
Abstract
This article investigates the role of family socio-economic status (SES) as a buffer for adolescents with mental health disorders (MHDs) against entering precarious school-to-work trajectories. We follow a cohort born in Norway in 1992 from the age of 16–25 using data from administrative registers. We find that externalizing disorders, to a higher degree than internalizing disorders (registered in the 16–18 age range), are associated with subsequent precarious school-to-work trajectories (measured from January 2011 to December 2017) for both genders. In boys, high family SES seems to buffer the negative impact of externalizing disorders on entering precarious school-to-work trajectories, but not for internalizing disorders. In contrast, in girls, high-SES families partly buffer the negative impact of internalizing disorders, but not for externalizing disorders. Thus, this paper broadens the current perspective on how the impact of MHDs on entering school-to-work trajectories is interrelated with social class and gender.
Introduction
Youth joblessness and inactivity are major concerns in many European countries (Frøyland et al., 2022). Increasing demands for higher and more formal education in combination with high youth unemployment rates have made school-to-work trajectories more difficult and complex for young people in recent decades (Halvorsen & Hvinden, 2018). The ease or difficulty young people experience in these trajectories has a lasting impact on future life chances (e.g., on their labour market attachment; see Hammer & Hyggen, 2013), making this phase of life a highly critical one but also a window of opportunity for policy interventions aimed at preventing young people from ending up in marginalized positions.
Mental health disorders (MHDs) often have their onset in adolescence (Kessler et al., 2007), and a large and growing body of literature shows that poor mental health in adolescence is negatively associated with subsequent educational attainment and labour market attachment (Esch et al., 2014; Hale et al., 2015). Moreover, the evidence indicates strong associations between adolescent mental health problems and NEET (not in education, employment, or training) status (Gariépy et al., 2021). Meanwhile, in Norway, adolescents’ self-reported symptoms of mental health problems, as well as the clinical diagnosis and treatment of adolescent psychiatric disorders, have increased in recent decades (Simson et al., 2021).
The categorization of MHDs is often divided into internalizing and externalizing disorders: the former refers to symptoms directed inwards, such as mood and anxiety disorders, whereas the latter is recognized by symptoms directed outwards, such as behavioural and conduct disorders (Liu et al., 2011). In general, girls experience internalizing disorders more than boys, while externalizing problems are more common among boys than girls (Reneflot et al., 2018). Overall, externalizing disorders are found to have a consistent and strongly negative association with subsequent educational attainment and employment (Evensen et al., 2016; Melkevik et al., 2016; Veldman et al., 2015), whereas for internalizing disorders, the results are less consistent: some studies find educational and work outcomes to be compromised by internalizing disorders (Jensen et al., 2021; Simson et al., 2021; Veldman et al., 2017) while others do not (Evensen et al., 2016; Hetlevik et al., 2018; Landstedt et al., 2016).
Much political and scientific attention has been devoted to the intergenerational reproduction of socio-economic status (SES) (i.e., how the educational success and labour-market outcomes of children are closely related to parental SES; see Erola & Kilpi-Jakonen, 2017). However, research investigating how unequal access to family resources might create disparities in how MHDs impact school-to-work trajectories remains scant.
Thus, this study aims to investigate the interaction between adolescent MHDs, family background and school-to-work trajectories by posing the following research questions: (a) To what extent are externalizing and internalizing disorders in adolescent boys and girls associated with subsequent precarious school-to-work trajectories? (b) To what extent does the impact of externalizing and internalizing disorders on school-to-work trajectories in adolescent boys and girls vary by family background?
Unlike previous studies, which have mostly investigated the role of mental health in school-to-work trajectories by focusing on simple one-time transitions (e.g., educational or employment status at a given point), we use individual trajectories to construct an index of precarity based on individuals’ frequent status transitions and the undesirableness of the statuses (e.g., transitions between education, work or benefits over a period of 84 months or 7 years). Thus, the current study expands current knowledge of how MHDs affect the evolution of social position during youth, focussing on the complexity of the individual’s multiple status changes over a longer period rather than providing an instantaneous snapshot of the outcome (Albaek et al., 2015; Gauthier et al., 2014).
Background
Adolescent Mental Health Disorders and School-to-Work Trajectories
To the best of our knowledge, few studies have explored the impact of adolescent mental health issues on school-to-work trajectories when measured as more complex life-course trajectories. Huegaerts et al. (2019) followed 540 school-leavers in Brussels aged 18–29 years to investigate the impact of self-reported mental health status (collected in 2015) on school-to-work trajectories in the subsequent 20 months (2015–2017). Using administrative data on employment status (i.e., ‘employed’, ‘participating in active labour market policies’ and ‘unemployed’), six different clusters of school-to-work trajectories were constructed: ‘unemployed’; ‘stable employment’; ‘delayed employment’; ‘unemployed with guidance’; ‘set back to unemployment’ and ‘dropout’. The results of multivariable multinomial logistic regression show that men in ‘delayed employment’ had, on average, significantly poorer mental health than those in ‘stable employment’, after controlling for self-esteem and educational level. No differences were found between women. Thus, the study provides support for a more difficult transition into employment for men with adverse mental health issues. A Swedish study (Landstedt et al., 2016) investigated the importance of (self-reported) depressive symptoms at age 16 for school-to-work trajectories based on four questionnaire waves administered to a cohort of 1,001 individuals. Gender-separated trajectories were mapped between the ages of 18 and 42 using sequence analysis and including seven statuses of labour market attachment: ‘education’; ‘labour market measures’; ‘full-time employment’; ‘part-time/precarious employment’; ‘unemployment’; ‘outside labour market’ and ‘other’. The study revealed no differences in depressive symptoms across trajectory types for either men or women. Thus, the paper concludes that depressive symptoms do not seem to be associated with any selection processes.
Previous studies investigating the association between adolescent MHDs and educational and work outcomes from a gender perspective have yielded ambiguous results. The above-mentioned study by Landstedt et al. (2016) found depression symptoms in adolescence to be unrelated to unstable labour market trajectories in later adulthood for both men and women. In contrast, Simson et al. (2021), using Norwegian registry data, found that adolescents with internalizing and externalizing disorders completed upper secondary school less often than their healthy peers and, furthermore, attended tertiary education less frequently. These results applied to boys and girls alike after adjustments to family background and school characteristics. Fletcher (2008), using the National Longitudinal Study of Adolescent Health (Add Health), found females with depression in adolescence were less likely to graduate from high school, but not boys with depression. Also, girls with depression were less likely to enter college compared to females without depression, whereas no statistically significant relationship was found in boys. In later work, Fletcher (2013) found that females who experienced depression as adolescents were less likely than males with depression to be employed at age 30.
The Moderating Role of Family Background on School-to-Work Trajectories
There is an unambiguous relationship between young people’s school-to-work trajectories and family background (Albaek et al., 2015). Taken together, previous research supports the notion that parents with more resources available are in a situation to secure their offspring a better situation in every respect (Erola & Kilpi-Jakonen, 2017). But how do mental disorders in adolescence complicate this relationship? The compensatory advantage model (CAM) argues that high-SES families mobilize economic, social and cultural resources to counteract the negative effect of their children’s disadvantages, thereby avoiding adverse socio-economic outcomes (Gratz & Bernardi, 2017). For instance, advantaged families can pay for tutoring (Bernardi, 2014) or use social networks to open doors to the labour market for their vulnerable children.
