
Abstract
The expansion of Medicaid coverage under the Affordable Care Act offers the potential for significant increases in health care access, use, and spending for vulnerable nonelderly adults who are uninsured. Using pooled data from the Medical Expenditure Panel Survey, this study estimates the potential effects of Medicaid, controlling for individual and local community characteristics. Our findings project significant gains in health care access and use for uninsured adults who enroll in Medicaid coverage and have chronic health conditions and mental health conditions. With that increased use, annual per capita health care spending for those newly insured individuals (excluding out-of-pocket spending) is projected to grow from $2,677 to $6,370 in 2013 dollars, while their out-of-pocket spending would drop by $921. It is expected that these increases in spending would be offset at least in part by reductions in uncompensated care and charity care.
While many Americans will benefit from national health reform, low-income uninsured adults are among those with the most to gain since many will become newly eligible for coverage under the Medicaid program. At the heart of the Affordable Care Act (ACA) of 2010 is the option for states to enact a major expansion of Medicaid eligibility in 2014, covering most adults under age sixty-five with incomes up to 133 percent of the federal poverty level (FPL) or up to 138 percent, including a standard 5 percent “income disregard.” In this paper, we explore how that Medicaid expansion might affect health care use and spending for some of the most vulnerable uninsured adults—low-income adults with chronic health conditions. We also conduct analyses on a subset of adults with chronic health conditions: those with mental health conditions.
The prevalence of chronic conditions, including mental health conditions, is high among uninsured adults. Recent national statistics indicate that approximately one in three uninsured adults has a chronic health condition, and approximately one in nine has a mental health condition or a substance abuse disorder or both. 1 Since prevalence rates are similar or higher for uninsured individuals with incomes below poverty, it is likely that substantial numbers of those adults who will be newly eligible under the ACA’s Medicaid expansion will have a chronic condition, with many also having a mental health condition. Individuals with a chronic condition tend to have high medical care needs and, consequently, account for a disproportionate share of health care spending (Anderson 2010; Druss et al. 2001).
For those who are eligible for coverage, the Medicaid program covers a comprehensive range of benefits addressing physical and mental health needs, including coverage for acute care, ambulatory care, and prescription drugs. By contrast, the health care safety net for the uninsured is a patched-together system; many individuals rely on community-based clinics and emergency departments (EDs) for their care, or they delay care or get no health care services at all (Kaiser Family Foundation 2012b). By providing access to a broad range of health services at no cost or low cost, we would expect the expansion of eligibility for Medicaid to yield improvements in access to, and use of care for low-income uninsured adults, as well as in better health (Hadley 2007; Sommers, Baicker, and Epstein 2012).
This paper provides insight into how the Medicaid expansion under the ACA will likely improve access to health care for low-income uninsured adults with chronic conditions. Building on previous research (Coughlin, Long, and Shen 2005; Hadley and Holahan 2003–2004; Kaiser Family Foundation 2012a; Ku and Broaddus 2008), we use data from the Medical Expenditure Panel Survey (MEPS) to compare health care access, use, and spending for low-income uninsured adults with chronic conditions overall and those with mental health conditions to their counterparts with Medicaid coverage. We focus on the potential effects of Medicaid on the beneficiaries’ access to various types of health care services and prescription drugs, their level of health care use, and spending on their health care, including the individuals’ out-of-pocket health care spending by the individuals. In the analysis, we control for a wide array of factors that influence health care use and spending (such as individual and community characteristics) in an effort to isolate the effects of Medicaid coverage from other factors.
Data
The primary data source for this paper is the 2003 to 2009 Household Component of the MEPS, a nationally representative survey of the U.S. civilian, noninstitutionalized population sponsored by the Agency for Healthcare Research and Quality (AHRQ) (AHRQ 2004; Cohen 1997). Our analytical sample is low-income adults ages nineteen to sixty-four64 (hereafter referred to as “adults”) who had full-year Medicaid coverage or were uninsured a full year 2 and had one or more chronic health conditions. We exclude noncitizens since they are not generally eligible for Medicaid coverage and pregnant women because they already are categorically eligible for coverage. We also exclude Medicaid enrollees who have “dual” coverage through Medicare. We focus on a low-income population, defined as those with family incomes at or below 138 percent of the FPL because this is the new Medicaid eligibility standard to be implemented for adults under the ACA. 3
Identifying Chronic Health Conditions
To identify chronic conditions, we first identify conditions listed in the MEPS “medical conditions” files that satisfy at least one of the following criteria: (1) The condition is reported by the individual as the reason for using health services (e.g., hospital inpatient stay, office or outpatient visit), (2) the condition is reported as the reason for one or more episodes of disability days, or (3) the condition is reported as “bothering” the person during the survey reference period (AHRQ 2011). Chronic conditions are defined as a physical or mental health condition that generally lasts at least one year and results in a limitation of self-care, independent living, and social interactions or the need for ongoing intervention with medical products, services, and special equipment. To identify these conditions, we use the Chronic Condition Indicator (CCI) tool developed as part of the Healthcare Cost and Utilization Project (HCUP 2011). 4 Due to the confidential nature of the detailed condition data used (the fully specified International Classification of Diseases–Ninth Revision [ICD-9] codes), access is available only within a restricted Data Center. We include individuals with one or more chronic conditions in our analytical sample.
