
Abstract
Life expectancy at birth is considered the best mortality-based summary indicator of the health status of the population and is useful for measuring long-term health changes. The objective of this article was to present the concept of the bottom-up policy risk assessment approach, developed to identify challenges involved in analyzing risk factor reduction policies and in assessing how the related health indicators have changed over time. This article focuses on the reasons of the significant life expectancy prolongation in Poland over the past 2 decades, thus includes policy context. The methodology details a bottom-up risk assessment approach, a chain of relations between the health outcome, risk factors, and health policy, based on Risk Assessment From Policy to Impact Dimension project guidance. A decline in cardiovascular disease mortality was a key factor that followed life expectancy prolongation. Among basic factors, tobacco and alcohol consumption, diet, physical activity, and new treatment technologies were identified. Poor health outcomes of the Polish population at the beginning of 1990s highlighted the need of the implementation of various health promotion programs, legal acts, and more effective public health policies. Evidence-based public health policy needs translating scientific research into policy and practice. The bottom-up case study template can be one of the focal tools in this process. Accountability for the health impact of policies and programs and legitimization of the decisions of policy makers has become one of the key questions nowadays in European countries’ decision-making process and in EU public health strategy.
Introduction
Many epidemiological studies find a range of health outcomes (eg, mortality) to be consistently related to provided policy.1,2 This is made possible by identifying and affecting risk factors directly connected with some health outcomes. The results in health outcomes might be related to many different policies at the same time.
The conceptual model of the determinants of health inequalities of the World Health Organization (WHO) concludes the influence of the main aspects that affect inequalities in health, the majority of them being outside the health sector. 3 Following this conclusion and considering the factors that affect equity in health and well-being, it is necessary to reinforce the need for considering the concept of “Health in All Policies.” In Poland, like in other Central European countries (eg, Czech Republic, Slovakia, Hungary), the life expectancy has significantly improved over the past 20 years. This process has started after political and socioeconomic transformation in the region that started in 1989. This study focuses on how this interaction has caused significant life expectancy prolongation in Poland over the past 2 decades and thus includes health policy context. As an example of effective population health management, it may aid decision makers, public health experts, and health promoters in engaging in scientific and intellectual reflections on how to improve population health and the distribution of health outcomes within a given population in the future.
The objective of this article was to present the concept of the bottom-up policy risk assessment approach, developed to identify challenges involved in analysis of risk factor reduction policies and in assessing how the related health indicators have changed over time.
This study was a part of a European Commission’s public health research project Risk Assessment From Policy to Impact Dimension (RAPID). 4 The aim of the project was to develop and provide policy makers with methodological guide for the assessment of the complex impact structure of policies in relation to the health of the population. 5 Because of the project limitations, we were not able to do any modeling study to examine how much of the observed increase in life expectancy in Poland could be attributable to the risk factor reduction due to implemented policy. We tried to point out the health effects of policy change in Poland over the past 20 years; our methodological considerations were pilot tested based on a literature review.
Methods
The Model: Bottom-Up Risk Assessment Approach
An extensive literature review and documentation analysis was based on the widely acknowledged scientific sources: PubMed/Medline, Embase, CINAHL, WHOLIS, Eurostat Healthcare statistics. National and international reports, legislative documents, health statistics, and programs were studied for the 20-year period 1990 to 2010.
A case study has been performed based on the bottom-up approach model; a chain of interaction between the health outcome, risk factors, and determinants of health and policy is presented in Figure 1.

Bottom-up health risk assessment model.
Health outcome is the starting point of the impact assessment chain. It should be clearly defined (eg, ICD-10code) and measurable. The second step of the assessment procedure is to list acknowledged risk factors and to describe all proven connections of the risk factors and health outcome and interactions between the risk factors. The next point of the bottom-up methodology chain aims to systematize scientific knowledge concerning the relation between determinants of health and risk factors that are supposed to be influenced by the policy level. The policies can either be on central, regional, or local level, orconducted by industry or other organizations’ activities. Using this model should allow for the quantification of health outcomes from an existing or a new policy through its implications for health determinants and associated risk factors and provide decision makers with practical information on expected changes of health outcomes. This approach guides the analysis of causal chains from the health outcomes to the policy. The main aim of this article was to develop the assessment model, not the assessment itself. The development of the “full chain” approach model was the key issue and naturally, the model is not changing due to change in data. It is a robust model and can be applied both with old and new data, the important is to draw the impact chain across four levels (health outcome, risk factors, health determinants, policy).
