
Abstract
There is a growing body of literature exploring how young people’s digital use shapes their mental health and well-being. However, very few studies have examined the ways in which digital use throughout adolescence shapes later outcomes, and even fewer studies have explained the precise pathways linking digital use to youth mental health. This study utilizes high-quality data from the 1998 birth cohort of the longitudinal Growing Up in Ireland (GUI) study (N = 5,077, 52% female) to examine: 1) how both current (age 20) and previous (ages 9, 13, 17/18) digital use behaviors are associated with depressive symptoms in young adulthood; 2) what pathways operate in the relationship between digital use and youth depressive symptoms; and 3) how associations and pathways between digital engagement and youth depressive symptoms differ by gender. Results show that higher levels of digital screen-time at age 20 (2+ hours daily) and consistent “heavy” digital usage throughout adolescence are associated with higher depressive symptoms at age 20. Further, path analyses reveal both direct and indirect paths of time spent online with higher depressive symptoms via poor sleep, decreased physical activity, decreased body-weight satisfaction, and low self-esteem. Finally, while associations between digital use and depressive symptoms are similar by gender, the explanatory pathways between previous adolescent digital use and depressive symptoms in young adulthood differ markedly between men and women. Overall, sleep, physical activity, self-concept and self-esteem are potential mediators driving the associations between digital use and youth depressive symptoms, while the pathways operating behind these processes differ by gender.
Introduction
Young people’s mental health has become and remains a major matter of interest in public health, and a principal concern to parents, physicians, and policymakers alike. The risk of developing psychiatric conditions such as anxiety and depression has been found to increase remarkably during adolescence, having a direct impact on individuals’ lifelong health and well-being (Kessler et al. 2007; Ludwig-Walz et al. 2022; Wilson & Dumornay, 2022). Although growing numbers of young people are experiencing poor mental health and depressive symptoms, what is driving these phenomena is complex and dynamic (Duffy et al., 2019; Keyes et al., 2019). Consequently, continued research aimed at understanding contemporary factors contributing to poor mental health in adolescents and young adults is of high importance to both public health and society at large.
A factor of particular contemporary concern is growing digital use amongst young people. As contemporary adolescents engage with increasingly ubiquitous and mobile digital devices that can present both risks and opportunities to mental health (Bohnert & Gracia, 2021; Goode et al., 2020; Livingstone et al., 2018), there is a present need to examine how and to what extent digital engagement might be associated with adolescent and young adult mental health outcomes. However, the literature on adolescent digital use and mental health outcomes presents three important gaps.
First, to date little research has examined how digital behavior throughout adolescence is associated with later mental health in young adulthood (McCrae et al., 2017). Current literature is largely focused on cross-sectional associations of digital use on youth mental health, lacking longitudinal perspectives (Course-Choi & Hammond, 2021). Particularly, current research has tended to miss a developmental perspective that considers how the effects of digital behaviors throughout the critical stages of adolescence might accumulate in ways that impact later mental health outcomes in adulthood (Hollenstein & Colasante, 2020). Understanding the cumulative effects of digital use over time, instead of examining just contemporaneous effects, is particularly relevant to design appropriate and efficacious interventions and policies to prevent mental ill health outcomes among young people (Kardefelt-Winther, 2017). This calls for new research addressing such effects of digital use throughout adolescence and youth.
Second, what potential pathways connect digital use and mental health during adolescence remains unclear (Ivie et al., 2020). The preponderance of current research largely utilizes regression modelling and testing direct associations of digital engagement on various mental health outcomes (Course-Choi & Hammond, 2021). While this approach captures the associations between digital use and youth mental health, it limits our understanding of potential paths between digital behaviors and mental health. As a result, it is difficult to design policies and interventions that effectively target potential risks of youth digital engagement. Therefore, conducting systematic research on (in)direct effects, as well as exact pathways, behind the association between young people’s digital use and their mental health is of particular importance.
Third, and finally, the role of gender in the associations between adolescent digital use and well-being outcomes across developmental stages is not clearly understood. Given observed gender differences in adolescent digital behaviors, as well as the well-known social, emotional, and psychological differences between boys and girls during adolescence, it is likely that young men and women’s mental health is differently affected by their digital use (Booker et al., 2018; Salmela-Aro et al., 2017). However, there is limited research on gender differences, particularly in mechanisms, between digital use and mental health, which may be particularly salient considering the variety of differences by gender observed across developmental outcomes (Yoon et al., 2023). Therefore, investigating and examining associations and mechanisms by gender is crucial to understand sociodemographic inequities in digital engagement, and to design policy that is targeted towards those who are most at risk.
The present study tackles these important scientific gaps mentioned above by achieving four key objectives:
i. To assess whether current digital screen-time is associated with depressive symptoms among young adults
ii. To examine if young people’s previous digital behaviors throughout adolescence is associated with depressive symptoms in young adulthood.
iii. To investigate potential explanatory pathways between digital use and depressive symptoms for observed associations—via sleep, physical activity, self-esteem and body image.
iv. To examine how the existing associations and pathways between digital use and depressive symptoms vary by gender.
Background
Digital Use and Youth Depressive Symptoms
Debates over the potential effects of adolescents’ digital use on mental health outcomes have been ongoing since the 1990s. Over the past 30 years, concerns have continued to raise over how adolescents and young adults both use and are affected by increasingly powerful and ubiquitous digital technologies (e.g. mobile phones, iPads, etc.). Associations between adolescent digital use and depressive symptoms have been the focus of multiple previous studies (Kelly et al., 2018; Layte et al., 2023), and the subject of systematic reviews and meta-analyses by McCrae et al. (2017) and Ivie et al. (2020), respectively. Both McCrae et al. (2017) and Ivie et al. (2020) found that, overall, current empirical research shows a significant correlation between digital and social media use and depressive symptoms in young people. However, both reviews found a high degree of heterogeneity in the literature due to “widely varying methods, sample sizes and results, making the clinical significance of these findings nuanced” (McCrae et al., 2017, p. 315). Most previous studies in this field use cross-sectional data, with most longitudinal studies covering only small segments of adolescence (McCrae et al., 2017). In this context, longitudinal data and approaches are essential to be able to empirically assess the “effects of spending time on digital technology from a young age” (Kardefelt-Winther, 2017, p. 253).
This temporal reality of contemporary adolescents’ digital use (i.e. that today’s young people have spent most of their adolescence engaged with digital technologies) is often overlooked by the literature. Particularly, there is an absence of research that examines how accumulated digital behaviors and chronic usage patterns might impact later developmental outcomes. Considering the large role that digital use now plays in adolescent’s lives, both socially and temporally, examining such potential accumulation effects becomes crucial (George et al., 2018). Overall, previous research presents a substantial gap in understanding the role of digital behaviors throughout adolescence, and their association with depressive symptoms in later young adulthood.
