underpin services delivery. The questions were based on various sources. 18 However, the authors formulated most of the questions according to the domains that were just presented. Choice of questions was guided by literature and proposals concerned with the implementation of the patient-centered medical home concept and integration of PHC.28,29 An initial validation of the questionnaire was achieved during a 2005 study. 30 Consultations were conducted with a group of experts to assess completeness and relevance of the questions. A pre-test was then carried out with practices located in geographical locations other than the 2 study areas. The Canadian Institute for Health Information used the questionnaire as a major reference source in the design of a questionnaire aimed at demonstrating PHC organization in Canada. 31 The questionnaire was also used in another study. 32
Organizational and population surveys were linked through population survey respondents’ identification of their regular source of PHC in the 2 years preceding the survey. Respondents who failed to identify a usual source of care were asked to identify the practice they attended most frequently in the past 2 years. This practice was then considered their usual source of care.
Outcomes Variables
Outcome variables included experience of care and preventive services reported by respondents who had used services during the 2 years preceding the population survey (2008-2010), and unmet needs in the last 6 months. Seven variables were constructed: accessibility of services, continuity of care, comprehensiveness, responsiveness, care outcomes, perception of unmet needs, and preventive services received (Supplementary File 1). The first five variables are indices of experience of care expressed as scores on a 10-point scale. As items composing the indices were more causal than effect indicators, we considered that the grouped indicators constituted composite formative indices rather than reflexive scales. 33 Therefore, we did not subject them to factor analysis, inappropriate to use with the formative approach, as indicators are not necessarily correlated with each other. 34 Preventive services variable was measured on a 10-point scale as for experience of care. Unmet needs in the 6 months preceding the survey were measured by a dichotomous variable (yes/no).
Explanatory Variables
The main independent variable was size of PHC practice, measured by the number of physicians working in the practice regardless of the number of hours they spent in that practice. The variable “size” was categorized as follows: small (1-2 physicians), medium (3-6 physicians), and large (7 physicians or more), based on the distribution of practice sizes to achieve a fair number of practices in each category.
Other independent variables included the following organizational characteristics:
Targeted population
Presence and role of nurses
Presence of medical specialists and other health professionals in the same building
Level of information technologies used in the practice
Quantity of specialized diagnostic services available in the same building
Collaboration with other PHC practices
Collaboration with hospitals
Services available on evenings or weekends
Predominant type of visits in the practice (walk-in visits or by-appointment visits)
Quantity of diagnostic or therapeutic services available in the practice
Average number of hours physicians devote weekly to clinical activities in the practice.
Supplementary File 2 provides operationalization details on these variables.
Data Analysis
We used logistic regression analysis to measure the association between size of PHC practice and each of the organizational characteristics. We tested the association of size of PHC practice and other organizational characteristics with patients’ experience of care, preventive services, and unmet needs by applying multilevel regression analyses, either logistic or linear, depending on whether the outcome variable was continuous or categorical. In our multilevel analyses, outcomes were level 1 variables, and organizational characteristics, level 2. Proportions of variance explained at each level of the models were estimated using Snijders and Bosker formulas. 35 All analyses were adjusted for sex, age, presence of morbidities, perceived health, level of education, and economic status (Supplementary File 3). We used STATA software (version 13).
Results
Association Between Practice Size and Other Organizational Characteristics
Table 1 presents the percentage distributions of organizational characteristics by practice size; Table 2 shows corresponding odds ratios for each characteristic, comparing medium and large practices with small ones. On most characteristics, small practices contrast with medium and large practices that both present higher percentages and larger odds ratios. Three characteristics show lower percentages and smaller odds ratios for medium and large practices: targeted population (clientele), by-appointment visits and average number of hours physicians devoted weekly to clinical activities. These are 3 distinctive characteristics favoring small practices.
Organizational Characteristics (%) by Size of PHC Practice, Montréal and Montérégie, 2010.

Note. PHC = primary health care.