Based on the WHO reports and evidence-based literature, we identified four key risk factors that are strictly connected with cardiovascular disease (CVD) mortality; they are also in big part related to public health policy: tobacco and alcohol consumption, diet and physical activity, the socioeconomic background, and health care system effectiveness.
Tobacco use is the second leading global risk for mortality (9%); it is one of the most important risk factors concerning CVD and accounted for 18% of deaths in high-income countries. 6 There is strong evidence of relations between smoking and CVDs. 7 Generally non-smokers live many years longer and they are free of CVD longer than smokers, but at the end of their lives, non-smokers will have lived longer with CVD. 8
According to the WHO, alcohol consumption is mentioned as the third most dangerous risk factor for population health, responsible for 9% of total global burden of diseases (GBD) and traumas. 9 WHO estimated economic costs of the alcohol problems as 2% to 3% of the gross domestic product (GDP) and it takes the third place for the world disability-adjusted life years (DALYs; 5%).
There are strong associations between the prevalence of obesity and physical inactivity and the increase of CVD in the population 10 ; for example, 45-year-old obese men with no CVD survived a few years less than their normal weight counterparts, whereas, for women, the difference was even longer. Obesity before middle age is related to a reduction in the number of years lived free of CVD. 11 Economic conditions result in a diet quality, which contributes to the health status of a population. In analyses of large group of countries, positive associations were observed between higher income inequality and mean body mass index (BMI), obesity prevalence, and between coronary heart disease (CHD) mortality rates. 12
Physical activity positively influences health conditions. Frequent physical activity results in lower heart rate and reduces the incidence of arrhythmia and rapid cardiac arrest, 13 so it is significant in terms of life expectancy for men and women free of CVD. This effect is already seen at moderate levels of physical activity, and the gains in CVD-free life expectancy are twice as large at higher activity levels. 14 According to WHO recommendations, adults aged 18 to 64 years should undertake at least 150 minutes of moderate-intensity aerobic physical activity throughout the week, or undertake at least 75 minutes of vigorous-intensity aerobic physical activity throughout the week, or a combination of moderate- and vigorous-intensity activity. 15
Income conditions, social status, quality of work, education, unemployment, social exclusion, and poverty are the most representative elements of the socioeconomic determinants of health. Various international research confirms the impact of social capital on health, and a particularly strong relationship between gross national product (GNP) per capita and life expectancy. 16 Per capita income and the structure of health expenditures financed by the government are strongly associated with better health outcomes. 17 There is also a consistent correlation between national income inequality and population health at the country level. Change in inequality is significantly related to change in life expectancy. 18
According to the WHO, lack of adequate access to health care is one of the health risk factors for a population. 19 Primary care is the first level of contact with the health care system, which should be universally available. Modern and efficient primary care takes responsibility for both health promotion and public health activity. 19 Increased accessibility to primary care physicians contributes to better health and lowers overall costs in the health care system. 20
Results
Health Outcome—Life Expectancy
Life expectancy is defined as the average number of years a person can expect to live in the future. It reflects the overall mortality level of a population and summarizes mortality patterns that prevail across all age groups. 21 It is considered the best mortality-based summary indicator of the health status of the population. 22 It is also useful for measuring long-term health changes. 23
The political transformation in 1989 was a brand new challenge for Polish society and in the beginning it resulted in a decrease in life expectancy at birth. In 1990, life expectancy at birth in the EU-15 region was longer compared with Poland: 6.56 years for men and 4.34 for women. 24 However, life expectancy at birth in Poland has consistently increased since 1993 and over the past 2 decades has systematically risen, which is presented in Figure 2.

Life expectancy in Poland (1989-2012).
Life expectancy is strictly connected with mortality rate. Various recent studies indicate that increases in life expectancy were mostly achieved by reductions in CVD mortality and infant mortality. 25 We conducted our case study referring to CVD mortality as a main factor that was attributed to the life expectancy increase in Poland over the past 2 decades: 1990 to 2010.