In contrast, the ‘Blaxter hypothesis’ states that privileged adolescents facing an MHD might be unable to utilize the advantages that they hold over their peers, thus experiencing an equal or even greater risk of entering precarious school-to-work trajectories relative to less-privileged adolescents with mental disorders (Jackson, 2009). It is well documented that an offspring’s educational and occupational expectations are shaped by family SES (Andres et al., 2007). Privileged adolescents with MHDs who have trouble fulfilling their own and their family’s educational and occupational expectations have more to lose than adolescents from low-SES families with lower expectations, which explains the rationale behind the ‘Blaxter hypothesis’.
Few studies have investigated the moderating effect of family SES on the relationship between adolescent MHDs and later socioeconomic position, and they have yielded mixed results. Jensen et al. (2021), using mental health diagnoses extracted from the specialist health service, found that high parental educational level and high family income buffered the negative impact of externalizing and internalizing disorders on upper secondary school completion for girls, but less so for boys. A Finnish register-based study (Mikkonen et al., 2020) using six birth cohorts to investigate educational attainment by age 27 found that high parental education buffered the negative impact of MHDs on secondary education completion. However, high parental education exacerbated the association between MHDs and tertiary education completion. Evensen et al. (2016) found no moderating effect of high parental education on the association between self-reported externalizing and internalizing problems and educational attainment after controlling for all stable observable and unobservable characteristics shared between siblings. Another Norwegian study (Brekke & Reisel, 2017), this one using a health survey linked to longitudinal registry data, was unable to find a significant association between psychological distress and upper secondary school completion in either low- or high-income families when controlling for the other, included independent variables (e.g., parental education and health-related behaviour). A U.S. study (Jackson, 2009) using National Longitudinal Survey of Youth 1997 data found that the negative association between self-reported general health and timely high school graduation plus college attendance was greatest for non-Hispanic white adolescents compared to their black peers, controlling for household-fixed effects. These results indicate that a favourable family background defined by race/ethnicity does not buffer against the negative consequences of poor health on educational attainment.
Overall, the few studies exploring the moderating role of family background in the association between mental health problems and school-to-work trajectories have used single-state outcomes. To the best of our knowledge, the current study is the first to investigate how the interaction between MHDs and family background produces social inequalities in school-to-work trajectories when measured as processes.
The Norwegian Context
All public education in Norway is free of charge, and anyone who has completed compulsory education is entitled to an upper secondary school education, which offers a choice between an academic (normally 3 years in duration) and a vocational track (normally 4 years). Of all 16-year-olds, 98% enrol in upper secondary education the year they finish compulsory education (Utdanningsdirektoratet, 2020); however, one in five does not complete it within 6 years. The dropout rate is highest among boys following the vocational track (Statistics Norway, 2022). In higher education, there seems to be a widening gender gap as the proportion of higher-educated women increases relative to men (Statistics Norway, 2019). Moreover, the Norwegian labour market is characterized by gender equality; however, men and women work in different occupations and positions (Statistics Norway, 2015).
Norway has a publicly funded welfare system based on compulsory membership in the National Insurance Scheme, giving all Norwegian residents the right to social security and universal healthcare services (Oslo kommune, 2022). The primary health service, which covers general practitioner (GP) service and the school health service, among other benefits, has a legal responsibility to follow up and treat young people with mental health problems, but for more specialized investigation and treatment, GPs can refer children and young people to the specialist health service, where children and adolescents under 18 years can receive an examination, diagnosis and treatment from a Child and Adolescent Psychiatric Out-patient Clinic (BUP) (Helsenorge, 2020), where all contacts and treatments are registered in the Norwegian Patient Registry (NPR).
Methods
Data Sources and Population
This study uses register data provided by the NPR and Statistics Norway (SSB). The Directorate of Health manages the NPR, which includes, among other data, information on MHDs at the individual level from 2008 onward (Bakken et al., 2020). The SSB data includes information on income, demography, education, employment and all types of welfare benefits. Data access for the present study has been approved via a Data Protection Impact Assessment performed by Oslo Metropolitan University and through ethical vetting by the Regional Committees for Medical and Health Research Ethics and the various register owners. The study population includes all those born in 1992, residing in Norway, and alive from ages 16 through 25 (from 2008 to 2017). Given these restrictions, a total of 56,967 individuals are included in the analysis.
Constructing the Dependent Variable––Degree of Precarity of School-to-Work Trajectories
The construction of the dependent variable, Degree of precarity of school-to-work trajectories, included a two-step process. The first step was to construct individual school-to-work trajectories using the three ‘building blocks’ in sequence analysis: statuses, episodes and sequences. Episodes consist of the same status consecutively, and sequences consist of the ordered distribution of statuses over time. Sequences are ordered lists of elements (in this article various activity and maintenance statuses) which can be observed in register data linked to specific times, for example, the status ‘Normal income’ in a given month each year.
Twelve discrete, mutually exclusive statuses were defined (see Table 1). Using mostly monthly status information reduced the potential problem of overlapping statuses, which might be exacerbated by using only yearly information. These statuses were specified for each month for a total of 84 months (January 2011–December 2017) for the entire cohort. Information on education, employment and the various welfare benefit types is provided with start and end dates (i.e., information that will be used to recreate individuals’ complete school-to-work trajectories to measure the degree of precarity of school-to-work trajectories).
Status Alphabet.