Additionally, Ivie et al. (2020, p. 165) note that “other factors are likely to act as significant mediators of the relationship” between digital use and depressive symptoms, indicating the need for further research that examines potential mediators and pathways. Our study addresses this gap in the literature by bringing a longitudinal approach that considers explanatory mechanisms and pathways between early adolescent digital use and later youth mental health.
Digital Use, Gender, and Mental Health
Previous studies seem to indicate that digital engagement could lead to gender differences in well-being. Given that gender difference in depression peaks at adolescence, with three times as many adolescent girls diagnosed with depression as boys (Salk et al., 2017), it seems especially important to consider whether there are gender differences in associations between digital use and adolescent well-being. A focus on gender differences is particularly important given the sharp rise in unhappiness, depression, and suicide risk factors among adolescents since 2012, especially as these associations are stronger among girls (Keyes et al., 2019; Spiller et al., 2019; Twenge et al., 2018). If these declines in psychological and socioemotional well-being among girls are related to patterns of digital use, it is imperative to examine potential differing associations and pathways between digital use and well-being across gender.
Social media and online communication with friends may have differential impacts by gender. Girls and women may be more likely to engage in social comparison and seek feedback on social media (Nesi & Prinstein, 2015). Girls also spend more time than boys in carefully crafting their online image and soliciting help from friends in doing so (Yau & Reich, 2018), possibly as a result of girls self-objectifying more (Fredrickson & Roberts, 1997). Social media use in particular is linked to worries about body weight among adolescent girls (Tiggemann & Slater, 2017). A recent study found that cyberbullying, lack of sleep, and lower physical activity mediated the link between social media use and mental health among girls but not among boys, suggesting that these mechanisms may explain the link for girls, but other mechanisms may be in place for boys (Viner et al., 2019). As very few studies have addressed such gender mechanisms, new research in this area is needed.
The way gender differences in time spent across different digital activities links to mental health has been debated, but research on this question is inconclusive. Boys have been found to spend more time than girls on digital activities, focusing especially on gaming, while girls engage relatively more on social digital activities (Gracia et al., 2020; Ortega et al., 2010; Wight et al., 2009; Mikuška & Vazsonyi, 2018). Boys, particularly at high levels of digital use, have also been found to show greater risks of depressive symptoms than girls (Ortega et al., 2010). However, little research has explored how these differences in quality and quantity of digital use between boys and girls may affect well-being outcomes.
To summarize, further research is essential to understand the moderating role of gender in how digital engagement throughout adolescence is associated with later mental health outcomes. This paper fills this important gap in the gender literature on adolescent digital use and well-being by (1) utilizing longitudinal data that spans from early adolescence (i.e., at age 9, 13 and 17) to young adulthood (i.e., age 20), (2) testing conceptual pathways, and (3) examining differing associations and pathways between men and women.
Conceptual Framework
The theoretical underpinning of our conceptual framework is derived from a time-displacement perspective, which posits that increased time spent on one activity must necessarily mean a directly inverse decrease in time spent on another activity. In the case of the present research, the time displacement hypothesis infers that time spent on digital technologies is “inversely related to mental well-being” due to time spent on digital technologies displacing “healthier activities” (Rosen, 2019, p. 5), such as sleep and physical activity. Further, time spent on digital technologies by adolescents is hypothesized to substitute face-to-face, socially stimulating activities and relationships, leading to weak social relationships and “increased feelings of social isolation and disconnectedness” (George et al., 2018: 81). This hypothesis also centers the idea of digital technologies as developmentally deleterious gateway to materials and situations that may be distressing for adolescents, such as cyberbullying, unrealistic body representations, and violent or explicit content (Fahy et al., 2016; Verduyn et al., 2017). Thus, engagement with digital technology is seen as a locus for the development of low self-esteem and body image issues (de Vries et al., 2016).
To further guide our conceptual model, we utilize the model put forth by Kelly et al. (2018) on explanatory pathways between social media use and adolescent depressive symptoms. The model by Kelly et al. (2018) was chosen as a basis for our conceptual model as 1) it focuses on the same outcome variable (depressive symptoms), 2) the model was conceptualized for a similar age group, and 3) the model incorporates many of the most widely researched and cited hypothesized pathways between digital use and mental health outcomes (i.e. poor sleep, poor self-esteem, and body image). Thus, we utilize this model by Kelly et al. (2018) to form the basis for our own conceptual model (Figure 1A).
The literature, as well as the model by Kelly et al. (2018), points to specific factors which have been consistently hypothesized and studied as potential mediators and pathways between digital use and youth mental health. Previous studies have hypothesized sleep as a potential pathway (Kelly et al., 2013; Lemola et al., 2015). Digital use can impact sleep in multiple ways, including time displacement leading to poor sleep duration (Woods & Scott, 2016), sleep disruption from incoming alerts and messages (Garmy et al., 2012), and sleep disruption from screen exposure (Cain & Gradisar, 2010). Digital use has also been found to be associated with decreased and/or displaced physical activity, which can lead to poorer physical and mental health (Viner et al., 2019). Further, young people and adolescents are particularly vulnerable to developing low self-concept and self-esteem, which could be worsened by negative social comparisons facilitated through digital engagement (Frison & Eggermont, 2016; Valkenburg et al., 2017). The abundance of manipulated images of idealized “beauty” online are linked to individual perceptions of body image and self-esteem which in turn are associated with poor mental health (de Vries et al., 2016; Fardouly & Vartanian, 2016). Cyberbullying and online harassment have also been found to be potential mechanisms between digital use and youth mental health (Fahy et al., 2016; Livingstone & Smith, 2014); however, the data in our study does not have a measure for cyberbullying victimization and thus it is unable to be incorporated into our conceptual model for use in this study. Therefore, from the literature as well as previous models (Kelly et al., 2018; Viner et al., 2019), four key explanatory pathways between digital use and youth mental health emerge: sleep, physical activity, self-esteem, and body image.
Thus, our study seeks to examine underlying pathways between young people’s digital use and depressive symptoms via the displacement of critical health activities (sleep and physical activity), and via digital technologies as a gateway to deleterious and harmful content (low self-esteem and body weight satisfaction). We additionally anticipate that given the gendered sociocultural and physiological nature of adolescence and young adulthood, that significant pathways (and their magnitude) between digital use and depressive symptoms will differ between men and women. Accordingly, we test three hypotheses, outlined in the path model of Figure 1.