CVD Mortality Rate
In most highly developed countries, CVD rate has decreased since the 1970s. These improvements were mainly attributable to changes in the three main cardiovascular risk factors, smoking, raised cholesterol concentration, high blood pressure, and also to better treatment. 26 Over the last 40 years in Germany, reductions in CVD mortality had the greatest cumulative impact on life expectancy. 27 In the same period (in the 1970s, 1980s), CVD mortality rate had a dramatic and steady increase in Poland and in the whole region of Central and Eastern Europe. In the beginning of the 1990s, CVD mortality in Poland was among the highest in Europe for both men and women. Since then, it has been steadily decreasing and when compared with all Central European countries, Poland has achieved the greatest success in CVD mortality reduction, which is presented in Figure 3.

Standardized CVD mortality rate in Poland.
Over the past decades, it has decreased in the young and middle-aged population (aged 20-64) by 40% and in this period, the decline was 3 times greater in women and 2 times greater in men than in the EU-15. 23 Life expectancy prolongation in Poland over the past decades is strictly connected with the decreasing death rate from CVD, which is responsible for about 46.0% of deaths (in Western European countries, it is less—approximately 40%). The latest report confirms that in period 1990 to 2010, the life expectancy prolongation is 51% in the case of men and 61% in the case of women attributed to reduction in CVD mortality. 28
Health Determinants
Many agents affect life of individuals and communities. Health determinants are connected with social, economic, and physical environments, and a person’s individual characteristics and behaviors. Lalonde postulates that individual health is 50% determined by lifestyle, 20% by genetics, 20% by environmental factors, and 10% by health care activity. 29 The Dahlgren and Whitehead model includes the following factors: general socioeconomic, cultural, and environmental factors, living and working conditions, social and community factors, and individual lifestyle behaviours. 30 Income conditions, social status, education, quality of work, unemployment, social exclusion, and poverty are the most representative elements of socioeconomic determinants of health. Our consideration refers to lifestyle determinants and health system activity.
Risk Factors
According to the WHO, 8 risk factors—alcohol and tobacco use, hypertension, high BMI, high level of cholesterol, high blood glucose level, low fruit and vegetable consumption, and low physical activity—account for 61% of cardiovascular deaths and the combination of the above mentioned factors results in about 75% of ischemic heart disease risk factors (the leading cause of death worldwide). 6 In this report, WHO concludes that reducing exposure to these 8 risk factors would increase global life expectancy by almost 5 years. Previous studies in the United Kingdom and United States showed that about half of the reduction in coronary deaths between 1980 and 2000 could be associated with reductions in major risk factors and about half with improvements in medical treatment.31,32 The implemented public health policies including increasing physical activity, non-smoking, and normal weight together with easy access to modern medical treatment are an effective means to reduce the incidence of CVD and could result in further improvements in life expectancy. 10 It is important to note that total life expectancy of normotensives is a few years longer in comparison with hypertensives, and increased blood pressure in adulthood is associated with large reductions in life expectancy; this affects both men and women similarly. 14 Very recent research provides evidence that the decrease in CVD mortality in Poland was mostly achieved thanks to changes in key CVD risk factors.23,33 Others show that the reduction in mortality mostly reflects the dynamic development of medical and clinical treatment in the 1990s. 34
Tobacco consumption
Tobacco consumption has risen steadily over the decades, and in the beginning of the 1980s Poland belonged to the group of countries with the highest consumption of tobacco in the world. 23 In 1982, at the peak of smoking prevalence, about 68% of men and 34% of women aged 20 to 64 years smoked. Tobacco consumption decreased by about 30% in the period 1985 to 2005. It remained in 2010 at 33% for men and 20% for women, and 27.8% for the entire Polish population compared with 29.3% (2005), 32.3% (2000), 37.9% (1995), which is presented in Figure 4.

Percentage of regular daily smokers in the population, age 15+ (WHO, Health for All [HFA] database).