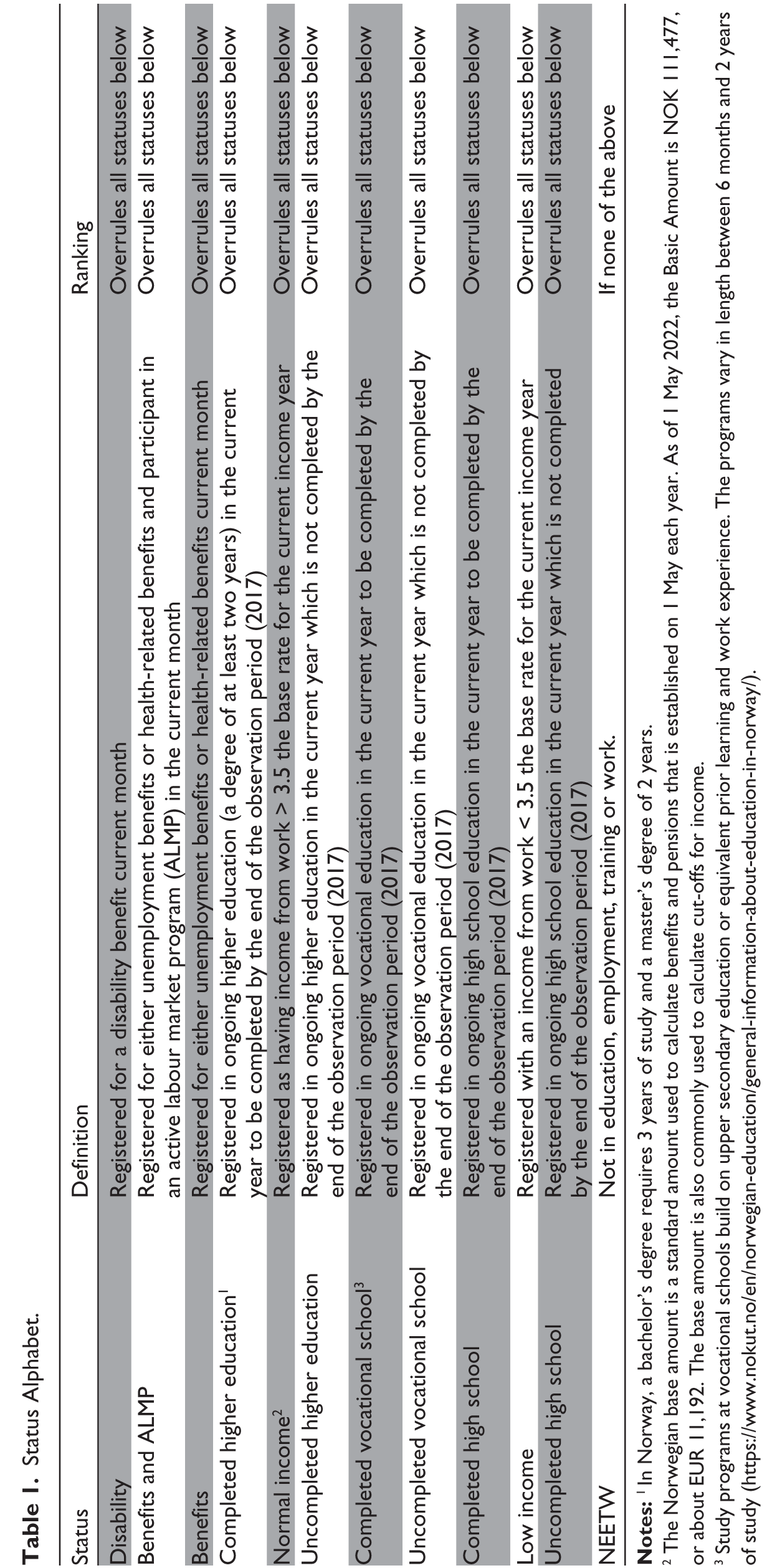
2 The Norwegian base amount is a standard amount used to calculate benefits and pensions that is established on 1 May each year. As of 1 May 2022, the Basic Amount is NOK 111,477, or about EUR 11,192. The base amount is also commonly used to calculate cut-offs for income.
3 Study programs at vocational schools build on upper secondary education or equivalent prior learning and work experience. The programs vary in length between 6 months and 2 years of study (
As shown in Table 1, ‘Disability’ takes precedence over all other simultaneous statuses; ‘Benefits and ALMP’ overrides all statuses except ‘Disability’; ‘Benefits’ overrides all statuses except the two mentioned above, and so forth. For practical purposes, ‘Disability’ is considered a permanent condition, thus, making it sensible to allow the ‘Disability status’ to override all other statuses. For all the other statuses, two main considerations come into play: firstly, whether we have access to monthly information, and secondly, statuses with higher education and employment or possible return to work were prioritized.
In the second step, the variable Degree of precarity of school-to-work trajectories was constructed using the badness index developed by Ritschard (2021), which measures the overall badness degree of individual sequences by considering the levels of undesirableness of the statuses. The index is constructed such that the weight of each status increases with the number of occurrences and recency, meaning that statuses occurring near the end of the sequence are given more weight when measuring the overall badness degree of the sequence. When using this type of weighting, a negative transition (e.g., from ‘Completed higher education’ or ‘Normal income’ to ‘Benefits’) is given a higher weight when the benefit episode is long-lasting and is near the end of the sequence. In other words, by using the badness index, our dependent variable can be defined as a measure of the overall precarity of individual school-to-work trajectories that captures downward social mobility. Before using the badness index to construct the dependent variable, we specified the rank order of the 12 statuses by deciding, first, the precarity degree of the statuses, and second, which statuses should be defined as equivalent. In our data, there are no non-comparable statuses (i.e., statuses considered to be neither better nor worse than any others and which therefore cannot be ordered). However, we have several equivalent statuses; these are considered to be equal and, therefore, have no hierarchy. Table 2 provides an overview of the included statuses, their order according to the degree of precarity, and which are considered equivalent.
Ranking the different statuses according to the degree of precarity was guided by attachment to the labour market and/or taking part in the educational system. This ranking is based on the assumptions that completing an education and/or having a strong attachment to the labour market are less precarious than not finishing an education or being on different types of benefits. These assumptions are both based on well-established knowledge and normative assessments based on the ‘work-first’ approach, which has guided Norwegian social policy for more than three decades.
The constructed continuous variable Degree of precarity of school-to-work trajectories was used as the dependent variable in the regression analysis; it takes the value 0 for a sequence made of a single episode in the least precarious status (‘Normal income’ or ‘Completed higher education’) and the value 1 for a single episode in the most precarious status (NEETW). In the data, the outcome ranges from 0.045 to 1 (mean = 0.32, SD = 0.23). The dependent variable was then computed into quartiles/four clusters of precarious trajectories: ‘not-at-all-precarious trajectory’ (including the lowest quartile values (0%–25%) of the degrees of precarious school-to-work trajectories), ‘somewhat precarious trajectory’ (25%–50%), ‘considerably precarious trajectory’ (50%–75%) and ‘highly precarious trajectory’ (75%–100%). This categorical variable was used in the descriptive statistics.
Degree of Precarity.
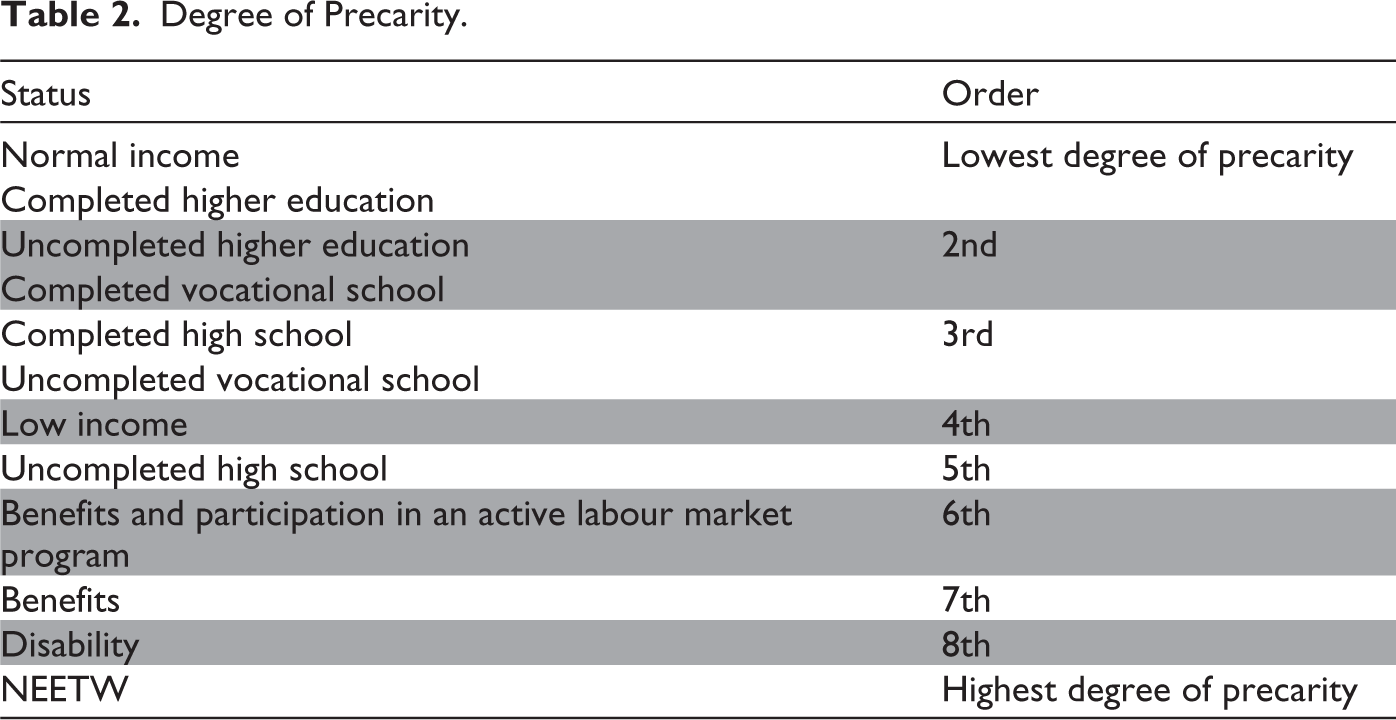
Table 3a illustrates sequences of ‘not-at-all-precarious trajectories’, and Table 3b illustrates examples of ‘highly precarious trajectories’.