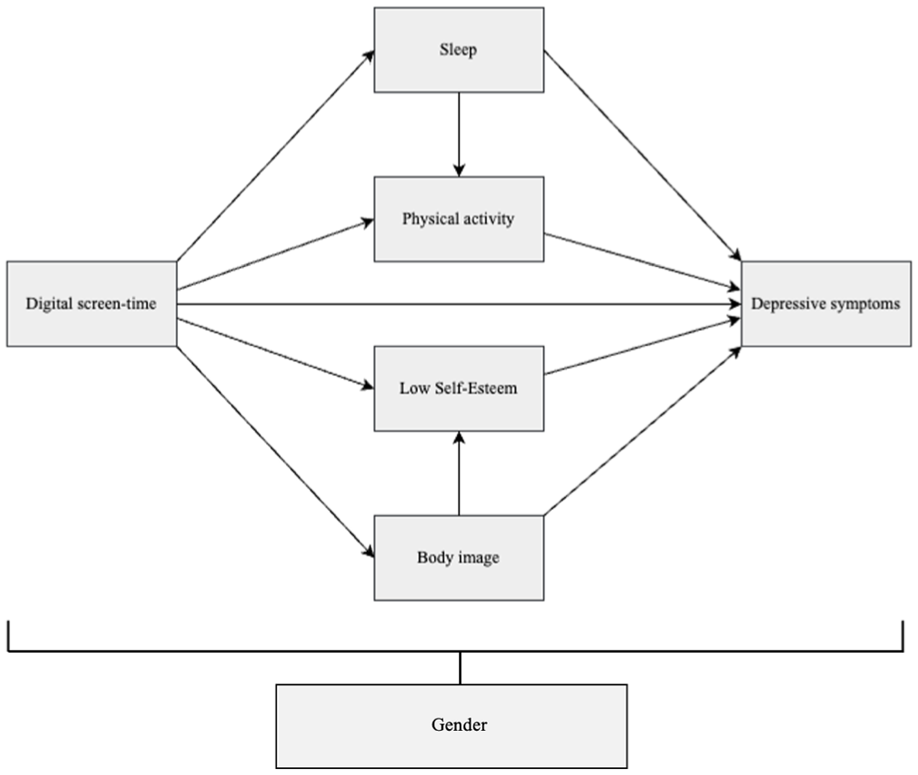
Hypothesized path model for digital screen-time on young adult depressive symptoms.
Methods
Data and Sampling
This study utilizes high-quality survey data from the “Child Cohort” of the Growing Up in Ireland (GUI) study. The GUI is a nationally representative longitudinal multi-cohort study of children living in Ireland which combines rich information on children, parents, and households, with repeated measures on digital engagement and well-being across four currently available waves. The Child Cohort consists of a nationally representative sample of Irish children aged 9 who were born between 1st November 1997 and 31st October 1998 (Williams et al., 2009). Participating families were sampled via a two-stage design in which a random sample of Irish nine-year-olds was selected out of a random sample of all Primary Schools in Ireland. The original sample at age 9 represented approximately 14 percent or about 1 in every 7 of nine-year-olds resident in the country. The GUI uses repeated measures collected across four waves of data collection, including at age 9, age 13, age 17/18, and age 20. At age 20, Young Adult participants and their parents were interviewed at their address(es) of residence via Computer Assisted Personal Interview (CAPI).
Our study sample includes all cohort members for whom data on depressive symptoms were available at age 20 (N = 5,077). Multiple imputation was implemented to maintain this sample by multiply imputing missing values on explanatory factors due to item non-response. Twenty datasets were imputed, and we report consolidated results from all imputations. The study sample is weighted with appropriate survey weights for the age 20 sample.
All measures used for analyses are presented in detail in Table 1A. These measures are further detailed in sections 2.2 through 2.4.
Depressive Symptoms
Participants completed The Centre for Epidemiological Studies Depression scale (CESD-8). The Centre for Epidemiological Studies Depression scale (CESD-8) is a widely used self-report measure that was developed specifically as a screening instrument for depression in the general population, as opposed to being a diagnostic tool that measures the presence of clinical depression.
Growing Up in Ireland used the 8-item short version of the CES-D (CESD-8) and provides a total score for the young adult participant, ranging from 0 –20.
“Current” Digital Use (At Age 20)
Across waves of the GUI survey, measurement of digital use varies. All waves include measurements of daily screen-time, as well as whether study participants take part in various digital activities. At age 20, the GUI asks how long participants spend online on an average weekday. The respondent is given five response options: 0 hours, less than one hour, 1–2 hours, 2–3 hours, and 3 hours or more. Similar to previous waves, participants are also asked what digital activities they engage with, and thus we include measures indicating participant’s engagement in the following digital activities: social media, socializing/communication, media consumption (watching TV, listening to music, watching YouTube videos, etc.), education, and gaming.
Previous Digital Use
In order to operationalize “previous digital use”, we utilize data from waves 1–3 (age 9–18) of the GUI Child Cohort. A classification system was constructed to differentiate study participants who were light, moderate, and heavy users on average throughout adolescence, as the number of response categories for screen-time varied by wave. To do so, we classify a respondent as belonging to a particular usage category if they were, for example, a “light user” in at least two of the three GUI waves. However, because screen-time averages vary considerably by age, what is considered “light” and “heavy” varies wave to wave. Thus, respondents were considered light users if they were non-users at age 9 and at age 13, and if they were a non-user or has “less than an hour” average weekday screen-time at age 17/18. Moderate users were those respondents with “less than an hour” of digital use at age 9, “less than an hour” and “1–3 hours” at age 13, and “1–3 hours” at age 17/18. Finally, respondents were considered heavy users with “1–3 hours” and “3+ hours” digital use at age 9, “3+ hours” at age 13, and “3+ hours” at age 17/18.
Mediator Variables
Our conceptual model highlights four other key variables: sleep, physical activity, self-esteem, and body image. In the GUI, sleep is measured by sleep duration i.e. how many hours respondents slept on an average night. To measure physical activity, respondents were asked how often in the last 14 days they had participated vigorous physical activity. Categories were recoded into 0 “None” 1 “Multiple days per week” and 2 “Most days.” At age 20, self-esteem was measured in the GUI using the Rosenberg Self-Esteem scale (Rosenberg, 1965). The Rosenberg Self-Esteem scale contains six items rated on a four-point scale, with higher scores indicative of higher global self-esteem. In our analyses we utilize a dichotomized variable (low vs normal/high) derived from the sum of the items, with scores ≤ 9 (i.e. the bottom 25% of the distribution) indicating low self-esteem. Finally, “body image” will be operationalized as “body weight satisfaction”. Respondents were asked how they felt about their bodyweight (e.g, severely underweight, moderately overweight, etc). These have been recoded into a binary variable to differentiate between those who were satisfied with their body weight (i.e. answered that they feel they are “just the right size”) and those who are not satisfied with their body weight.
Confounders
In line with prior research (Bohnert & Gracia, 2021; Kelly et al., 2018; Parkes et al., 2013), we controlled for the following confounders: socioeconomic status (parent occupational class), family income (equivalized fifths), family structure (one vs two parent),
Study Sample Proportions, Means, and Standard Deviations (Age 20).