The highest rate of smokers is among unemployed and workers, most of whom are men with vocational education (34.5%). The most significant decrease in the rate of smoking was in the managers group (34% in 2010 compared with 46% in 2000). The lowest rate of smokers can be observed in the group of people with high education; 19.1% in 2010 compared with 23.4% in 2000. 35
Alcohol consumption
An increased quantity of alcohol results in the increase of cardiovascular mortality; 36 ; for example, the decrease in CVD mortality, observed in the 1980s and 1990s in Russia, was considered as an effect of reduced alcohol consumption that was the result of Gorbachev’s anti-alcohol campaign. But it is important to note that the pattern of drinking plays a key role. Traditionally, Poland was a liquor-drinking country and, at the beginning of the 1980s, vodka constituted 70% of the alcohol consumed. Since the beginning of the 1990s, a decreased share of spirits, which is presented in Figure 5, and an increased share of beer were observed. In the beginning of the 21st century, beer constituted 55% of total alcohol consumption, spirits 26%, and wine 19%. 23
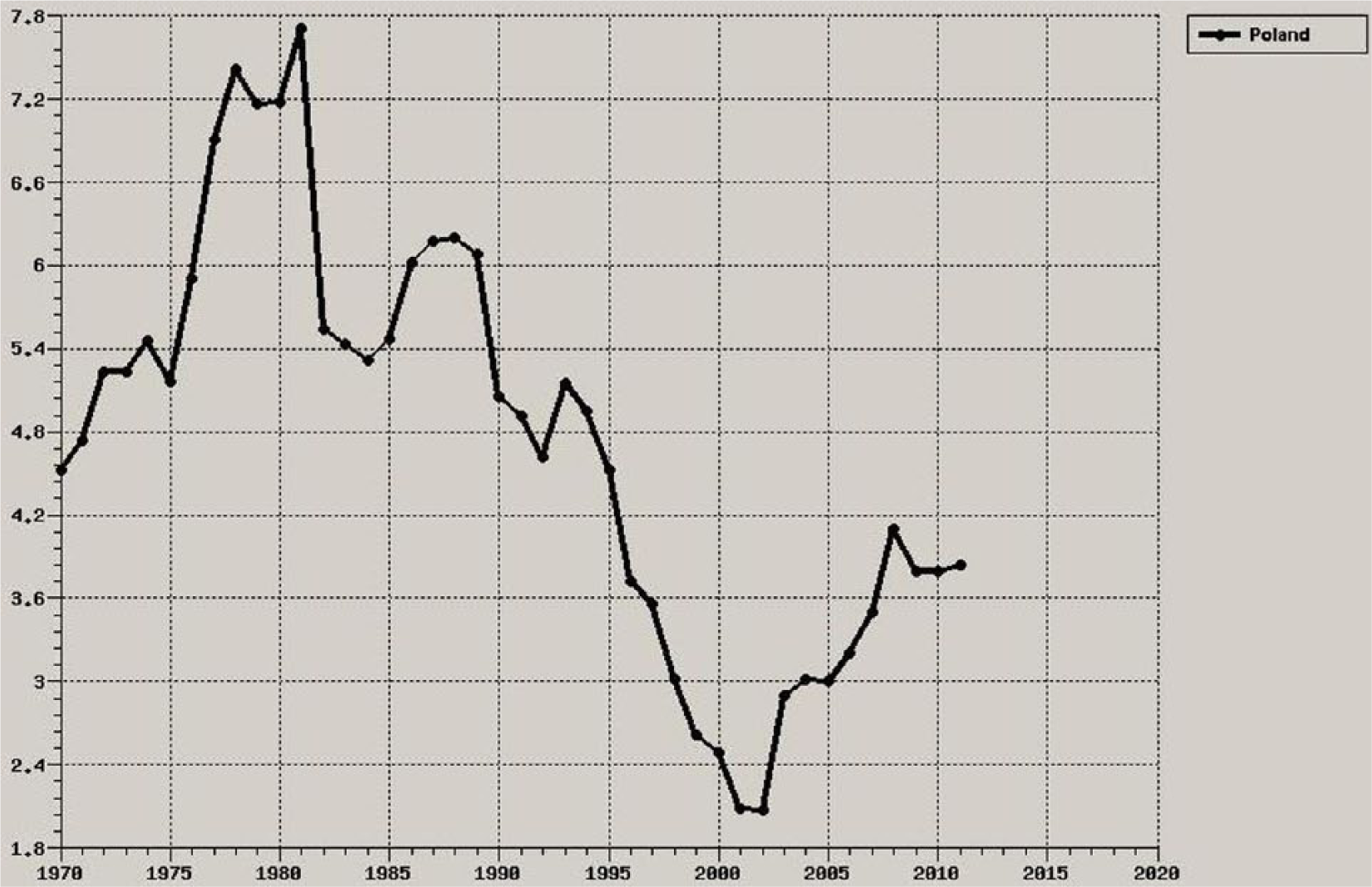
Spirits consumed in pure alcohol in Poland, liters per capita, age 15+ (WHO, Health for All database).