Example of Sequences of Not-At-All-Precarious Trajectories Extracted from the 12th Percentile (Number of Months in Parentheses).

Example of Sequences of Highly Precarious Trajectories Extracted from the 88th Percentile (Number of Months in Parentheses).

Descriptive Statistics for Full Cohort, Male and Females (N = 56,967).
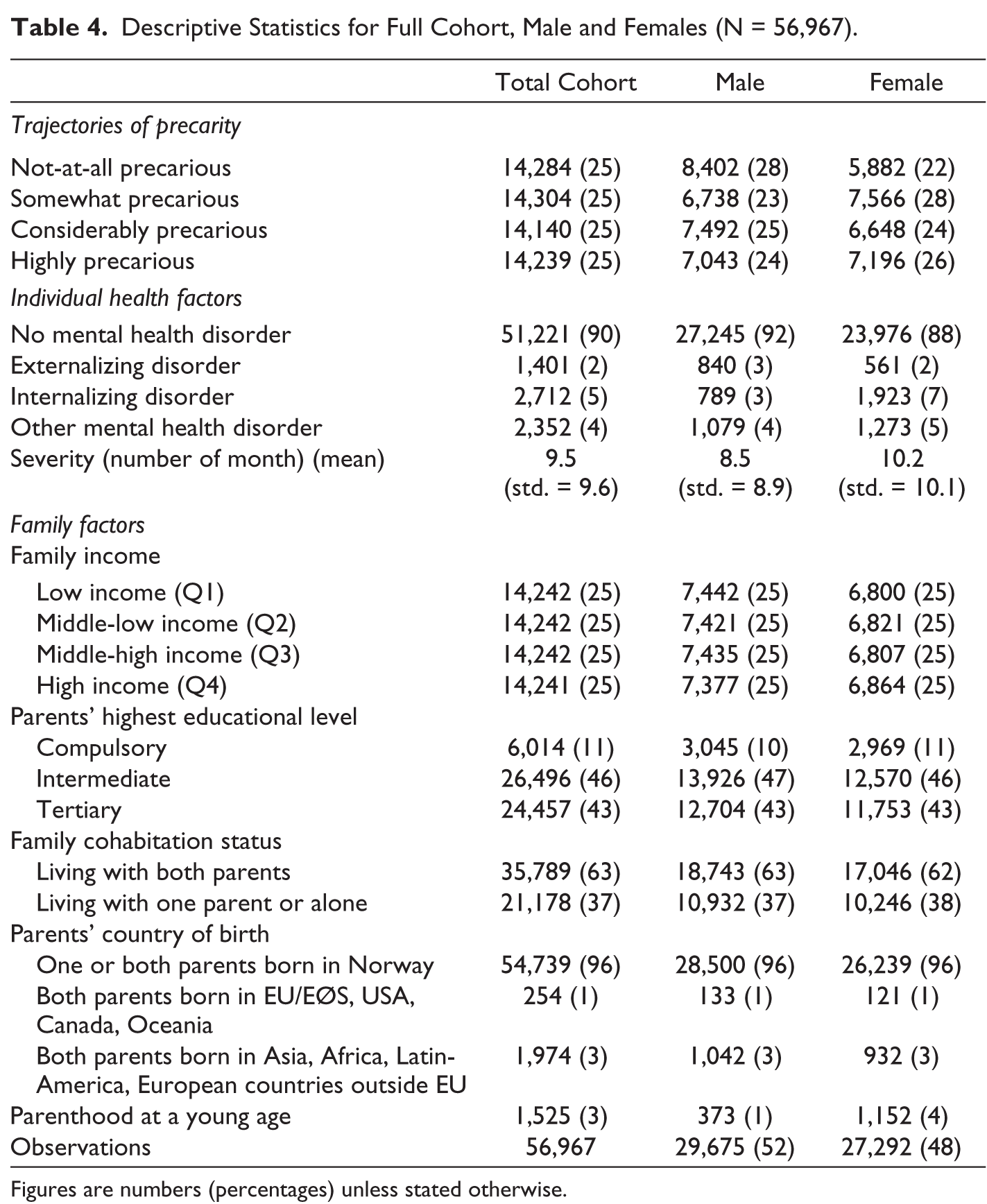
Figures are numbers (percentages) unless stated otherwise.
Mental Health Variables
Mental health is constructed as three health variables: internalizing, externalizing and other disorders (in the analysis, we focus on internalizing and externalizing disorders). The three variables were coded as indicator variables, taking the value 1 if the individual was registered with a psychiatric diagnosis in a specialist health service between 2008 and 2010.
Internalizing disorders include diagnoses of depression, anxiety, obsessive- compulsive and related disorders and trauma- and stressor-related disorders (ICD-10 codes: F32–F34, F38, F40–44 and F48). Externalizing disorders include diagnoses of attention-deficit hyperactivity disorder and conduct disorder (F90–F91). 1 The variable of other disorders includes all other MHDs, which are mainly unspecified disorders, in addition to eating disorders, developmental disorders and disorders due to psychoactive substance use.
Since it is well-documented that many adolescents experience multiple disorders concurrently (Costello et al., 2003), we account for comorbidity in our analysis 2 by restricting the three mental health variables to be not mutually exclusive (i.e., individuals can appear in several disease categories simultaneously).
We identified the number of months the individual was registered in the NPR from 2008 to 2010 and constructed the continuous variable Number of months in psychiatric services.
Variables of Socioeconomic Background and Family Factors
Equalized household income was constructed for a 5-year period (2008–2012) using the EU standard (first adult = 1.0, next adult = 0.5 and children under 17 in the household = 0.3). Next, the average household income over the five years was computed as quartiles: high income, middle-high income, middle-low income and low income. Parental education was taken from SSB’s education registry and includes information about the educational level of either the parent with the highest education level or the only parent present, measured in 2008. A categorical variable was then constructed: low (compulsory), intermediate (upper secondary and post- secondary non-tertiary) and high (tertiary). Parents with missing information were included in the low category. Using the household identification number retrieved from SSB, we learned whether the adolescent lived with both parents, with one parent or alone in 2008. The variable was dichotomized into Living with both parents or Living with one parent or alone. Parents’ country of birth was grouped into three categories: one or two Norway-born parents; two foreign-born parents from the EU/EØS, the United States, Canada, Australia or New Zealand; or two foreign-born parents from Asia, Africa, Latin America or Europe except the EU/EØS. The last included variable, Parenthood at a young age, is a measure identifying those adolescents who became a parent up until 2012 (at the age of 20).