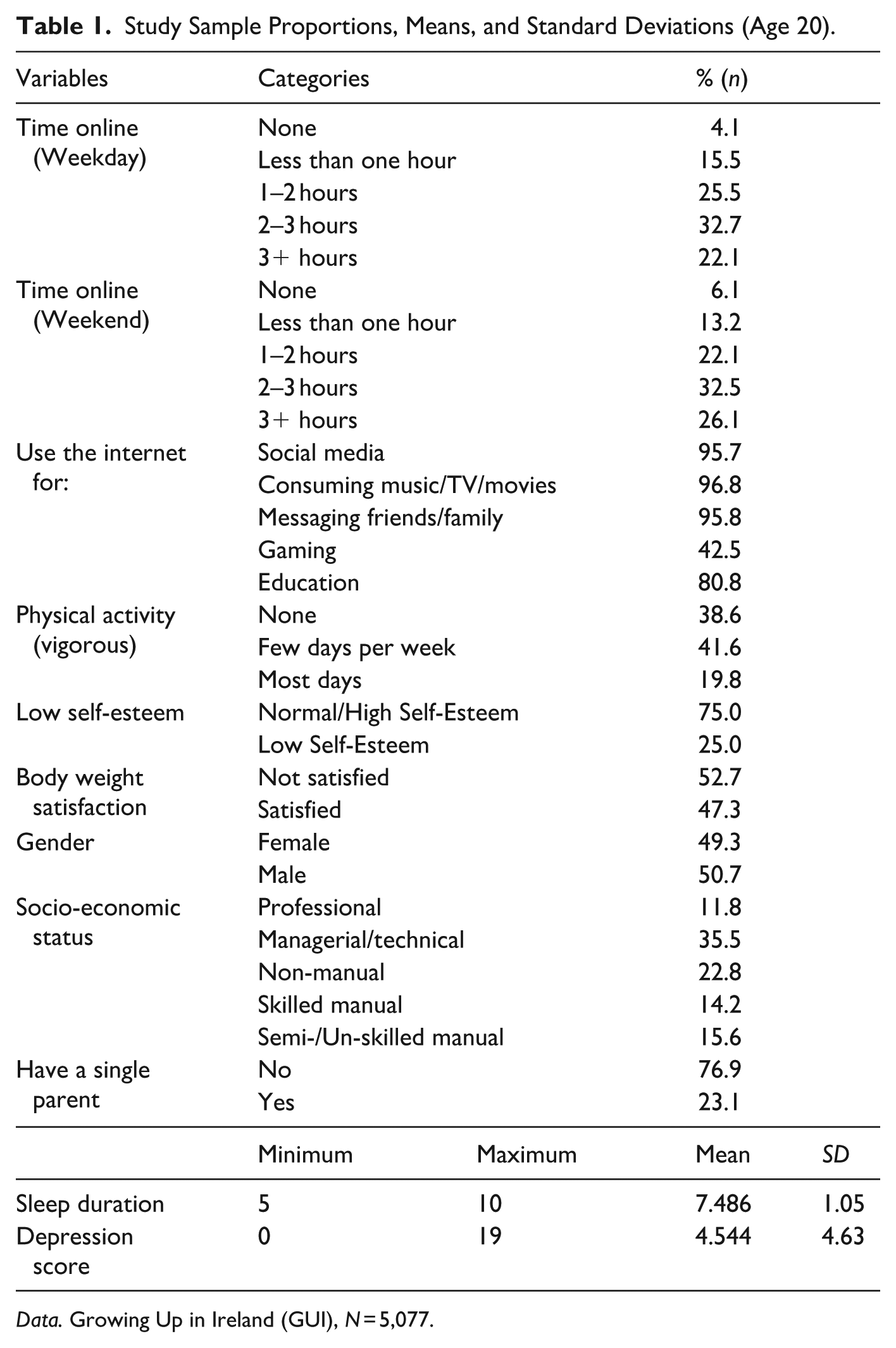
Data. Growing Up in Ireland (GUI), N = 5,077.
To account for the potentially cyclical association between digital use and depressive symptoms we controlled for previous emotional difficulties, derived from the “Emotional Difficulties” subscale of the Strengths and Difficulties Questionnaire completed at all previous waves. Previous depressive symptoms was unable to be used to account for this bidirectionality, as it is only measured at age 20, and the SDQ is unavailable in our age 20 sample.
Empirical Strategy
The study sample was first explored descriptively. First, we examine descriptive statistics of all variables included in analyses at age 20, and additionally descriptive gender differences in digital engagement. Second, to examine associations of previous and current digital use with depressive symptoms at age 20, we conduct multivariate linear regressions. We examine whether and by how much associations of digital use and depressive symptoms are explained by markers of sleep, physical activity, self-esteem, and body image. Analyses are also run separately for men and women at age 20, to examine differences in associations by gender. Finally, we conduct path analyses to quantify the hypothesized explanatory pathways between digital use and depressive symptoms. Multiple path models are estimated such that each model will be estimated for the entire sample and then separately to be constrained by gender. The path models are estimated using the generalized structural equation model, GSEM command in Stata. This command allows for the continuous, binary, categorical and ordered measures to be modelled. All analyses are carried out using Stata version 16.1.
Results
Descriptive Statistics
Table 1 presents descriptive statistics with proportions, means and standard deviations for our variables of study in our age 20 sample. First, we observe that most respondents are active daily digital users, with only 4.1% of our sample reporting no time online per average weekday. Around 15% of our sample reports minimal daily usage of less than one hour, and over half of the sample (58.2%) falls somewhere between 1–3 hours daily digital use.
Approximately a fifth of our sample (22.1%) reports spending over 3 hours on digital devices per average weekday. Weekend estimates are largely similar, with a 4% increase in respondents reporting over 3 hours digital use per average weekend day. We observe nearly full engagement in social media (95.7%), media consumption (96.8%) and socializing/communication (95.8%) digital activities. Further, approximately 80% of the young adult respondents engage in educational/learning oriented activities, and 42.5% engage in online gaming.
We further examined gender differences in digital use across the four currently available waves of the 1998 “Child Cohort” of the GUI study (Table 2A). We observe that the proportion of digital non-users is consistently higher among male respondents, and that the proportion of heavy digital users (3+ hours per day) is consistently higher among females throughout adolescence and young adulthood. Girls additionally appear to have engaged more extensively than boys in socializing and educational digital activities in earlier stages of adolescence (age 9 and age 13), though these gaps appear to shrink in young adulthood. Finally, we observe a substantial gender gap in engagement with online gaming that emerges at age 13 between boys and girls. At age 13, 21% more boys report engaging in gaming than girls, which rises to 42% at age 17/18, and 52% at age 20.
Further, we observe that 68.2% of our sample were classified as “moderate” digital users throughout their adolescence, 23.2% were classified as “light” users, and 8.6% fitted in the category of “heavy” users. We find that more boys (25.2% vs 21.1%) are classified as “light” users and more girls (11.4% vs. 6.0%) are classified as “heavy” users (see: Table 2A).
Associations of Digital Use on Depressive Symptoms: Screen Time at Age 20
OLS linear regression models were run for the total sample, and separately for men and women. Model 1 presents regression results with only digital use variables and confounders, and Model 2 presents regression results of Model 1 with the mediator variables (i.e. sleep, physical activity, low self-esteem, and body image). The analyses of Model 1 are graphically supported by Figure 2, and detailed regression outputs are available in Table 3A.