Diet
Over the past decades, we have observed significant changes in the diet structure in Poland, so fruit (including fruit preserves) and vegetable consumption has increased. The main increase concerned the consumption of apples, citrus fruits, and bananas. The consumption of citrus fruits increased 4 times in the period 1989-1997 (from 2.5 kg/cap/year to 10 kg/cap/year). In the period of 1990-1997, a total consumption of fruits and fruit preserves increased from 29 kg/cap/year to 53 kg/cap/year. 37 In the period 1989-2005, a decline in saturated fat consumption and an increase in unsaturated fat consumption (both polyunsaturated and monounsaturated) were observed, which is presented in Figure 6. This was achieved by changing dietetic patterns of the Polish population. Fish and poultry became much more popular than red meat. In the end of 1980s, the average consumption of poultry was estimated on a level of 30 kg/cap/year and in 2005, 55 kg/cap/year. 38 Although the access to a variety of food has improved, daily energy supply decreased, and since 1990 has been at a level of about 3300 kcal/cap. 23

Fat intake in Poland (kg/person).
Physical activity
Physical activity among Polish citizens has risen steadily over the past 2 decades and is now close to the EU average. The health benefits that came from increases in leisure time physical activity in Poland are well documented.39,40 There was an observed decline in prevalence in physical inactivity in Poland in men from 64.6% in 1991 to 38.75% in 2005 and in women from 68.8% to 44.5%, respectively. 40 The recent studies confirmed that the decrease in physical activity in the period 1991-2005 contributed in 10% of the fall in CVD mortality in Poland, that is, resulted in about 2500 fewer coronary deaths. 33 Over half of adult men and women do not achieve the adequate recommended level of physical activity; there is also a significant territorial diversification in physical activity among Polish society. 23
Socioeconomic circumstances
The experiences of Eastern and Central Europe in the last decades provide an example of how social transition can influence the health of a population. 41 The temporal decrease in life expectancy value in Poland from 1990-1992 could have been influenced by rapid economic and social changes, which affected a majority of population. Expenditures on health, culture, and others became less significant comparing with food expenditures and housing payments after 1989. Unemployment (6.5% in 1990), a dramatically increased inflation rate (1.395% in 1990), and inadequate salaries were brand new phenomena. 42
Over the past decade, the majority of the socioeconomic indicators in Poland reached the European average. From 2000 to 2009, the rate of households with any kind of savings increased to 32% whereas that of the group of people with savings of over 1 year of earnings has grown steadily from 8% in 2000 to 19% in 2009. Household equipment rate has also increased significantly. Access to Internet has grown by 400%, the number of stationary computers by 400%, notebook possession has increased by 800%, microwave ovens by 300%, and dishwashers by 500%. 35