Among the low-income adults in our sample, Medicaid beneficiaries were much more likely than the uninsured to have one or more chronic health conditions (70.6 percent vs. 40.1 percent). In part, this reflects the availability of Medicaid coverage for individuals who qualify for the Supplemental Security Income (SSI) program, which provides cash assistance to severely disabled and aged low-income individuals.
Because the identification of adults with chronic conditions is based on their health care use over the past year, it is possible that we have underestimated the share of full-year uninsured adults with such conditions given their lower levels of health care use. To test the sensitivity of our findings to the definition of the sample, we estimated the models using an alternative definition of chronic conditions based on the individual’s report of ever having been diagnosed with any of a specific list of chronic conditions, including diabetes, asthma, high blood pressure, heart disease (e.g., coronary heart disease, angina, or myocardial infarction), stroke, emphysema, arthritis, joint pain, or bronchitis. This alternative definition of chronic conditions is available for a less comprehensive list of conditions than the definition based on coding used in our main results, resulting in a slightly smaller sample of individuals with a chronic condition (5,853 vs. 6,453). The estimates based on the alternate sample were similar to those of the core analysis reported here, although the magnitudes of the estimates and the Medicaid-uninsured differences tended to be smaller.
For the component of the analysis that focuses on the subset of adults with a mental health condition, we identified individuals with a mental health-related condition using a strategy similar to that of researchers at the U.S. Department of Health and Human Services Substance Abuse and Mental Health Services Administration (SAMHSA) (Buck, Teich, and Miller 2003). That methodology uses selected ICD-9 codes (including schizophrenia, major depression, stress and adjustment reactions, and other psychoses) to identify individuals who receive treatment for a mental health condition, as shown in Table 1. In this analysis, we exclude codes associated with substance abuse disorders. In our sample of low-income adults, 37.1 percent of Medicaid beneficiaries and 16.6 percent of uninsured adults are identified as having a mental-health-related condition.
Diagnosis Codes to Identify the Population with Mental Health Conditions.
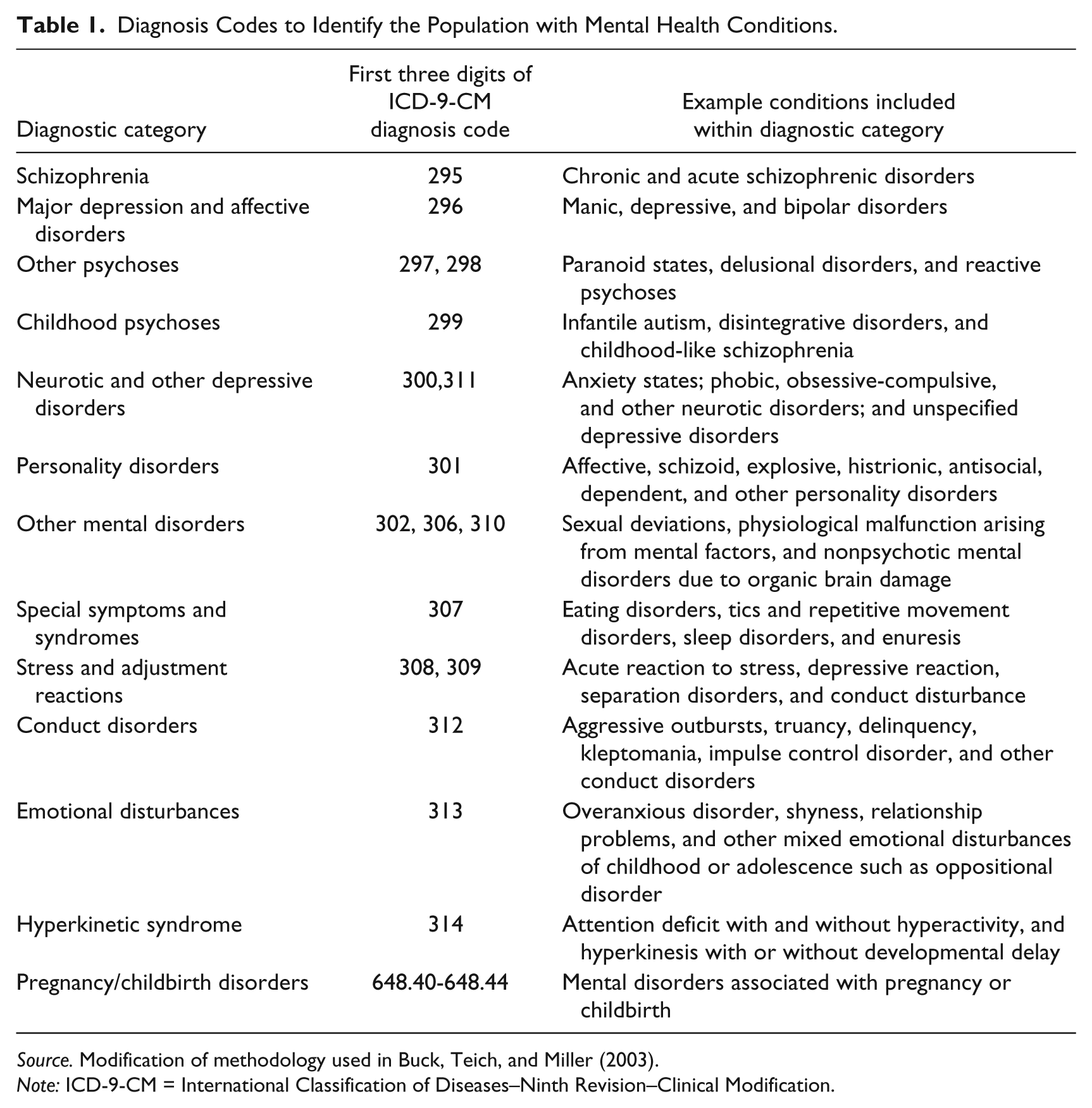
Source. Modification of methodology used in Buck, Teich, and Miller (2003).