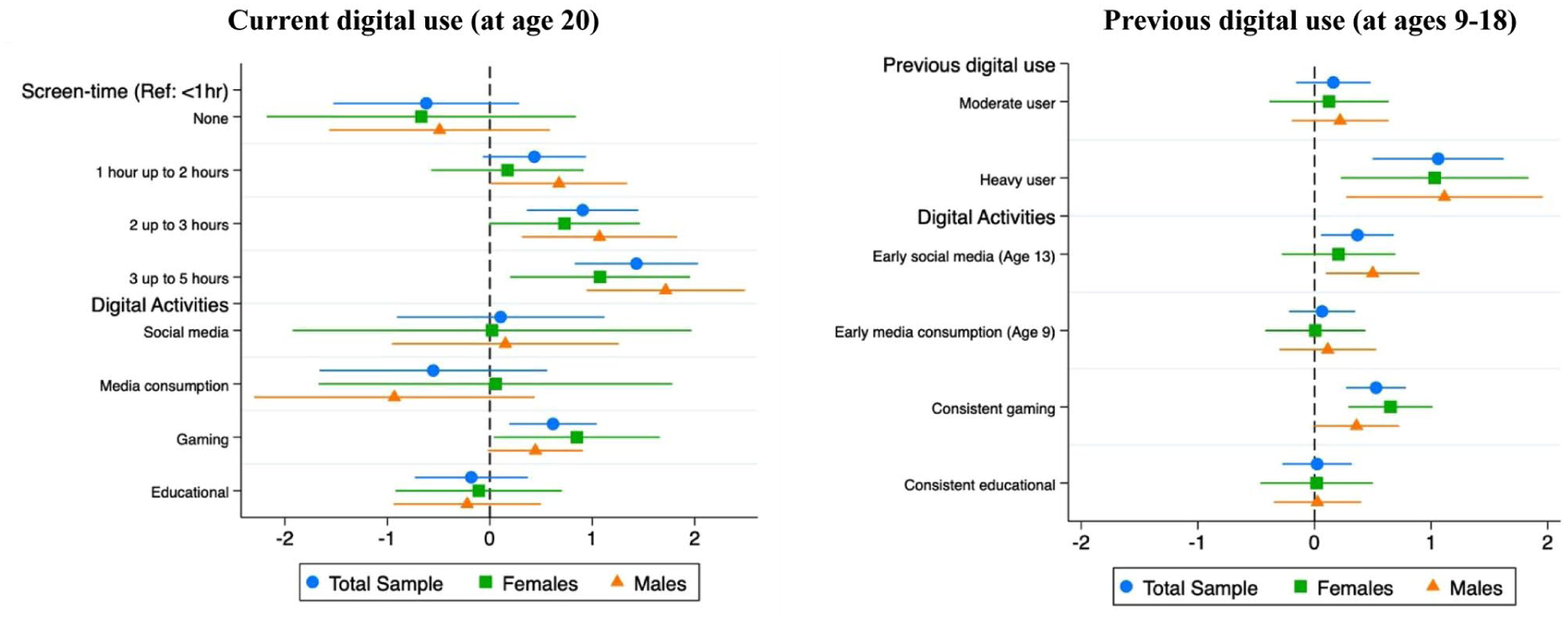
Coefficient plot of digital screen-time on depressive symptoms.
In model 1, we find that 2–3 hours (B = .938; p < .01) and 3+ hours (B = 1.426; p < .001) of daily screen-time at age 20, compared to those who engage in less than an hour of daily screen-time, is associated with significantly higher depressive symptom scores. Gaming is the only specific digital activity we find to be significantly associated with depressive symptoms. We find that those young adults who engage with online gaming to have higher depressive symptoms at age 20 (B = .602; p < .01).
When the models are observed separately for men and women, we find more significant associations between time spent online and depressive symptoms in young adult men than in young adult women: 2–3 hours (B = 1.099; p < .01) and 3+ hours daily screen-time (B = 1.694; p < .001) are significantly associated with higher depressive symptoms for men, while only 3+ hours daily screen-time is significant for women (B = 1.087; p < .01). However, we find the magnitude of the association between online gaming and higher depressive symptoms is only significant for men (B = .478; p < .05) at age 20.
We then observe our results when the variables from our conceptual model (i.e. sleep, physical activity, self-esteem and body image) are added to the analyses, captured in Model 2 (Table 3A). When these variables are added, we find a reduction in the magnitude and significance of coefficients between online screen-time and depressive symptoms, suggesting these factors at least partially explain the observed associations. Despite this reduction in the size of the coefficients, we observe that 2–3 hours and 3+ hours of daily screen-time remains statistically significant in the association with higher depressive symptoms within our full sample analyses (B = .458, p < .05; B = .923, p < .001). Further, if we observe Model 2 separately for men and women, we find that the addition of these further variables completely erases any significant association of online screen-time and depressive symptoms for women, while 2–3 hours and 3+ hours daily screen-time remains significant for men (B = .564, p < .05; B = 1.105, p < .001).
Associations of Digital Use and Depressive Symptoms: Previous Adolescent Digital Engagement
OLS linear regression models examined associations between previous adolescent digital use and depressive symptoms for the total sample, as well as separately for men and women (see: Table 4A). Model 1 presents regression results with only previous digital use variables and confounders, and Model 2 presents regression results of Model 1 + mediator variables from our conceptual model (i.e. sleep, physical activity, low self-esteem, and body image). The analyses of Model 1 are graphically supported by the second panel of Figure 2.
When mediator variables are added in Model 2 (see: Table 4A), we find that the associations between previous adolescent digital use and depressive symptoms at age 20 are no longer statistically significant for men, but remain significant in the overall sample (B = .600; p < .05) and for women (B = .753; p < .05), though with decreased magnitude compared to Model 1. This finding may indicate that the association between digital use throughout adolescence and depressive symptoms are almost largely explained by associations of depressive symptoms with sleep, physical activity, self-esteem, and body image. However, mediation analysis in future research would be necessary to explore more exact mediation patterns.
Path Analysis
The first path model, captured in visually in the leftmost model in Figure 3, presents path modelling results between digital screen-time and depressive symptoms at age 20 (see: Table 5A). We first observe that there is a statistically significant direct path between contemporaneous digital screen-time and depressive symptoms at age 20 (B = .339; p < .001). We also observe significant pathways via poor sleep (B = -.045; p < .05), decreased physical activity (B = −.063; p < .01), low self-esteem (B = .034; p < .001), and decreased body weight satisfaction (B = -.035; p < .001), confirming our hypothesis H-1. Additionally, we find that the relationship between body weight satisfaction and depressive symptoms to be significantly mediated by low self-esteem (B = -.155; p < .001).