The psychological condition of Polish society has changed as well. The rate of people who consider themselves very happy has increased from 3.7% in 1991, 5.2% in 2000, 5.8% in 2005 to 9.4% in 2009. In other words, the rate of people who described themselves as unhappy has decreased from 4.5% in 2003 to 2.4% in 2009. 35
In general, some experts explain the phenomenon of positive health changes in Polish society as a result of the introduction of democracy. 23 It is also confirmed by other studies, which even concluded that democracy, civil liberties, and political rights are related to health status. In some research, democracy showed more significant association with health status, (e.g. life expectancy), than economic indicators such as GNP, total government expenditure, or inequality in income. 43
More accessible health care system
More effective primary care sector
The higher effectiveness of the primary care sector was one of the main aims of health care reforms in Poland after 1989. The implementation of Universal Health Insurance Act in 1999 44 was the starting point of the primary care transition; non-integrated primary care, based on four specialists—pediatrician, gynecologist, dentist, internist—was replaced by the new institution of the general practitioner. Introducing the institution of the family physician led to the end of the historical undervaluation of primary care in Poland. General practitioners started to play an important role in health promotion and health education (eg, prophylaxis of heart disease program and tobacco-related disease program)
Development of new technologies: Invasive cardiology in Poland
Scientific data underline the significant role of increased access to modern treatment procedures over the past 2 decades in Poland.13,34 An increasing number of diagnostic and therapeutic procedures for patients with acute coronary syndromes during the first hours after significant pain appearance is one of the main factors that helps to reduce the death rate from acute coronary syndromes, stroke, and apoplexia cerebri. 13 A rate of 1000 angioplasties per year was achieved in 1989 and in 1997 it reached 5000; then in 1998, the number of angioplasties and stents was doubled, with a 24% increase in coronarography procedures during the same period. In 1999, there were 31 invasive cardiology centers in Poland and the total number of coronarographic procedures grew by 31.8% and angioplastic procedures by 32.8% compared with 1998. 45 Number of invasive cardiology procedures is presented in figure 7. Since 2011, the total number of 127 invasive cardiology units, located in all 16 voivodeships, has exceeded the level in highly developed countries. 45
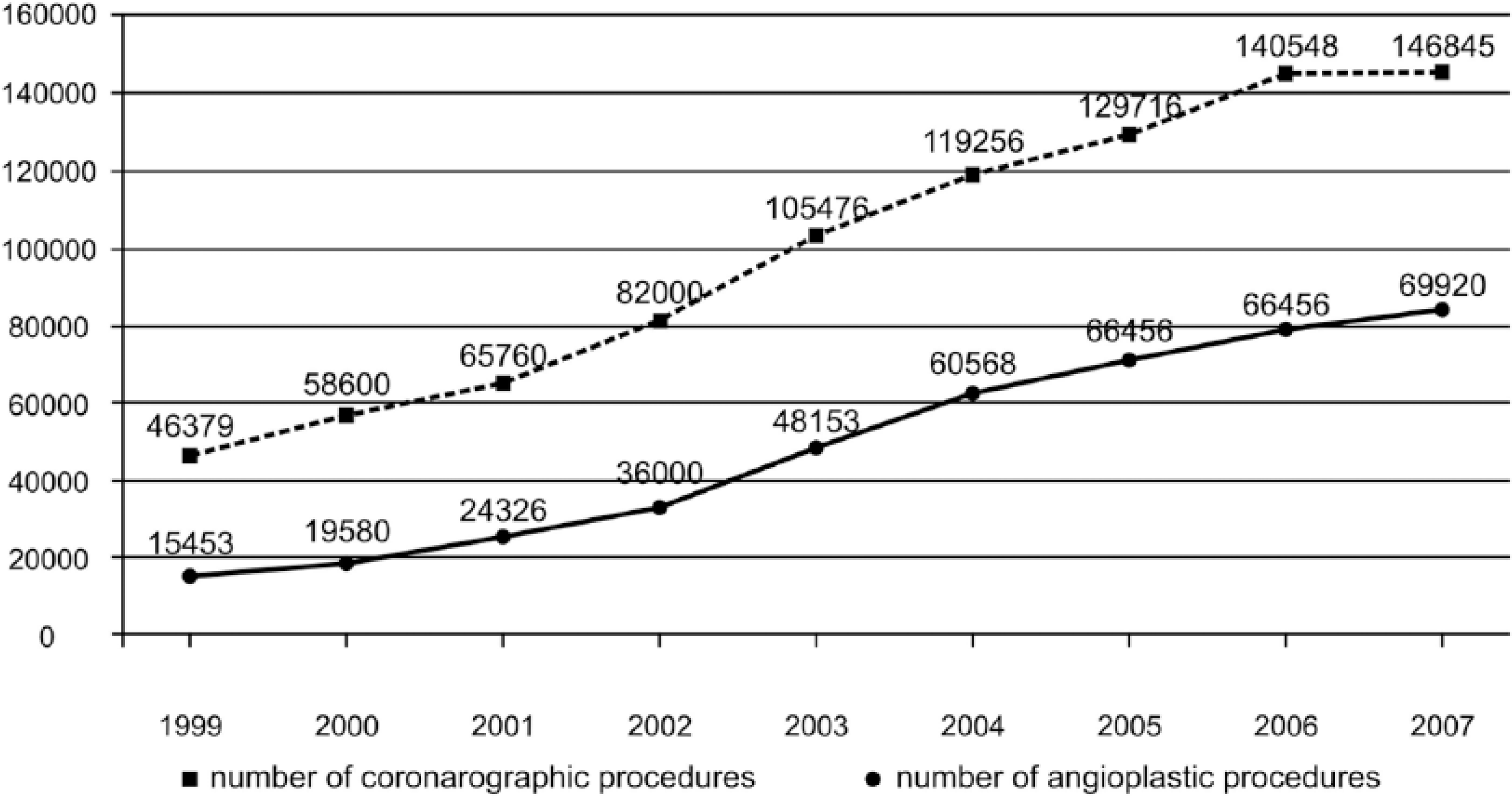
Number of invasive cardiology procedures in Poland (1999-2007).