Note: ICD-9-CM = International Classification of Diseases–Ninth Revision–Clinical Modification.
Similar to the sensitivity test described previously for the definition of chronic conditions, we tested the sensitivity of our findings to alternative definitions of mental health conditions based on self-reported information. The alternative definition limited the sample to those who were in the lower quartile of the Mental Component Summary (MCS), which has been found to be less dependent on the contemporaneous use of health care than other measures of mental health status (Zuvekas and Fleishman 2008), or who reported fair or poor mental health status. The alternative definition yielded a similar sample size of people with a mental health condition compared with the sample used in the core analysis (2,793 vs. 2,846). The estimates produced under this alternative definition were similar to those of the core analysis, although generally smaller in magnitude.
Outcome Measures
The primary focus of the analysis is on health care use and spending, supplemented by some indicators of health care access. The health care access measures include whether the individual had a usual source of care (other than the ED) and whether the individual reported unmet need for medical care, tests, or treatments, or unmet need for prescription medicines. The measures of health care use and expenditures are for specific types of care—hospital inpatient stays, outpatient ED visits, 5 office or outpatient visits, general practitioner visits, specialist visits, and prescription drugs. 6 The average number of health care visits is an outcome measure for office or outpatient visits, general practitioner visits, and specialist visits. Due to the infrequency of inpatient stays and outpatient ED visits, we measure the share with “more than one” stay or visit rather than the average number of stays or visits for these types of care.
For Medicaid enrollees, health care spending includes direct payments by Medicaid to health care providers; for uninsured individuals, health care spending represents health care costs associated with uncollected liability, bad debt, and charitable care, unless provided by a public clinic or hospital; for both types of individuals, these spending estimates do not include out-of-pocket spending by the patient. 7 Out-of-pocket spending includes direct payments by individuals to health care providers; it does not include spending on health insurance premiums. 8 To provide benchmarks for evaluating costs, health care spending is inflated to 2012 dollars using the historical medical care index from the Consumer Price Index (CPI) (Bureau of Labor Statistics 2013) and to 2013 using per capita growth rates from the national health spending projections from the Centers for Medicare and Medicaid Services (CMS 2012).
We supplement the MEPS data with characteristics of the local (county or county equivalent) health care market from the Area Resource File (ARF) compiled by the Health Resources and Services Administration. The geographic variables include measures of provider supply, health care costs, and local demand for health services. 9 Due to the confidential nature of geographic identifiers, access to the MEPS files merged with geographic data are available only within a restricted Data Center.
Method
We rely on both descriptive and multivariate methods to compare health care access, use, and expenditures for adults with Medicaid and those with no insurance. In the multivariate analysis, we control for individual and family demographic and socioeconomic characteristics; the individual’s physical and mental health, health conditions, and limitations; and characteristics of the health care market in his or her local community. The variables included in the regression models are listed in Table 2. As has been shown elsewhere, low-income Medicaid beneficiaries are significantly different from the uninsured on a host of demographic, socioeconomic, and health dimensions. 10 This holds true for adults with chronic conditions and those with mental health conditions as well (Table 2). Among low-income adults with at least one chronic condition, Medicaid beneficiaries reported poorer physical and mental health, more limitations, and more comorbidities than did uninsured adults. For example, over two-thirds (67.1 percent) of Medicaid adults with a chronic condition reported a health limitation as compared with about one-half (49.7 percent) of the uninsured. We observed similar patterns when looking within the population that has a chronic condition to those with a mental health condition. For this population, more than three-quarters (75.6 percent) of Medicaid adults reported a health limitation as compared with about two-fifths (58.9 percent) of the uninsured adults. Given these significant differences, we focus primarily on the regression-adjusted comparisons in presenting the findings.
Variables Included in the Multivariate Analysis: Characteristics of Low-Income Full-year Uninsured Adults and Full-year Medicaid Adults with Chronic Conditions and Mental Health Conditions, 2003–2009.

Source: 2003–2009 Medical Expenditure Panel Survey (MEPS).