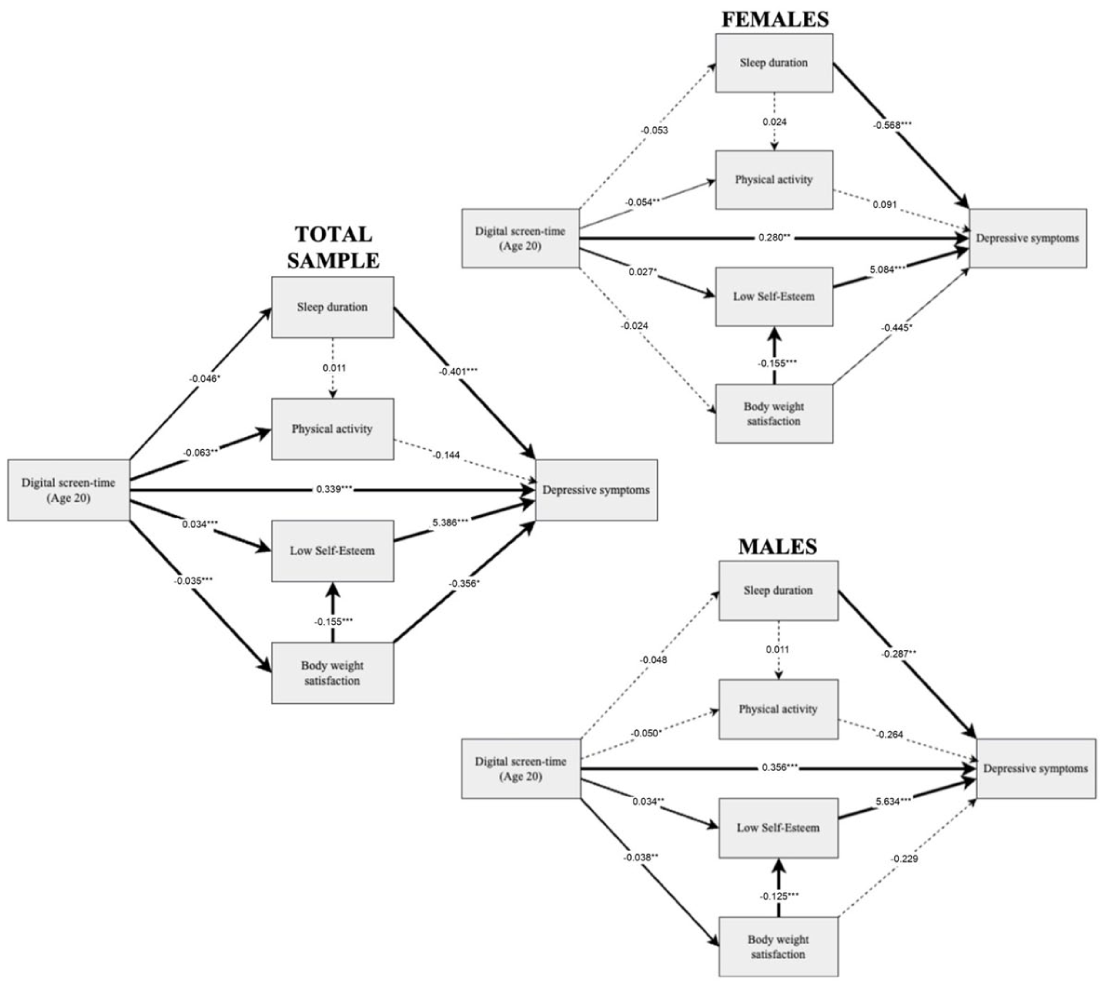
Path analysis for current digital screen-time on depressive symptoms at age 20: Total sample and by gender.
The right panels of Figure 3 then capture the results of our path model between current digital screen-time and depressive symptoms at age 20 separately for men and women. For both women and men we find significant direct paths between digital screen-time and higher depressive symptoms (B = .280, p < .001; B = .356, p < .001, respectively). We also observe a statistically significant pathway between current digital use and young adult depressive symptoms via low self-esteem for both men (B = .034; p < .01) and women (B = .027; p < .05).
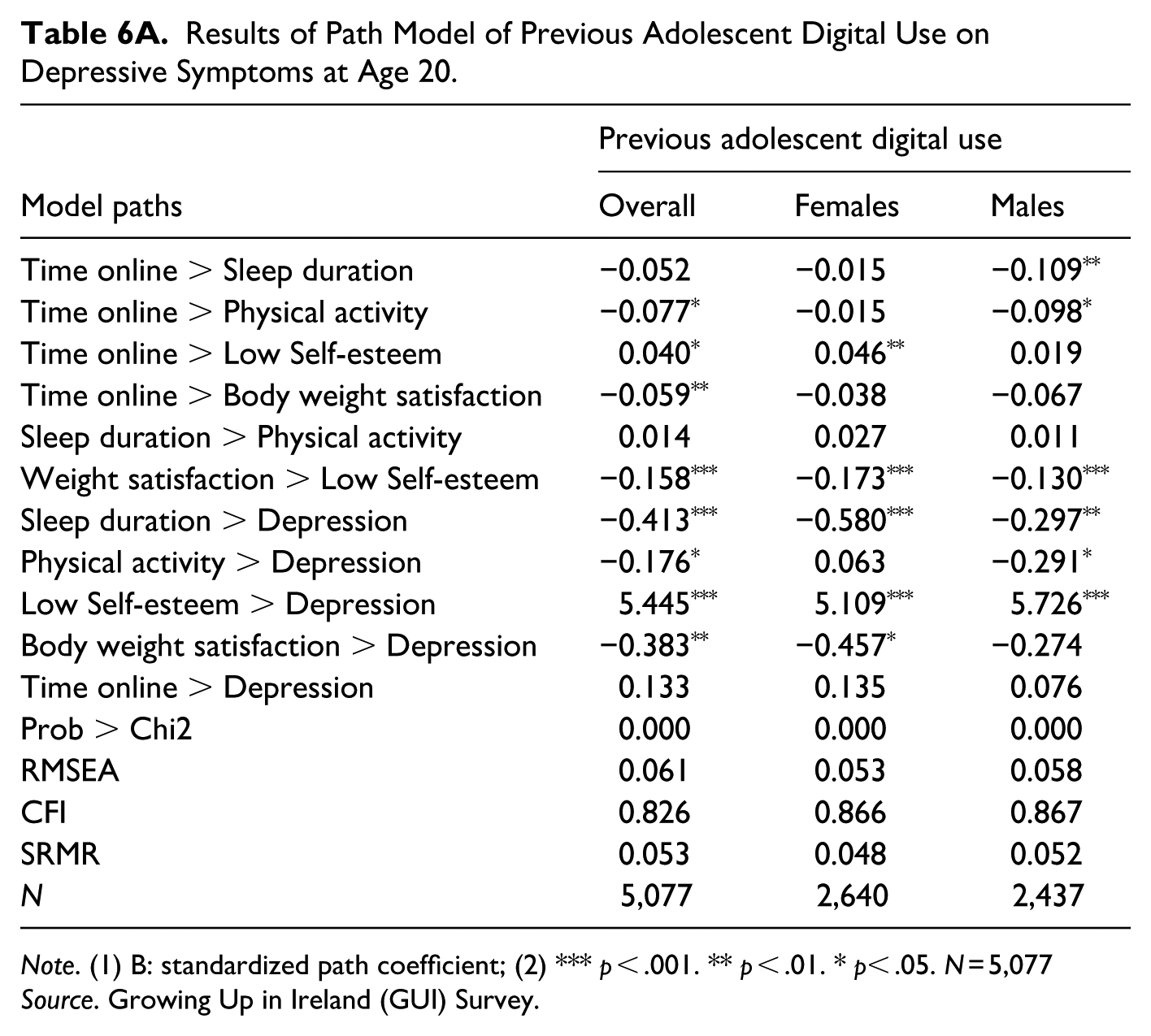
Figure 4 presents the results of our second path model (see: Table 6A) between previous adolescent digital use (i.e. light, moderate, heavy usage) and depressive symptoms at age 20. Our results show that there is no significant direct path between previous adolescent digital use and depressive symptoms at age 20. However, we observe statistically significant pathways via decreased physical activity (B = −.077; p < .05), low self-esteem (B = .040; p < .05), and decreased body weight satisfaction (B = -.059; p < .01).