Associations Between Size of PHC Practice and Organizational Characteristics.

Note. PHC = primary health care; OR = odds ratio.
We observe a gradient going from small size to large size practices in Table 2, particularly for resources and structure variables. For most of these variables, large practices have higher scores than medium practices. Medium and large practices do not differ much with respect to targeted population (whether it is all individuals presenting or the whole population) and predominance of walk-in visits.
Association of Practice Size and Organizational Characteristics With Experience of Care, Preventive Services, and Unmet Needs
With the exception of accessibility, which is higher for medium (P < .001) and large size practices (P < .001), most associations favor small practices, regarding unmet needs (P = .043; P = .023), continuity (P < .001; P < .001), comprehensiveness (P = .008; P = .002), responsiveness (P < .001; P = .014), and perceived outcomes (P = .025; P < .001) (Table 3). Medium practices do not differ significantly from small practices with respect to preventive services (P = .132).
Associations Between the Size of PHC Practice and Patients’ Experience of Care, Preventive Services, and Unmet Needs.

Note. PHC = primary health care; OR = odds ratio.
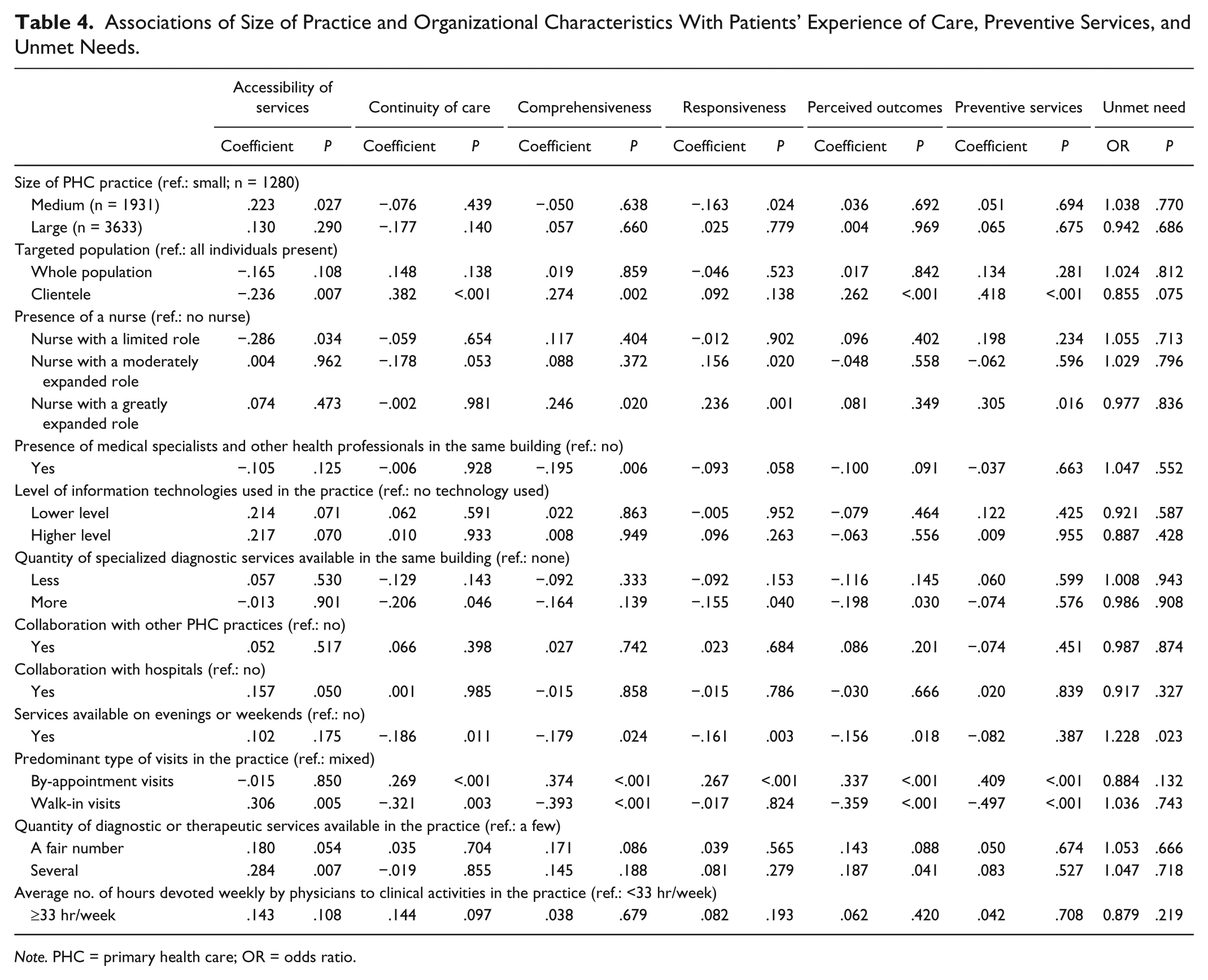
When organizational characteristics are added to the regression model, most relationships between practice size and outcome variables fade away (Table 4). Medium practices maintain a positive association with accessibility (P = .027) and a negative one with responsiveness (P = .024), in comparison with small practices. Surprisingly, large practices do not differ from small practices on these aspects of experience of care and score even better than medium practices on responsiveness (P = .002; data not shown). Among organizational characteristics, targeting a clientele rather than the broader population or all individuals who present is positively associated with most indices of experience of care, including unmet needs (P = .075), but negatively associated with accessibility (P = .007). The presence of a nurse who has a limited role is negatively associated with accessibility (P = .034). Having a nurse with a greatly expanded role is positively associated with comprehensiveness (P = .020), receiving preventive services (P = .016), and responsiveness (P = .001). The presence of a nurse with a moderately expanded role is also associated positively with responsiveness (P = .020). Availability of