Note: SF-12 = Short-Form 12; AHRQ = Agency for Healthcare Research and Quality.Family characteristics such as income are defined based on health insurance eligibility units as provided by the AHRQ. For details on the methods, see text.
Significantly different from zero at the .10 level. **Significantly different from zero at the .05 level. ***Significantly different from zero at the .01 level, two-tailed test.
In estimating the multivariate models, binary outcome variables, such as the probability of a health care visit during the year, were estimated using logit regression. Counts for outcome variables, such as the number of office/outpatient visits during the year, were estimated using zero-inflated negative binomial (ZINB) models to account for the presence of a large share of the sample with zero values and the skewness (a heavy right-hand tail) of the distribution (Buntin and Zaslavsky 2004; Zuvekas and Cohen 2007).
Expenditures for health care during the year were estimated using two-part models to account for both the large share of zero values and the skewness of the distribution. In the first part of the model, the use of any health care was estimated using logit regression, and in the second part, the level of expenditures conditional on use was estimated with generalized linear models (GLMs) in which we specify a gamma regression model with a log link. The specification of the two-part GLM spending models was determined as follows. The link function, which characterizes how a linear combination of the explanatory variables relates to the prediction on the original scale, was determined using a Box-Cox test. The functional family was determined using the modified Park test. The fit of the selected link and family were tested using multiple diagnostics: the Pregibon link test, the Ramsey reset test, and the Hosmer–Lemeshow test. In cases where the Box-Cox test or Park test was inconclusive, we compared the fit of candidate links and families using the remaining statistics. In all cases, we determined that a log link function was most appropriate. For the family, the gamma distribution was found to be generally superior to other family distributions. In a few cases when another family was found to be superior, the gamma distribution produced similar results. We estimated all models with the same specification so that results are comparable across services and component spending aggregates to total spending.
In presenting the findings from the analysis, we focus on the average treatment effect of being insured by Medicaid relative to being uninsured. To compute the average treatment effect, we used the estimates from the regression models to first generate a predicted value for each outcome under the assumption that the full analytical sample is enrolled in Medicaid and then under the assumption that the full analytical sample is uninsured. Given the focus of the paper on the implications of the Medicaid expansion for uninsured adults, the main findings from the multivariate analyses are presented as the average marginal effect of Medicaid coverage relative to being uninsured for the sample of uninsured adults with a chronic condition overall and for those with a mental health condition.
The calculation of the average marginal treatment effects varies across the outcomes with the estimation method. For outcomes based on binary and count models, average marginal effects were calculated using STATA’s margins command to compute discrete first-differences, producing the average “treatment” effect of having Medicaid coverage among the sample of those currently uninsured. For outcomes from the spending models, which comprise two stages and could not be calculated using the margins command, we used our modeled parameter estimates to estimate the expected value of spending for each observation based on its values for the predictor variables (including specified treatment). We then computed the standard error of the predicted change of total health care expenditures using the method of balance and repeated replications (BRR) as the root mean square error of the replicate weight estimates from the base weight estimates. Assuming normality of the estimates, we computed the p-value corresponding to the ratio of estimated effect to computed standard error.
All analyses were weighted using the MEPS sample weights and adjusted for the complex design of the survey. The models were estimated using STATA 12 (StataCorp 2011). Unless otherwise noted, all the differences discussed in the text are significant at p = .05 or better.
Results
Medicaid-Uninsured Differences in Estimates of Health Care Access, Use, and Spending
Among low-income adults with chronic conditions, Medicaid beneficiaries had much better health care access and higher use than did those who were uninsured based on simple differences (Table 3). For example, Medicaid adults with a chronic condition were more likely than those who were uninsured to have a usual source of care (89.3 percent vs. 58.4 percent) and less likely to report unmet need for medical care (6.9 percent vs. 23.3 percent) or for prescription drugs (4.6 percent vs. 16.6 percent). Further, Medicaid beneficiaries were more likely to report using all types of care. For example, the Medicaid beneficiaries had an average of 12.0 office/outpatient visits and 3.8 specialist visits, compared with 4.4 and 1.2 visits, respectively, for the uninsured.
Unadjusted and Regression-adjusted Comparison of Access, Service Use, and Spending for Low-income Uninsured and Medicaid Adults with Chronic Conditions, 2003–2009.