Statistical Analysis
First, the analytic procedure consisted of descriptive statistics investigating how educational, work and welfare statuses in months 42 and 84, respectively, were distributed in four clusters of precarity. Second, descriptive analysis was conducted to explore the distribution of individual background characteristics in the clusters. All descriptive analysis was gender stratified. Third, linear multiple regression was conducted in two steps to examine associations between MHDs, family background and the degree of precarity of school-to-work trajectories, stratified by gender. In Model 1, we estimated the association between externalizing and internalizing disorders, respectively, and the degree of precarity of school-to-work trajectories, controlling for the comorbidity of other MHDs, the number of months in psychiatric services, parents’ country of birth, family cohabitation status, young parenthood, and household income/parental educational level. In Model 2, we include interaction terms between MHDs and household income and parental educational level, respectively, to investigate the moderating effect of family background on the association between MHDs and the degree of precarity of school-to-work trajectories.
To better understand the substantial effect/magnitude of the associations in the regression analysis, we constructed the degree of precarity of school-to-work trajectories as percentiles (that is, 100 groups based on the score of the dependent variable) (see Supplementary Material, Table A1). This percentile version of the dependent variable is called the ‘percentile index’. Thus, those in the first percentile of the index have the least precarious school-to-work trajectories, whereas those in the 100th percentile have the most precarious school-to-work trajectories. This allows us to ‘convert’ the regression coefficients of the outcome variable (values 0–1) into percentiles on the percentile index (values 1–100), making it easier to interpret substantial changes in the degree of precarity of school-to-work trajectories.
Results
Descriptive
Tables A2–A5 in the Supplementary Material, show the gender-stratified distribution of educational, work and welfare statuses of the individuals in the four clusters of precarity, measured, respectively, in the middle (i.e., in July 2014 [month 42]) and at the end of the observation period (i.e., December 2017 [month 84]).
On the not-at-all-precarious trajectory, everyone has a ‘normal income’ or ‘completed higher education’ status in months 42 and 84 for both genders. In the highly precarious trajectory for boys, in the middle of the observation period, 46% have the status ‘low income’, 26% receive ‘benefits’ or ‘benefits and ALMP’, 2% are on ‘disability’ and 11% are ‘NEETW’. In month 84, the ‘low income’ status has increased to 56%, ‘benefits’ or ‘benefits and ALMP’ have decreased to 16%, while the proportion who are on ‘disability’ or ‘NEETW’ has increased to 8% and 13%, respectively. For girls on a highly precarious trajectory, 50% were registered as ‘low income’ in month 42, and by month 84, the number had increased to 60%. In month 42, 27% have the status ‘benefits’ or ‘benefits and ALMP’, 2% are on ‘disability’ and 7% are ‘NEETW’. In month 84, ‘benefits’ or ‘benefits and ALMP’ decreased to 19%, while ‘disability’ and ‘NETTW’ increased to 6% and 10%, respectively.
Tables A6 and A7 in the Supplementary Material present the background characteristics of the individuals in the four clusters of precarious trajectories stratified by gender. Of boys diagnosed with externalizing disorders, 60% are on a highly precarious trajectory; for internalizing disorders, the proportion is 53%. Of girls diagnosed with externalizing disorders, 69% are on a highly precarious trajectory, and for internalizing disorders, the proportion is 55%. Both boys and girls from low-income families are overrepresented in the highly precarious trajectory (37% vs. 42%) compared to the not-at-all-precarious trajectory (21% vs. 14%).
Mental Health Disorders and Precarious School-to-Work Trajectories
In Tables 5a and 6a, Model 1 presents the regression results for the association between externalizing disorders and the degree of precarity of school-to-work trajectories, while Model 1 in Tables 5b and 6b presents the regression results for the association between internalizing disorders and the dependent variable; all models are stratified by gender. The results presented below are all adjusted for the comorbidity of other MHDs, number of months in psychiatric services, parents’ country of birth, family cohabitation status, young parenthood, and, respectively, household income and parental educational level.
The results show that both externalizing and internalizing disorders are associated with an increasing degree of precarity in school-to-work trajectories for both genders. Boys with externalizing disorders and in contact with psychiatric services for 8.5 months 3 (the average for boys) have an estimated value of the degree of precarious school-to-work trajectories of 0.46 4 (Table 5a) and 0.47 (Table 6a), holding all other included variables constant. By comparing the estimated value with the corresponding score in the percentile index (see the statistical analysis section), we find that boys with externalizing disorders are in the 77th percentile, that is, on a ‘highly precarious trajectory’. Boys with internalizing disorders in contact with psychiatric services for 8.5 months have an estimated value of 0.39 (Table 5b) and 0.41 (Table 6b), respectively, holding all other variables constant, which are located in the 72nd–73rd percentile of the percentile index––implying that these males are at the high end of ‘a considerably precarious trajectory’. In contrast, boys without an MHD are in the 62nd percentile (estimated value: 0.29/0.30), indicating that they are at the lower end of ‘a considerably precarious trajectory’.
Girls with externalizing disorders and in contact with psychiatric services for 10.2 months (the average for girls) have an estimated value of 0.5 (Table 5a) and 0.53 (Table 6a), respectively, holding all other variables constant, which is equivalent to being in the 80th–81st percentiles in the percentile index. Girls with internalizing disorders and in contact with psychiatric services for 10.2 months, holding all other variables constant, are in the 77th (estimated value 0.46, Table 5b) and 78th (estimated value 0.49, Table 6b) percentiles––implying that both groups are on a ‘highly precarious trajectory’. In contrast, girls without MHDs are in the 65th (estimated value 0.31, Table 5a/5b) and 68th (estimated value 0.34, Table 6a/6b) percentiles, respectively, indicating ‘a considerably precarious trajectory’.
Externalizing Disorders, Household Income and Precarious School-to-Work trajectories. Gender-Stratified LMR Analyses (N = 56,967).