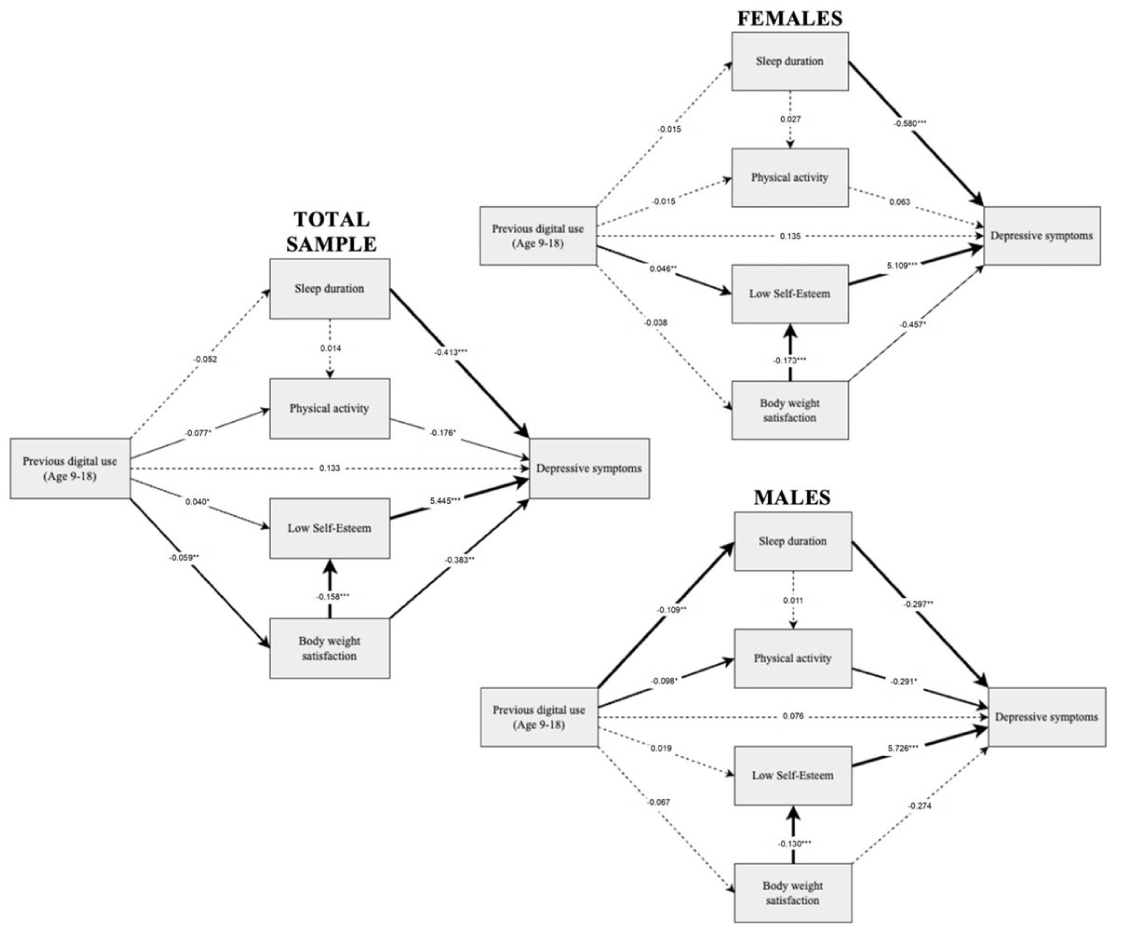
Path analysis for previous digital screen-time (Ages 9–18) on depressive symptoms at age 20.
Finally, the rightmost panels of Figure 4 graphically present the results of our path model between previous adolescent digital use and depressive symptoms at age 20 separately for men and women. Similar to digital use at age 20, we observe that the only pathway between previous adolescent digital use and young adult depressive symptoms that is statistically significant for women is via low self-esteem (B = .046; p < .01). For men, however, we observe significant pathways via decreased sleep duration (B = −.109; p < .01) and decreased physical activity (B = −.098; p < .05).
Overall, we find the relationship between both current and previous digital use and depressive symptoms in young adulthood to be partially mediated via poor sleep, reduced physical activity, low self-esteem, and decreased body weight satisfaction. Thus, we validate our hypotheses H-1 and H-2. Further, while we did find significantly different pathways between men and women in our models, we did not find any evidence that paths are stronger for women than for men. Therefore, we partially validate H-3.
Discussion
This study has contributed to the literature with a new analysis of how current and previous adolescent digital use is associated with depressive symptoms in young adulthood. Using robust, longitudinal data from the Growing Up in Ireland (GUI) survey, this study goes beyond associations to assess key explanatory mechanisms, as well as examine differences in associations and pathways by gender.
We can highlight three main findings from our study. First, we found that heavy amounts of daily screen-time in young adulthood is associated with higher depressive symptoms. Daily screen-time above 2 hours is associated with significantly higher depressive symptoms compared to those who spend less than one hour per day online, and associations are particularly strong for those who spend over 3 hours daily on digital devices. Similarly, we also find that consistently “heavy” digital usage throughout adolescence is associated with higher depressive symptoms, compared to “light” adolescent usage. These results complement research showing that negative effects of digital screen-time on well-being are particularly salient at high levels of daily usage during childhood (Bohnert & Gracia, 2021). Such heavy digital use is theorized to be deleterious to mental health and depressive symptoms because of the substantial time displacement it necessitates. For example, time online displaces healthier and/or more enriching face-to-face activities (e.g. sleep, exercise, in-person socializing) (George et al., 2018). Additionally, lengthy time spent online also increases both the likelihood and the length of exposure to potential harmful online content, such as unrealistic body standards, cyberbullying, and pornography, leading to poorer mental health.