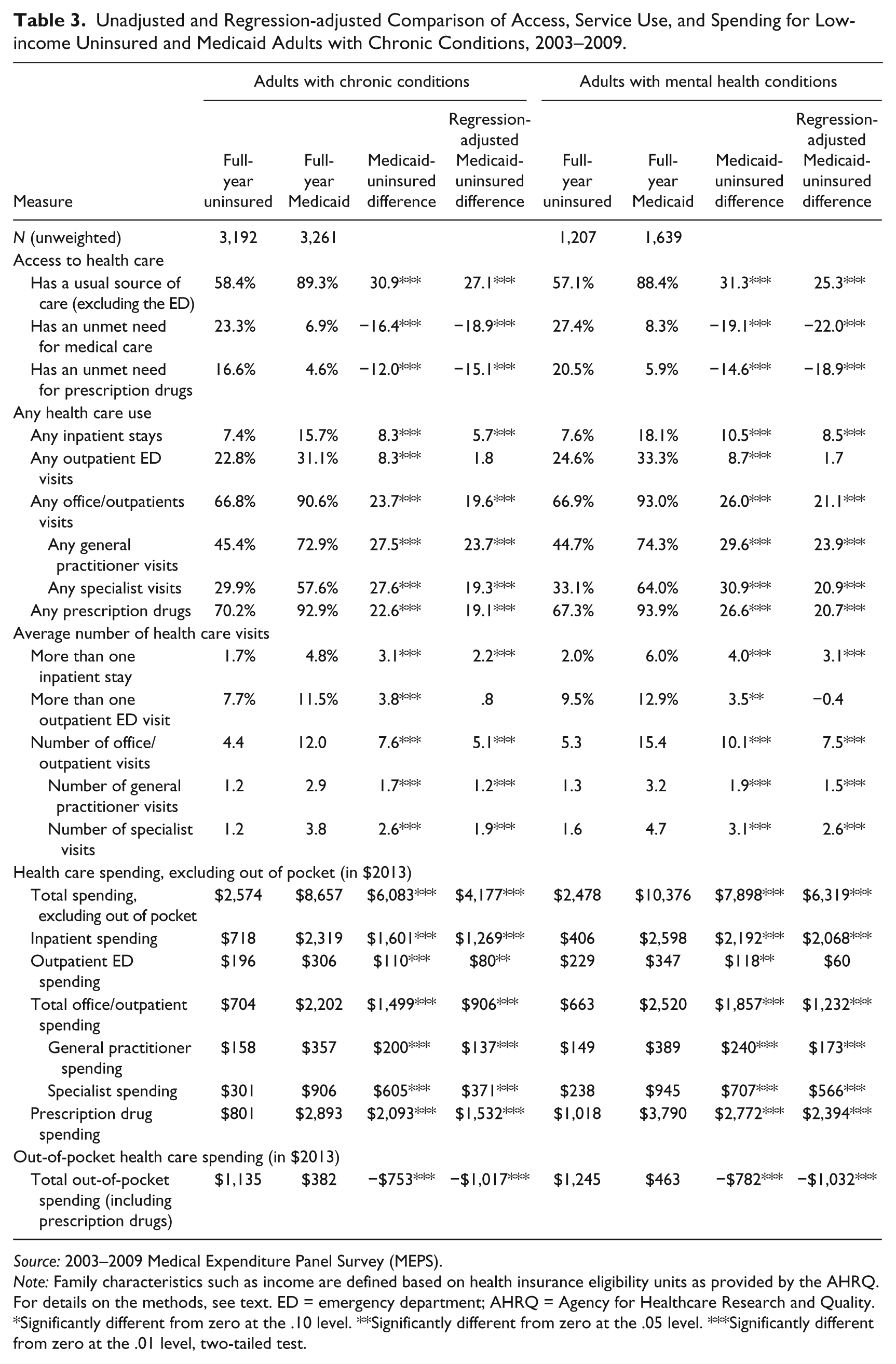
Source: 2003–2009 Medical Expenditure Panel Survey (MEPS).
Note: Family characteristics such as income are defined based on health insurance eligibility units as provided by the AHRQ. For details on the methods, see text. ED = emergency department; AHRQ = Agency for Healthcare Research and Quality.
Significantly different from zero at the .10 level. **Significantly different from zero at the .05 level. ***Significantly different from zero at the .01 level, two-tailed test.
The higher levels of health care use by Medicaid beneficiaries with chronic conditions translated into higher health care spending. Among adults with a chronic condition, total health care spending (excluding out-of-pocket spending) was $6,083 higher for Medicaid adults than spending for the uninsured ($8,657 vs. $2,574). This difference arose from higher spending for Medicaid beneficiaries on several types of services, most notably $2,093 more in spending on prescription drugs, $1,601 more in spending on inpatient stays, and $605 more in specialist spending. In contrast, total out-of-pocket spending was far lower for Medicaid beneficiaries than it was for the uninsured ($382 vs. $1,135).
The differences in health care access, use, and spending between Medicaid adults and uninsured adults with chronic conditions overall are echoed in the findings for the subset with a mental health condition. In particular, the differences in spending were even more pronounced for those with mental health conditions. Total spending (excluding out-of-pocket spending) for Medicaid beneficiaries was $10,376 as compared with $2,478 for the uninsured, with much of the difference driven by greater levels of spending under Medicaid for inpatient care ($2,192 higher), office/outpatient care ($1,857 higher), and prescription drugs ($2,772 higher).
Significant differences in health care access, use, and spending between Medicaid beneficiaries and the uninsured persist for nearly all outcomes after controlling for differences in the characteristics of the Medicaid and uninsured adults in the multivariate analyses. For example, after controlling for individual and local area characteristics, total spending (excluding out-of-pocket spending) was $4,177 higher for Medicaid beneficiaries, compared with the uninsured adults with a chronic condition; among adults with a mental health condition, it was $6,319 higher under Medicaid relative to being uninsured. Controlling for the differences between Medicaid beneficiaries and the uninsured adults has the strongest impact on ED use and spending, with the simple Medicaid-uninsured differences generally small and not statistically significant based on the regression-adjusted estimates.