information technologies has a positive effect on accessibility (P = .070) but not on the other outcome variables. The presence of specialists and other professionals in the same building is associated with lower scores for comprehensiveness (P = .006), responsiveness (P = .058), and perceived outcomes (P = .091). Collaborating with other PHC practices has no effect, whereas collaborating with hospitals has a positive effect on accessibility (P = .050). Unexpectedly, offering services on evenings and weekends is not associated with accessibility (P = .175), and is negatively associated with continuity (P = .011), comprehensiveness (P = .024), responsiveness (P = .003), and perceived outcomes (P = .018). Favoring by-appointment visits increases continuity (P < .001), comprehensiveness (P < .001), preventive services (P < .001), responsiveness (P < .001), and perceived outcomes (P < .001), whereas emphasis on walk-in visits shows a negative association with these indicators, but a positive one with accessibility (P = .005). Quantity of services offered is also associated positively with accessibility (P = .007) and health outcomes (P = .041), but not with other variables. Finally, devoting more hours to clinical activities in the practice slightly increases continuity (P = .097), but has no association with other outcome variables.
Associations of Size of Practice and Organizational Characteristics With Patients’ Experience of Care, Preventive Services, and Unmet Needs.
Note. PHC = primary health care; OR = odds ratio.
To further assess the respective contribution of size and of other organizational characteristics to variations in the outcome variables, we compared the percentage of variance explained by level 2 variables with size only and with other organizational characteristics (Table 5). The data show the results of three combinations of level 2 variables. The variance explained by level 1 variables remains unchanged. For level 2 variables, variance is much higher with organizational characteristics other than size than with size alone for all outcome indicators. Furthermore, the addition of size of PHC practice to organizational characteristics does not increase substantially the variance explained by level 2 variables and, in some cases, even decreases it. This clearly indicates that organizational characteristics other than size are better predictive and explanatory variables than size alone.
Proportions of Variance Explained at Each Level by Models Including Different Combinations of Level 2 Predictors.