Second, our results reveal key explanatory pathways in the association of digital use and depressive symptoms. We found a direct path between contemporaneous digital use and higher depressive symptoms at age 20 through multiple mediating pathways, specifically via poor sleep, low self-esteem, and decreased body weight satisfaction. This finding supports the study by Kelly et al. (2018) which found robust mediating paths between social media use and depressive symptoms via sleep, self-esteem, and body image. Thus, our study lends further evidence that sleep, self-esteem, and body image are key mediators and potential mechanisms in the relationship between young adult digital use and mental health. Additionally, our path model between previous adolescent digital use and depressive symptoms at age 20 revealed significant mediating paths via decreased physical activity, low self-esteem, and poor body weight satisfaction. While accumulated digital behaviors throughout adolescence do affect mental health in young adulthood through multiple paths, the strength of associations and paths are much stronger for current/contemporaneous digital use than for previous digital use, and we do not observe a direct path between previous digital screen-time and depressive symptoms. This suggests that the association operates indirectly through mediating mechanisms rather than as a direct effect. Thus, contemporaneous digital behavior is substantially more salient for depressive symptoms in young adulthood than previous digital behaviors.
Third, our study finds differences and similarities and associations and pathways by gender. We find that associations between both current and previous digital screen-time and depressive symptoms during young adulthood are largely similar across gender, though we find associations to be slightly stronger for men versus women. Further, our results show that the association between contemporaneous digital use and depressive symptoms at age 20 is primarily explained by low self-esteem for both men and women. These findings differ from recent cross-sectional studies that found significant differences in pathways of digital use and depressive symptoms by gender (e.g., Kong et al., 2022; Svennson et al., 2022). Yet, when we examine pathways between previous adolescent digital use to current depressive symptoms in young adulthood, we seem to find gendered processes. While the relationship between previous digital use and depressive symptoms for women is still mediated through lowered self-esteem, the relationship with previous adolescent digital use and later depressive symptoms among men is significantly mediated via poor sleep and decreased physical activity. Thus, we observe that the mechanisms by which adolescent digital use affects later mental health differs substantially between girls and boys across developmental stages. Particularly, we observe that the significant pathways for men come from accumulated effects of past digital use on physical behaviors (e.g. sleep, physical activity) and for women from accumulated effects of past digital use on emotional/mental behaviors (low self-esteem), which may imply that patterns consistent with digital exposure throughout adolescence function through significantly gendered mechanisms. These findings refine prior expectations, suggesting that gender differences may lie more in pathway structure than in overall effect magnitude.
Our study has some shortcomings and limitations that need to be mentioned. First, our analyses are limited by the digital use variables at our disposal through the GUI study. Particularly, our analyses rely on self-report data of respondent’s digital behaviors, which can introduce some biases (Araujo et al., 2017).
Despite these limitations, this study and its findings are highly relevant to ongoing policy development. Our findings on the detrimental associations of heavy digital screen-time on young adult depressive symptoms have clear implications on current and future guidelines for the safe and responsible use of digital technologies by adolescents and young people. These findings are particularly relevant considering the increased calls on industry to more tightly regulate both adolescent digital screen-time and content. Our study provides additional policy-relevant context by investigating key pathways and mechanisms, as well as gender differences in the potential pathways linking digital use and adolescent mental health. These findings are particularly helpful in designing effective public policy interventions, educational programs, and wider screen-time guidelines, as they help to tackle specific underlying mechanisms that work differently between young males and females.
To conclude, our study adds to current literature on digital use, gender, and mental health, using rich and robust longitudinal data from the 1998 “Child Cohort” of the Growing Up in Ireland (GUI) study to examine not only associations between digital use and mental health, but also key explanatory pathways. We find that heavy digital screen-time, both at the age of measured symptoms and throughout adolescence, is significantly associated with higher depressive symptoms. Further, we contribute to the international literature by examining multiple potential explanatory pathways between digital use and depressive symptoms (i.e. via sleep, physical activity, self-esteem, and body image) and demonstrating that, despite important gender similarities in associations, the explanatory pathways between digital use throughout adolescence and depressive symptoms in young adulthood differ between men and women. We hope our study will guide further literature on digital use and young people’s mental health, as well as encourage future research that explores and disentangles the complex interplay between digital processes and young people’s well-being in contemporary societies.
Footnotes
Appendices
Results of Path Model of Previous Adolescent Digital Use on Depressive Symptoms at Age 20.
| Model paths | Previous adolescent digital use | ||
|---|---|---|---|
| Overall | Females | Males | |
| Time online > Sleep duration | −0.052 | −0.015 | −0.109 ** |
| Time online > Physical activity | −0.077 * | −0.015 | −0.098 * |
| Time online > Low Self-esteem | 0.040 * | 0.046 ** | 0.019 |
| Time online > Body weight satisfaction | −0.059 ** | −0.038 | −0.067 |
| Sleep duration > Physical activity | 0.014 | 0.027 | 0.011 |
| Weight satisfaction > Low Self-esteem | −0.158 *** | −0.173 *** | −0.130 *** |
| Sleep duration > Depression | −0.413 *** | −0.580 *** | −0.297 ** |
| Physical activity > Depression | −0.176 * | 0.063 | −0.291 * |
| Low Self-esteem > Depression | 5.445 *** | 5.109 *** | 5.726 *** |
| Body weight satisfaction > Depression | −0.383 ** | −0.457 * | −0.274 |
| Time online > Depression | 0.133 | 0.135 | 0.076 |
| Prob > Chi2 | 0.000 | 0.000 | 0.000 |
| RMSEA | 0.061 | 0.053 | 0.058 |
| CFI | 0.826 | 0.866 | 0.867 |
| SRMR | 0.053 | 0.048 | 0.052 |
| N | 5,077 | 2,640 | 2,437 |
Note. (1) B: standardized path coefficient; (2) *** p < .001. ** p < .01. * p< .05. N = 5,077
Source. Growing Up in Ireland (GUI) Survey.
Ethical Considerations
This research received ethical approval in line with all relevant Irish legislation on child protection, research ethics and data protection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the DIGYMATEX project (870578) from the European Commission H2020 (call “DT-TRANSFORMATIONS-07-2019—The impact of technological transformations on children and youth”), the Government of Ireland Postgraduate Award from the Irish Research Council (project: Social Inequalities in Child Time Use and Development in Ireland: A Mixed-Methods Longitudinal Approach), the DIGINEQ project (Grant agreement ID: 101089233) funded by the European Research Council Consolidator Grant, and Equalise: the ESRC Centre for Lifecourse Health Equity (ES/Z504270/1).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Copyright Statement
There are no copyrighted materials utilized in this manuscript.
Data Availability Statement
Growing Up in Ireland (GUI) data is available to researchers upon request on a confidential and anonymized basis through the Irish Social Sciences Data Archive.