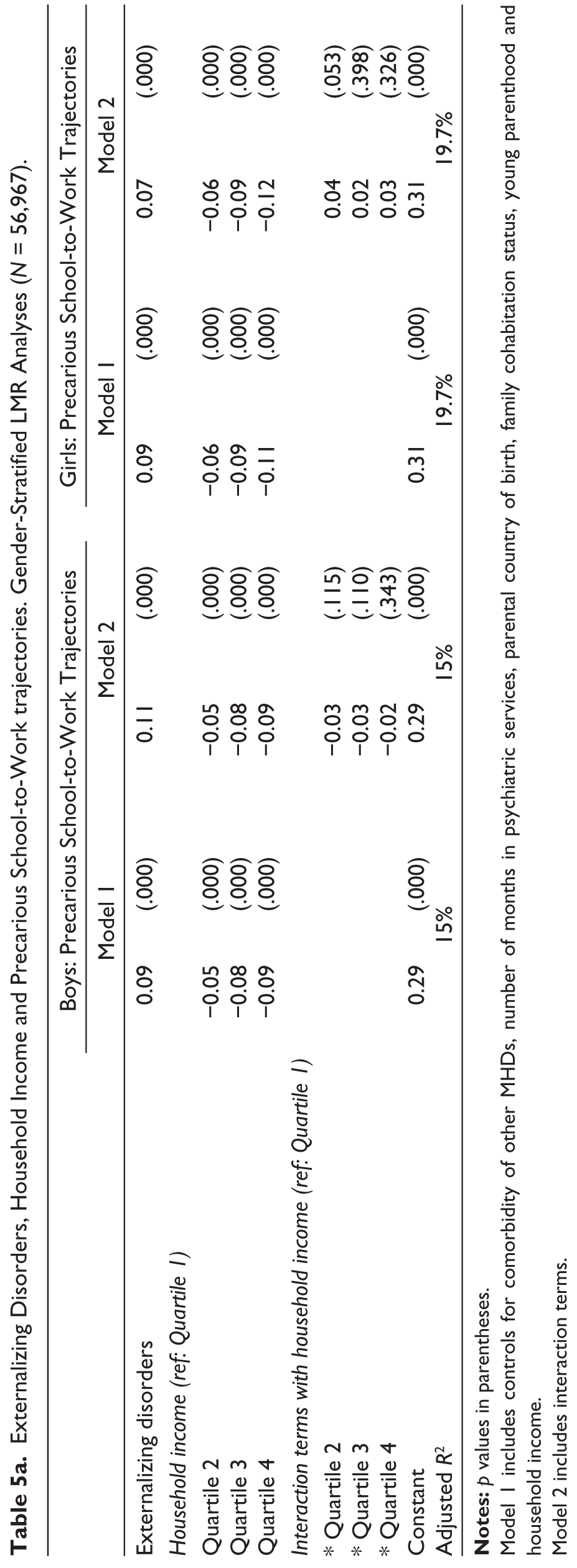
Model 1 includes controls for comorbidity of other MHDs, number of months in psychiatric services, parental country of birth, family cohabitation status, young parenthood and household income.
Model 2 includes interaction terms.
School-to-Work Trajectories and Interaction with Family Background
Model 2 (Tables 5a and 6a) includes additional interaction terms between externalizing disorders and family background (household income and parental educational level, respectively), while Model 2 (Tables 5b and 6b) includes interaction terms between internalizing disorders and family background. Starting with the boys, none of the interaction terms between externalizing disorders and household income are statistically significant, although the coefficients of the interaction terms are negative, implying that boys with externalizing disorders from high-income families are ‘buffered’ against entering precarious school-to-work trajectories relative to boys from low-income families. The interaction term between externalizing disorders and high parental educational level is statistically significant, indicating that boys with externalizing disorders with high-educated parents are in the 57th percentile 5 (i.e., the low end of ‘a considerably precarious trajectory’), while those with low- educated parents are in the 72nd percentile (i.e., the high end of ‘a considerably precarious trajectory’.
Internalizing Disorders, Household Income and Precarious School-to-Work Trajectories. Gender-Stratified LMR Analyses (N = 56,967).
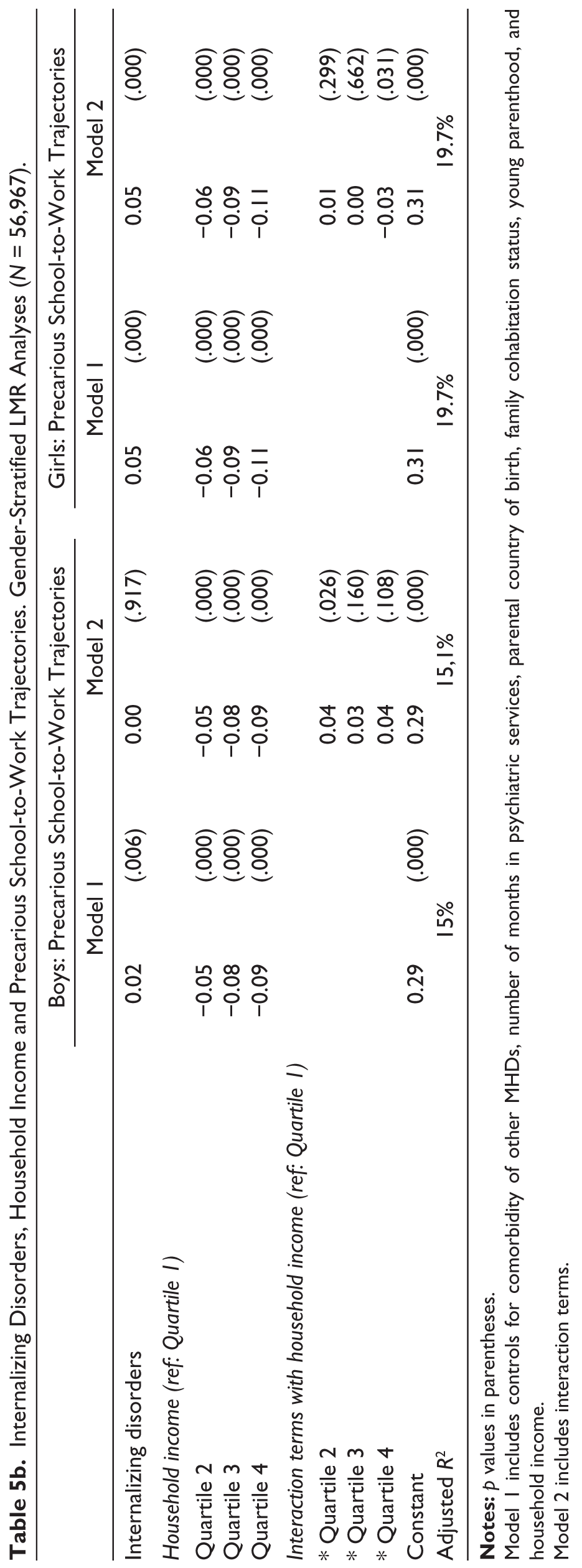
Model 1 includes controls for comorbidity of other MHDs, number of months in psychiatric services, parental country of birth, family cohabitation status, young parenthood, and household income.
Model 2 includes interaction terms.
Externalizing Disorders, Parental Educational Level and Precarious School-to-Work Trajectories. Gender-Stratified LMR Analyses (N = 56,967).