Policy Screening
Health care including public health action is financed and managed in Poland on central, regional, and local levels. The crucial targets of health policy are provided by the Ministry of Health. The National Health Fund is the main public provider of health care procedures and plays a key role in health care system management.
Poor health outcomes of the Polish population at the beginning of the 1990s highlighted the demand of policy makers for the implementation of various health promotion programs, legal acts, local strategies, and more active public health policy.
Health promotion programs
In 1995, National Health Programme 1996-2005 was established, 46 based on WHO strategy Health for All in 2000, whereas the main objective was to decrease premature deaths from CVD. Most targets were continued in the second National Health Programme 2007-2015. 47 The main goal of National Programme for Cardiovascular Diseases Treatment and Prophylaxis 2003-2005 (POLKARD—the first edition) was to continue cardiovascular death rate reduction in Poland, which was achieved by actions started by National Programme of Heart Protection (1993-2001). The main objective of the second edition of Polkard programme 2006-2008 was to maintain the 3% decrease in CVD death rate every year over the 10-year period from 2003 to 2012. 48 The POLKARD program was based on EU Council recommendations.49,50 Among the main POLKARD targets, the following were mentioned: cholesterol level reduction below 5 mmol/L, blood tension level of population older than 65 years below 140/90 mmHg, tobacco consumption level reduction 1% per year, and social access to health promotion and health prevention activities with special focus on obesity, type 2 diabetes, and heart inefficiency.
Two other vital CVD prophylaxis programs were financed by the National Health Fund (NHF): Cardiovascular Diseases Prophylaxis Programme and Prophylaxis Programme for Tobacco Related Diseases. They were managed on the regional level by NHF divisions. 51
National Programme for Preventing Overweight, Obesity and Chronic Non-communicable Diseases by Increasing Nutrition Quality and Physical Activity 2007-2011 52 was introduced to improve early prevention of overweight and obesity to reduce the incidence proportion on chronic diseases, it was based on the global strategy on diet, physical, activity and health 53 and supported the European Commission initiative: “Promoting healthy diets and physical activity: a European dimension for the prevention of overweight, obesity and chronic diseases.” 54
National Programme for Prevention of Alcohol Related Problems 2006-2010, established by the Ministry of Health, was a response to the increasing role of social degradation as an effect of alcohol abuse, and it was managed on 3 levels. 55
Legal acts
The Act on Physical Culture defined the activity of central and local governments, non-public associations, and other organizations in the aspects of physical culture, sport, and rehabilitation. 56 The Act on Physical Culture was amended by the Act on Sport. 57
Due to the Act on Upbringing in Sobriety and Counter-acting Alcoholism, central and local authorities were obliged to take actions that would reduce the level and structure of alcohol consumption. 58
Poland was the first Central European country that introduced a comprehensive tobacco control program in 1995 (Act of November 9, 1995). New anti-tobacco law (Act of April 8, 2010) forbids smoking in public indoor spaces. Advertisement and tobacco companies sponsoring is also limited by current anti-tobacco regulations. 59
Discussion
Effective public health policy means translating scientific research into policy and practice. The RAPID study is one of the first to develop methodology for the “full chain” process of policy risk assessment and provide policy makers with standardized guidance. Accountability for the health impact of policies and programs and legitimization of the decisions of policy makers based on research evidence has become one of the key questions nowadays in the decision-making process of European countries as in EU public health strategy. If policy can achieve reductions in human exposing, the potential health benefits may therefore be essential.