In the next section, we use the estimates from the multivariate models to project the potential gains in health care access, use, and spending from extending Medicaid coverage to low-income uninsured adults with chronic conditions overall and more specifically to those with mental health conditions.
Projected Gains in Health Care Access, Use, and Spending if Medicaid Coverage Is Extended to Low-income Uninsured Adults
Extending Medicaid coverage to low-income uninsured adults with a chronic condition is projected to lead to significant improvements in their access to health care and increases in their use of nearly all types of care, all else equal. It is predicted that gaining Medicaid coverage will increase by 28.6 percentage points (from 58.4 percent to 87.1 percent) the likelihood that they would have a usual source of care, and decrease by three-quarters the likelihood of having unmet health care needs (Table 4).
Regression-adjusted Estimates of the Projected Change in Health Care Access, Use, and Spending for Low-Income Uninsured Adults with Chronic Conditions Who Gain Medicaid Coverage.

Source: 2003–2009 Medical Expenditure Panel Survey (MEPS).
Note: Family characteristics such as income are defined based on health insurance eligibility units as provided by the AHRQ. For details on the methods, see text. ED = emergency department; AHRQ = Agency for Healthcare Research and Quality.
Significantly different from zero at the .10 level. **Significantly different from zero at the .05 level. ***Significantly different from zero at the .01 level, two-tailed test.
The shift to Medicaid also would be associated with considerable increases in use of care, including inpatient stays, office/outpatient visits, and prescription drugs. The analysis suggests a shift to Medicaid would result in no significant changes in outpatient ED visits for the previously uninsured. Nearly one-quarter likely would still use the ED in a given year. However, under Medicaid, the share of the previously uninsured adults with an inpatient stay would increase from 7.4 percent to 15.7 percent, and the share with more than one inpatient stay would increase from 1.7 percent to 4.8 percent. Similarly, the share of uninsured adults with an office/outpatient visit is expected to increase from 66.7 percent to 88.0 percent under Medicaid, with the average number of office/outpatient visits over the year projected to increase from 4.5 to 8.9.
The higher levels of health care use projected with the expansion of Medicaid coverage would translate into higher levels of health care spending, with total per capita health care spending (excluding out-of-pocket spending) increasing from $2,677 when uninsured to $6,370 when covered by Medicaid—an increase of $3,693. At the same time, out-of-pocket spending would decline for those who were uninsured with the gain in Medicaid coverage, falling from $1,214 to $293 a year.
The projected gains under Medicaid for the subset of the uninsured adults with a mental health condition would also be large. Health care access and use would both increase by significant margins. In particular, office/outpatient visits would more than double with the switch to Medicaid, with the average number of office/outpatient visits over the year increasing from 5.4 to 12.0 for these adults. However, the analysis suggests that there would be no significant changes in outpatient ED visits for this sample of uninsured with a shift to Medicaid.
With Medicaid coverage, health care spending for the uninsured adults with mental health conditions would increase significantly. Overall, total spending per capita would increase from $2,536 to $8,116 per year, up by $5,580. The largest gains would be in inpatient spending ($1,825 higher) and prescription drug spending ($2,197 higher).
The Change in Aggregate Spending for Those Currently Uninsured if They Gained Medicaid Coverage
For the estimated population in 2009 of 4.7 million low-income full-year uninsured adults with a chronic condition in our sample, aggregate total spending (excluding out-of-pocket spending) was $12.1 billion (in 2013 dollars), the largest components of which were $3.4 billion for inpatient spending, $3.3 billion for office/outpatient spending, and $3.7 billion for prescription drug spending (Table 5). Given that these were low-income uninsured adults, the bulk of those costs was likely borne by the health care system at large or provided in the form of uncompensated care (e.g., care provided in federally qualified health centers or through charity care at hospitals). If all of those low-income adults were eligible for and enrolled in Medicaid under the 2014 ACA Medicaid expansion, we project that their total health care spending (excluding out-of-pocket spending) would increase by $17.8 billion. The largest components of that new spending are projected to be $5.0 billion for inpatient spending, $3.9 billion for office/outpatient spending, and $6.5 billion for prescription drug spending. While total Medicaid program costs would increase with the shift of the uninsured to Medicaid, the nation’s total health care bill would not increase by nearly as much since some of those costs would be offset by the reduction in payments from other sources for uninsured adults.
Projected Aggregate Change in Health Care Spending from Extending Medicaid Coverage to Full-year Uninsured Low-Income Adults with Chronic Conditions.