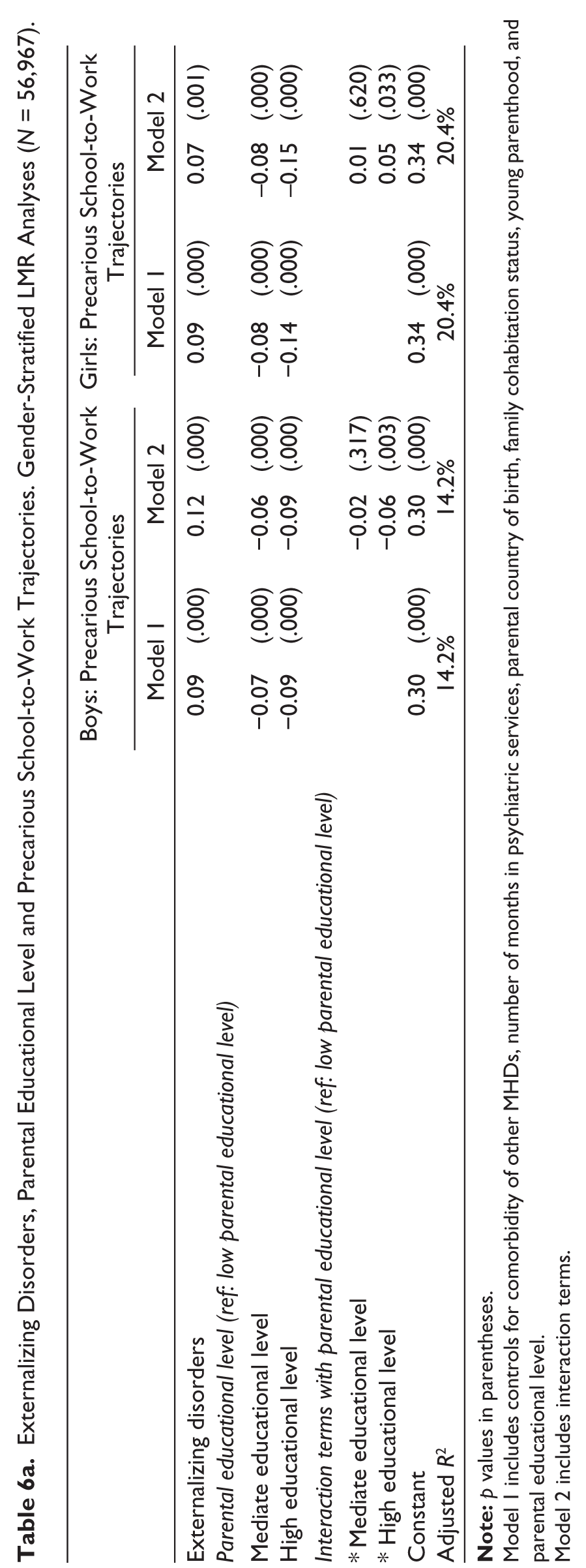
Model 1 includes controls for comorbidity of other MHDs, number of months in psychiatric services, parental country of birth, family cohabitation status, young parenthood, and parental educational level.
Model 2 includes interaction terms.
Internalizing Disorders, Parental Educational Level and Precarious School-to-Work Trajectories. Gender-Stratified LMR Analyses (N = 56,967).
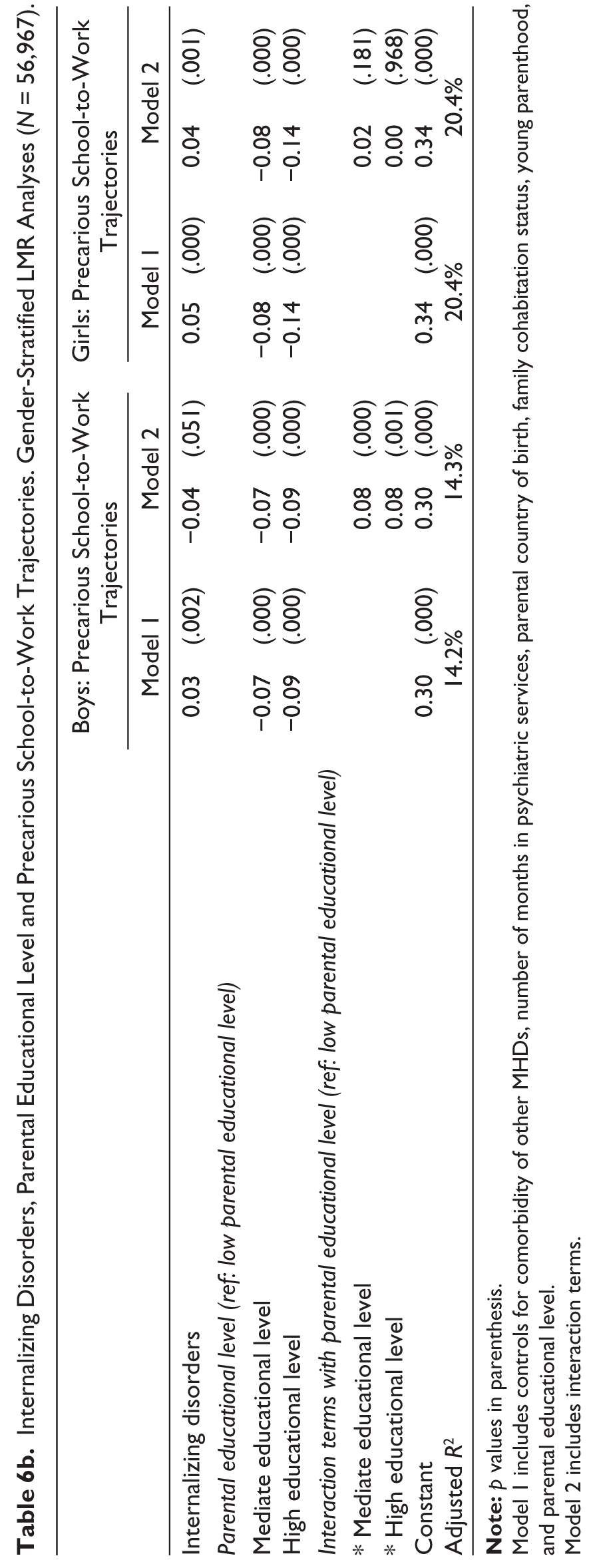
Model 1 includes controls for comorbidity of other MHDs, number of months in psychiatric services, parental country of birth, family cohabitation status, young parenthood, and parental educational level.
Model 2 includes interaction terms.
The interaction term between boys’ internalizing disorders and middle-low income is statistically significant with a positive coefficient (the interaction terms with middle-high and high income also have positive coefficients but are not statistically significant), indicating that middle-low income does exacerbate the association between boys’ internalizing disorders and precarious school-to-work trajectories compared to low-income boys with internalizing disorders. The interaction term between boys’ internalizing disorders and mediate and high parental educational levels, respectively, are statistically significant, with positive coefficients suggesting the same pattern: parental education higher than compulsory school exacerbates the association between boys’ internalizing disorders and precarious school-to-work trajectories.
Moving on to the girls, none of the interaction terms between externalizing disorders and family income are statistically significant, although all coefficients are positive, implying that high family income does not diminish the association between girls’ externalizing disorders and precarious school-to-work trajectories. The results for parental educational level show the same pattern as the coefficients of the interaction terms between externalizing disorders and mediate and high educational levels, respectively, both are positive and the latter significant. The interaction term between girls’ internalizing disorders and high-income families is statistically significant, indicating that girls with internalizing disorders from high-income families are in the 56th percentile (i.e. the low end of ‘a considerably precarious trajectory’), while girls from low-income families are in the 70th percentile (i.e. the high end of ‘a considerably precarious trajectory’). Conversely, the interaction terms between internalizing disorders and parental educational level do not seem to buffer the association between girls’ internalizing disorders and precarious school-to-work trajectories as these coefficients are positive/not different from the reference category; however, they are not significant.
In sum, the results indicate that coming from a high-SES family buffers the negative impact of boys’ externalizing disorders on entering precarious school-to-work trajectories, whereas the association between boys’ internalizing disorders and the degree of precarity of school-to-work trajectories is exacerbated among those with wealthier and better-educated parents, although not to a statistically significant degree. For girls, high family SES seems to exacerbate the association between externalizing disorders and precarious school-to-work trajectories. Regarding girls’ internalizing disorders, high household income buffers the negative impact of internalizing disorders on precarious school-to-work trajectories, whereas high parental educational level has an equal/exacerbating effect on the association between internalizing disorders and precarious school-to-work trajectories.