Note. PHC = primary health care.
Discussion
This study adds to the sparse literature exploring the relationship between the size of PHC practices and processes of care. It highlights that size is closely associated with organizational characteristics. Overall, the larger the practice, the more resources and desirable structural features it had. In contrast with medium and large practices, small ones tended to give priority to their regular patients and offer fewer walk-in slots. Furthermore, doctors in small practices devoted a greater portion of their time in their practice. In sum, small practices are more akin to closed systems centered on limited numbers of regular patients than medium and large practices. The latter are more complex open systems, centered on larger and more differentiated clientele. Casalino et al obtained somewhat similar results in their large-scale study of physician practices in the United States. 36 They found that practices of at least 3 physicians had more patient-centered medical home features than smaller practices of 1 or 2 physicians. These features included most of the organizational characteristics of our study.
A second finding of our study concerns relationships between size of PHC practice and processes such as patients’ experience of care, preventive services, and unmet needs. We found that greater accessibility was associated with medium and large practices, but that small practices performed better than medium and large ones on continuity, comprehensiveness, responsiveness, and perceived outcomes. Patients in small as well as in medium practices reported receiving more preventive services than those in large practices. Despite a relative lack of consistency across studies, our results agree with those reported in recent studies.9,15,18,37
An Ontario study found that larger size practices were associated with better access and comprehensiveness, but worse continuity of care. 17 They found no association between practice size and chronic disease management or health counseling. Another Ontario study found that practices with 4 or fewer full-time equivalent family physicians offered better quality chronic disease management. 13 A recent review found that patients in smaller practices report better experience of care, including accessibility, but when chronic care and preventive services were the outcomes, larger practices did better. 15 Pineault et al studied the performance of different PHC organization models in the management of chronic diseases in Québec. 16 They found that group practices with high degrees of integration and coordination and those providing greater proportions of walk-in visits were the most accessible, whereas solo practices were the least.
In a European study, Wensing et al found that patients reported a better experience of care in smaller practices, except for urgent health problems that needed quick responses. 10 However, these findings were not consistent across all countries. The Casalino et al large American study of 1045 primary care practices established that compared with larger practices (10-19 physicians), smaller practices (1-2 physicians) had 33% fewer preventable hospital admissions, and medium ones (3-9 physicians) had 7% fewer. 36 The authors concluded that their results questioned the commonly held assumption that bigger is better. The results of Haggerty et al also challenged this assumption: The authors found that solo practitioners offered accessibility that was comparable with group practices, and that accessibility and continuity decreased when practices had 10 physicians and more. 20
In a Quebec study of PHC practices, Beaulieu et al found a modest association between number of physicians and quality of care, measured by a score of conformity to clinical guidelines. 32 They interpreted this result as evidence supporting the view that smaller practices, and particularly solo practices, were likely to provide lower quality of care. This conclusion is unwarranted, as the authors excluded from their study practices of 3 physicians or less. In their study of Québec solo practices, Pineault et al distinguished 4 types of solo practices. 12 They found that the 4 types scored very high on patient experience of care, except for accessibility. However, among the 4 types, the one that performed best was the “resourceful networked” model and the least, the “resourceless isolated.” This suggests that interorganizational collaboration and networking are potent ingredients to improve patient outcomes in small practices, particularly solo practices.