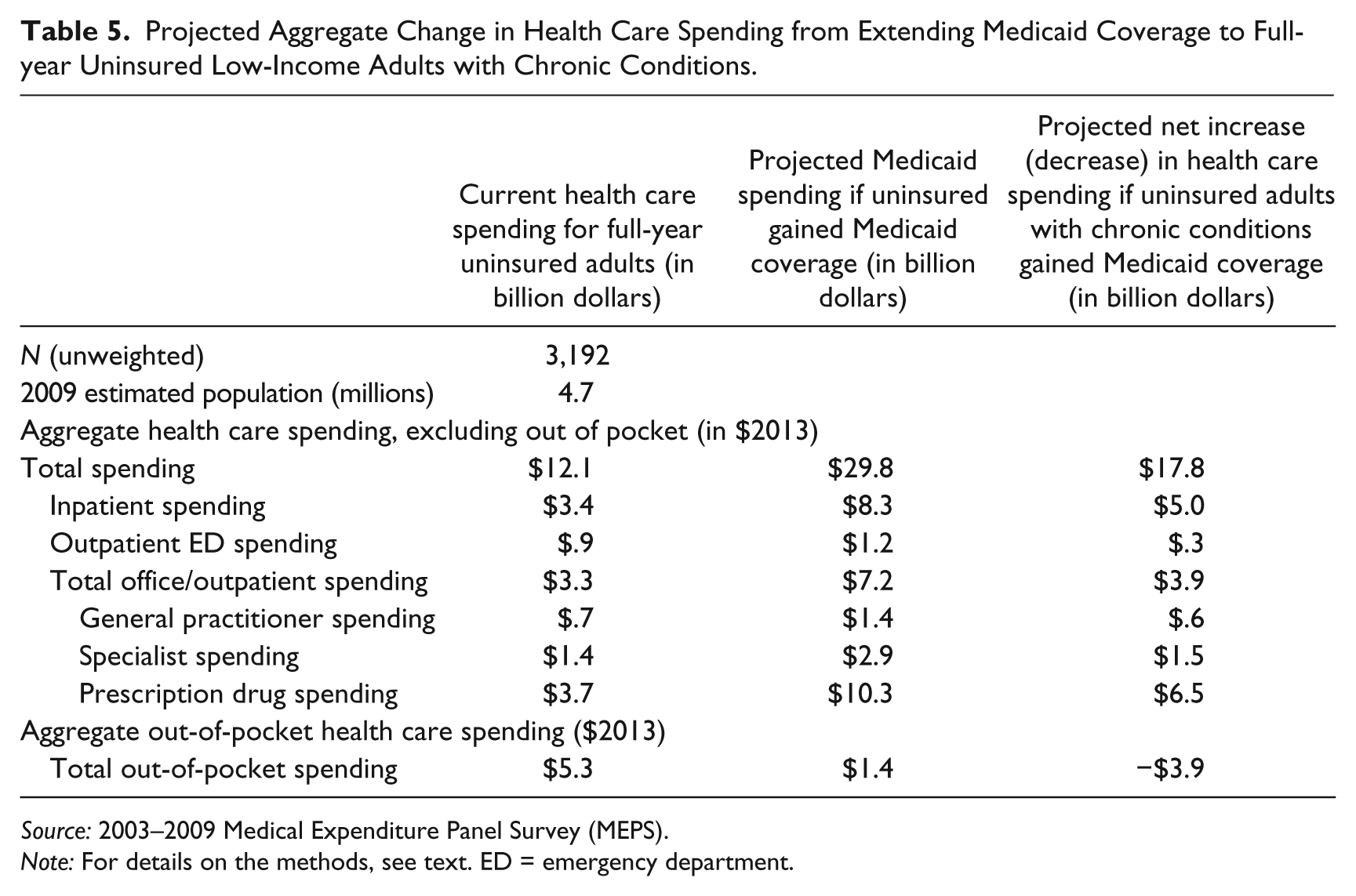
Source: 2003–2009 Medical Expenditure Panel Survey (MEPS).
Note: For details on the methods, see text. ED = emergency department.
Limitations
There are several limitations to the study. First, our focus on full-year coverage provides the most comparable experiences across health insurance statuses in terms of health care access, use, and costs, but this focus may limit the generalizability of our findings to the health care access, use, and costs of the full population of individuals who do not have consistent health insurance coverage over the year.
Second, we examined the potential for bias in the findings due to the possible endogeneity of Medicaid enrollment. This type of endogeneity bias could overstate the effect of Medicaid enrollment on service use and spending to the extent that uninsured Medicaid-eligible individuals who expect to use services and incur spending have an increased incentive to enroll in Medicaid. Due to the lack of available instruments, we used a method similar to that employed by Currie and Gruber (1996). Using each state’s Medicaid eligibility rules, we estimated the share of the national population within the applicable group (i.e., parents and childless adults) who would be eligible for Medicaid in each state and the District of Columbia. The 2011 Annual Social and Economic Supplement (ASEC) of the Current Population Survey (CPS) and Medicaid eligibility rules available through Kaiser State Health Facts were used to calculate the state eligibility shares. This eligibility measure is highly correlated with actual enrollment but independent of other characteristics of the individuals, and therefore likely exogenous to the individual’s enrollment decision. For this evaluation, we estimated models that replaced the enrollment status indicator with an applicable Medicaid-eligibility percentage. For models of access to care, models of the use of any health care, and some models of spending, this method produced similar results to those presented.
Third, the sample frame is limited to a community-based population according to residential addresses. Thus, the study sample does not include individuals who were living in nursing homes or the homeless who often have chronic conditions, including mental health conditions. However, the study population includes those most likely to obtain Medicaid coverage under national health reform.