The Polish experiences provide the examples that reveal health benefits following legislation and health policy to limit health risk exposure and to improve the effectiveness of health system. Implemented policy has led to appreciable lowering prevalence of smoking and physical inactivity, to change of the pattern of consumed alcohol, and dietary changes, as well as led to improvements in evidence-based clinical and medical treatments, what finally contributed to decrease in blood pressure and total cholesterol levels in men and in women. Therefore, consistent implementation of a range of policies could result in significant improvement of health status of population. The Polish data sources in the period 1990-2010 reflect the positive trend in population health; a steady increase in life expectancy has been observed over the past 20 years. The sharp falls in standardized CVD mortality was the main cause. This spectacular decrease has many reasons, and it is hard to assess precisely how much of the recent fall could be explained by change in major determinants (lifestyle, health system). Some experts highlight the main contribution of lifestyle risk factor reduction to the CVD fall,23,33 the others the evidence-based treatment (pharmacotherapy, that is, statins, coronary angioplasty and angiography) and better rescue system. 45 The most recent research based on modeling study using the IMPACT model explains 37% of the decrease in the death rate from CHD in Poland, over past 20 years, attributable to evidence-based medical treatments and about 54% of the reduction was related to changes in lifestyle risk factors. 33 The same research confirms that among major risk factors, 15% of the observed decrease in CHD mortality was related to reduced smoking in men (negligible in women), and 10% was related with increased physical activity. A similar research, conducted in Western Europe and United States, provide the same trends.10,14,27,31,43 Generally, the benefits of changes in population-level risk factors were substantially larger than those from improvements in medical and clinical treatment.
The bottom-up policy risk assessment methodology seems to be a useful tool in identifying challenges involved in the analysis of risk factor reduction policies and in assessing how the health-related indicators have changed over time. However, although we present in this article only general consideration, pointing out the relationship between the health outcome and policy, this case study should deliver evidence to help strengthen the basic public health functions and objectives. Our findings suggest the impact of the policy on chosen risk factor reduction, like tobacco and alcohol consumption, diet, new medical technologies, and others in CVD mortality decrease, which directly affect life expectancy prolongation. The developed model for the assessment of population health impacts of a policy provides a great opportunity to systematize both the assessment process and even more importantly the process of putting new regulations on the agenda of national legislation. A new regulation always starts a chain reaction in influencing key determinants of health, risk factors, and in the last step, health of population. As the determinants of health are rather on population and structural levels, policies can carefully plan how, by which means, and for what funding will they change the status of determinants of health. Risk factors are in contrary often in reach of individuals within a population, so intervention can be planned both at population and individual levels. Another significant issue to discuss is time; realization of the impact of policies may need time. The description of the probable latency of effects is important information that should be considered in the decision-making process. There is a latency period between the planning and implementation of a policy, as well as a lag phase between policy implementation and development of health effects.
Supporting the implementation of national legal instruments to control population health risk exposure seems very important from the public health policy point of view as also providing guidelines and evidence. It also requires a broad, cross-sectoral and multi-sector engagement. A bottom-up policy health risk assessment model can be one of the main tools in this process, providing harmonized guidance how to seek and evidence-based information, which could serve policy makers and also be accessible by the media and the general public.
Conclusions
Better health outcomes of population could be achieved mainly by the implementation of health promotion programs, effective legislation (ie, tax regulations, smoking cessation support, limitations), and active public health policy on central, regional, and local levels. The implementation of professional programs for the prevention and management of diseases is a crucial element of effective health policy. New technologies and evidence-based guideline implementation for medical treatment and primary care are necessary. Health promotion and education activity, especially addressed to the most vulnerable groups of society, to reduce the health and social inequalities should be one of key targets for decision makers. Bottom-up policy risk assessment model may provide policy makers with an effective approach to population health management, in evaluating policies and to determine their potential, current and future impacts on public health. The general scheme of relations analyzed in this case study is presented in Figure 8. Causal pathway diagrams are also a visual way of presenting the multi-causal relationships between a policy, program or intervention, and health effects.

Bottom-up full chain risk assessment model.
Limitation of the Study
The limitation associated with our study is related to qualitative research only. We took into consideration health reports, statistical yearbooks, scientific journal publications, and legal acts concerning health status of the Polish population in terms of CVDs and their risk factors (eg, tobacco policy, alcohol policy). There were not applied any statistical or mathematical models, which would allow to measure the direct impact of the legal acts on the value of CVD mortality decrease. There were not taken into consideration the possible methodological differences between reports, which were used in this case study. It is important to notice that the recent fall of CVD mortality has many reasons, and some of them were not included in the study, for example, the potential contribution of environmental risk factors. Another significant issue to discuss is time; realization of the impact of policies may need time. The description of the probable latency of health effects should be considered in the decision-making process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the European Commission, Directorate for Health and Consumers via Executive Agency for Health and Consumers, 2nd Community Action Plan on Public Health Program (grant agreement 20081105), project “Risk Assessment From Policy to Impact Dimension” (RAPID), 2009-2012.