The lack of consistency across the different studies described above partly reflects the fact that size is a proxy for numerous organizational characteristics that may relate differently to various care processes. This issue was addressed by the third, and perhaps most important finding reported in the article: the mediating effect organizational characteristics had on the relationship of practice size with patients’ experience of care, preventive services, and unmet needs. Although several studies have alluded to it, as far as we know, no one has ever examined this mediating effect. 4
Among the variables that contributed most to this effect were targeting regular patients rather than the broader population or anyone who presents to the practice, consultations offered on evenings and weekends, predominance of by-appointment visits rather than walk-in visits, and presence of nurses with expanded roles. Targeting regular patients and predominance of by-appointment visits, as opposed to walk-in visits, were associated with continuity, comprehensiveness, perceived outcomes, reporting unmet needs, and receiving preventive services. Conversely, predominance of walk-in visits had a negative effect on those aspects of experience of care, but a positive one on accessibility. Several authors have observed this antagonistic interaction between continuity and accessibility.4,9,15,17,19
The presence of nurses with greatly expanded roles had a positive influence on aspects of experience of care related to comprehensiveness, receiving preventive services, and responsiveness, but had no influence on accessibility and continuity. This indicated an important contribution of nurses to PHC care that could potentially be enhanced if they had more autonomy. In such conditions, continuity and accessibility would also likely improve.38,39 In addition, the influence of information technologies, their influence on improving accessibility was limited, regardless of the type of information technologies. This suggests that although information technologies are basic elements associated with the patient-centered medical home model, 28 they could contribute mostly to improving accessibility instead of other aspects of experience of care, even those related to physician-patient relationships.40-42 Finally, collaboration with hospitals and quantity of services offered in a clinic provided greater accessibility, but did not influence other aspects of patient experience of care.
These results show that associations between outcome indicators and organizational characteristics are highly variable. Hence, measuring these characteristics by a proxy such as size, even if they are correlated with it, can be misleading.
Conclusion
Size of PHC practice has a determining effect on patients’ experience of care, unmet needs, and preventive services. However, this effect is largely mediated by organizational characteristics, such as targeting regular patients rather than any individual who presents to the clinic or the broader population, being open in evenings and on weekends, and predominantly having scheduled visits as opposed to walk-in visits. Relationships between these different characteristics and outcome variables vary, which has research implications. First, using size as a proxy for organizational characteristics results in a loss of important and useful information and of capacity to explain the more specific reasons for better experience of care. This is particularly true when size is used as a predictor variable for processes of care. Hence, when information is available on other organizational characteristics, size does not add much to explain variations in outcome variables. Second, information about size on its own does not help to answer the often asked question, “What is the optimal size for a PHC practice.” 4 Answering this question is not a simple task. Contexts are very different, as evidenced when contrasting, for example, situations in Europe, the United States, and Canada regarding PHC organization. In addition, practices of different sizes seem to complement rather than substitute for each other. This point is well illustrated by the finding that continuity is better attained in small practices, and accessibility better attained in large practices in contexts that foster interorganizational collaboration and horizontal integration. 43 This has important policy implications. The current trend observed in many countries to create large-size mega practices may not be the best solution. From a system perspective, to ensure PHC services of quality for the whole population, practices should perhaps organize into networks of practices of various sizes rather than into large clinics with many health care professionals. 10 This approach implies that links among PHC practices of various sizes through interorganizational collaboration are preferred to solutions that are based on merging organizations. 44
Footnotes
Acknowledgements
Michel Fournier advised on and supervised statistical analyses carried out by Alexandre Prud’homme. Sylvie Gauthier revised the manuscript. Pierre Tousignant and Audrey Couture also brought their contribution in drafting the manuscript. The authors also acknowledge the following collaborators and researchers associated with the project: D. A. Roy, J. L. Denis, P. Lamarche, M. D. Beaulieu, J. Haggerty, D. Roberge, J. Côté, M. Hamel, F. Goulet, S. Dulude, M. Drouin, J. Rodrigue, and O. Lemoine.
Author Contributions
Raynald Pineault participated in all the stages of the study and drafted the manuscript. Sylvie Provost and Jean-Frédéric Levesque participated in the study design and the conduct and in drafting the manuscript. Roxane Borgès Da Silva and Mylaine Breton also participated in drafting the manuscript. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Canadian Institutes of Health Research (PHE 101905), Fonds de recherche du Québec–Santé (FRQS; 22032), Agence de la santé et des services sociaux de Montréal, and the Agence de la santé et des services sociaux de la Montérégie.