Lastly, our ability to control for the severity of the health conditions among those with a chronic condition is limited, since our data do not include measures of severity of health conditions. Medicaid beneficiaries may have more severe health conditions than the uninsured, perhaps reflecting eligibility for Medicaid via the SSI and Social Security Disability Insurance (SSDI) programs due to disability. 11 As a result, our control variables may understate the severity of health conditions for Medicaid beneficiaries relative to the uninsured. To the extent that occurs, the impacts on uninsured adults of gaining Medicaid coverage would likely be overstated. As one way to examine this issue, we looked at the extent to which the analysis was affected by those with SSI or SSDI status. We found that these adults represent a sizable share of the Medicaid population (7.9 percent of the sample with chronic conditions) and even more of the uninsured population (33.5 percent), but that results were not qualitatively different after removing these observations.
Discussion
As is true for the Medicaid population overall (Coughlin et al. 2013), we find that low-income adults with chronic conditions who are covered by Medicaid have much better access to care than do their uninsured counterparts. They are significantly more likely to use health care services, including ambulatory care services and inpatient care, and significantly less likely to have unmet need for health care. This holds true for adults with chronic conditions overall and for the subset of those adults with mental health conditions.
Another clear benefit of Medicaid coverage for low-income adults is its limited cost sharing. Low-income uninsured adults with chronic conditions incurred out-of-pocket costs that were more than three times higher than those incurred by Medicaid beneficiaries. Across all health care services, out-of-pocket spending by the uninsured averaged $1,135 in 2013 dollars. Given that the study population was adults with family incomes less than 138 percent of FPL, this level of out-of-pocket spending likely represents a substantial share of income. For example, for a single person with income equal to the poverty level in 2013, this would represent 9.9 percent of their annual income (Federal Register 2013).
As these findings demonstrate, extending Medicaid coverage to low-income uninsured adults with chronic conditions under the ACA offers the potential for significant gains in health care access and increases in health care use, as well as improved protection from high health care costs and better management of health care costs. For example, gaining Medicaid coverage is predicted to increase by 28.6 percentage points (from 58.4 percent to 87.1 percent) the likelihood that they would have a usual source of care by while decreasing by three-quarters the likelihood of unmet health care needs. Health care use and spending would increase, while out-of-pocket spending would decline for those getting Medicaid coverage to $293 a year. Uninsured adults with chronic conditions rely on a wide range of health care services; as we show, that reliance would expand with the improved access to care through Medicaid coverage under the ACA. This would include higher levels of use of inpatient and ambulatory care services, as well as prescription drugs.
For both existing and new Medicaid enrollees with chronic conditions, states can take advantage of new opportunities for better coordination and management of health care through Medicaid “health homes” services in the ACA. These include support services such as care management and coordination, transitional care and follow-up, and referral to community and social support services (CMS 2010). In order to target the limited available funds, states should analyze which subpopulations of eligible Medicaid enrollees would be most likely to have better quality health care and improved outcomes as a result of participation in these new health homes, which are also intended to decrease average spending.
As expected, the expanded health care use by low-income uninsured adults with chronic conditions enrolled in Medicaid under the ACA would cost more. Currently, total aggregate spending (excluding out-of-pocket spending) is estimated to be $12.1 billion for the 4.7 million low-income full-year uninsured adults with a chronic condition in our sample. If all those adults were eligible for and enrolled in Medicaid in 2014 under the ACA, total aggregate spending for their health care (excluding out-of-pocket spending) would increase by $17.8 billion. Since many of these adults are likely to be newly eligible for Medicaid, the vast majority of the costs would be borne by the federal government under the ACA (Kenney et al. 2012). As a result, the projected spending increases have implications for the federal budget related to Medicaid programs and more limited implications for state budgets. Further, to the extent that current funding for the uninsured is paid for through state funds, the shift to Medicaid may lower state spending on uncompensated care.
As states move forward in implementing the Medicaid expansion under the ACA, they will, among other things, need to determine the benefit packages and provider networks for newly eligible adults. This paper shows that many of these individuals are likely to have chronic conditions requiring a complex mix of services and drugs from a variety of health care providers. It will be important to carefully weigh the design of plans to ensure that these vulnerable individuals can obtain the health care they need.
Footnotes
Acknowledgements
The research in this paper was conducted at the Center for Financing, Access, and Cost Trends (CFACT) Data Center, and the support of AHRQ is acknowledged. We are grateful to Ray Kuntz for facilitating our work at the CFACT Data Center. The authors thank Willard G. Manning and two anonymous reviewers for their helpful comments on an earlier version of the paper. We also thank Lokendra Phadera, Emily Lawton, and Elaine Grimm for their research assistance.
Authors’ Note
The views, results, and conclusions in this paper are those of the authors and do not indicate concurrence by AHRQ; the Department of Health and Human Services; the Urban Institute, its trustees or sponsors; or the Kaiser Commission on Medicaid and the Uninsured.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This research was completed as part of a project for the Kaiser Family Foundation’s Commission on Medicaid and the Uninsured.