Discussion
First, the descriptive results show that the boys and girls with MHDs are overrepresented in the highly precarious trajectory compared to the other three. Externalizing disorders are overrepresented compared to internalizing disorders in the highly precarious trajectory for both genders. The regression analysis reveals a similar pattern: both internalizing and externalizing disorders are associated with a higher degree of precarity of school-to-work trajectories after controlling for the comorbidity of other MHDs, the number of months in psychiatric services, parents’ country of birth, family cohabitation status, young parenthood and household income/parental educational level; however, the association is more pronounced for externalizing disorders than for internalizing disorders. This result accords with previous research finding that externalizing disorders have a stronger negative impact on educational and employment status than internalizing disorders (Evensen et al., 2016; Hetlevik et al., 2018; Veldman et al., 2015). From a gender perspective, we found similar effects of the externalizing and internalizing disorders on the degree of precarity of school-to-work trajectories. This finding contradicts previous studies showing that internalizing disorders compromise only girls’ educational and work outcomes (Fletcher, 2013, 2008) but is consistent with studies finding the associations of both externalizing and internalizing disorders on educational outcomes to be quite similar for both genders (Jensen et al., 2021; Simson et al., 2021).
Second, turning to the moderating effect of family SES on the association between MHDs and precarious school-to-work trajectories, the results reveal interesting gender differences. For boys, high family SES seems to protect against the negative impact of externalizing disorders on a precarious school-to-work trajectory; however, this buffering effect did not apply to boys with internalizing disorders. In fact, the negative impact of internalizing disorders on the degree of precarity of school-to-work trajectories was the highest among boys with mediated and high parental education compared to boys with low-educated parents. Conversely, privileged girls with externalizing disorders seem to suffer an equal or even greater risk of entering a precarious school-to-work trajectory relative to less-privileged girls with this type of disorder. Regarding girls’ internalizing disorders, the picture is a bit more ambiguous; high family income seems to protect against the detrimental effects of internalizing disorders upon entering a precarious school-to-work trajectory, whereas high parental education does not show the same compensating effects. Thus, according to the two competing theoretical approaches, the CAM and the Blaxter hypothesis, the latter approach is supported for adolescents with gender-atypical disorders (i.e., boys with internalizing disorders and girls with externalizing disorders), suggesting that these otherwise advantaged adolescents are prevented from utilizing family resources and, therefore, suffer an equal or even greater risk of entering a precarious school-to-work trajectory relative to less-privileged adolescents with this type of mental disorder. Conversely, the CAM applies to boys with gender-typical disorders (i.e., externalizing) and, to some degree, to girls with gender-typical disorders (i.e., internalizing), indicating that advantaged families can use their resources to counteract their children’s disadvantages, minimizing their risk of entering precarious school-to-work trajectories.
Undoubtedly, our results underscore the importance of gender-stratified analysis to capture a more nuanced picture of the potential moderating effects of family background. However, most previous research investigating the interplay between externalizing and internalizing disorders, family background and school-to-work trajectories employs mixed samples (Brekke & Reisel, 2017; Evensen et al., 2016; Jackson, 2009; Mikkonen et al., 2020), which could be one explanation for the varied results of these studies.
A possible explanation for the observed gender differences might stem from the skewed distribution of diagnoses across genders. It appears that girls with gender-atypical disorders are referred to specialist healthcare less often even though they have an externalizing disorder (ADHD Norge, 2021; Holthe & Langvik, 2017; Stave, 2022), whereas, for boys, the situation appears to be the opposite: findings show that male adolescents with high depression scores are less likely to be diagnosed as depressed or to receive treatment (Fletcher, 2008). This underdiagnosis can be explained by, among other things, the fact that symptoms appear differently in boys and girls. Therefore, adolescents with gender-atypical disorders might be referred to treatment later than peers with gender-typical disorders. Thus, the mental health of boys and girls with gender-atypical disorders might be poorer when they finally obtain professional help, reducing the scope for family resources to make a difference, which might explain our results. From a policy perspective, this underscores the need for increased awareness of gender differences in symptoms of, e.g., ADHD and depression, both in the primary and specialist healthcare sectors, so that everyone can receive the right diagnosis and the treatment they are entitled to, irrespective of disorder type.
Related to this, conflicts between MHDs and gender norms and expectations could be another possible explanation for the gendered results. Stereotypical perceptions of ‘femininity’ involve characteristics such as being empathetic, good with relationships, nice and obedient, but girls with externalizing disorders displaying disruptive, hyperactive, impulsive or disorganized behaviours risk violating expectations of gender (Holthe & Langvik, 2017; Quinn, 2005). Consequently, females experiencing externalizing disorders could struggle with feelings of failure to fulfil the gender role expected of them by family and society (Quinn, 2005). In contrast, adolescent boys with internalizing disorders with symptoms of sadness and vulnerability risk violating traditional perceptions of masculinity, such as showing strength and avoiding emotions and perceived femininity (Coleman, 2015). Thus, adolescents with gender-atypical disorders may fail to fulfil expected gender roles and thus experience a double burden as they not only must cope with a mental disorder but also risk experiencing increased self-stigmatization and shame. This could explain why an advantaged family background has no compensating effect on gender- atypical disorders. Further research should investigate the mechanisms behind our gendered results in greater depth.
The current study is one of few investigating the interplay between adolescent MHDs, family background and school-to-work trajectories using population-covering registry data to provide reliable information on education, income, benefits and other demographic factors. Another advantage of the current study is that our objective measure of MHDs retrieved from patient registries is not biased by non-response, which otherwise can be a problem in survey data investigating mental illness.
However, the selection of specialist healthcare services is well-documented as low-SES individuals tend to consult specialist healthcare less than high-SES individuals, causing underreporting of mental disorders for this group (Godager & Iversen, 2013). Thus, the severity of MHDs might differ between the two groups as high-SES adolescents contact specialist healthcare with milder disorders than low-SES adolescents, which could bias our results for the effects of parental buffering. Under any circumstances, policymakers should prioritize school health services available at all times as these offer a unique opportunity to capture mental health problems in young people at an early stage, regardless of family socioeconomic background, thus contributing to reducing social inequality in healthcare service use.
A second limitation is that we lack information about specialist healthcare diagnoses before 2008 due to data limitations. As the average age of onset of behavioural (age 10), mood (age 14) and anxiety (age 9) disorders (Veldman et al., 2017) occur before the beginning of our observation period, individuals with early adolescent onset are likely to be followed up by a GP and thereby end up in the control group of the study. This could result in an underestimation of the observed impact of MHDs on the degree of precarity of school-to-work trajectories.
Third, the construction of the degree of precarity of school-to-work trajectories might be biased by gender-specific structures of the Norwegian institutional context. Well-paid full-time jobs that do not necessarily require higher education (i.e., in the building and construction industry) are male-dominated, whereas typical jobs for low-educated women are in the public sector (e.g., health and teaching), offer low pay and are often part-time. Conversely, in the educational system, more women than men complete higher education. However, in the face of mental illness, girls could lose their educational advantage and find fewer opportunities in the labour market. Thus, in the construction of degrees of precarity of school-to-work trajectories, girls with mental illness could be at particularly high risk of ending up in a highly precarious trajectory, which may bias the results.
Finally, even though parent education and income are regarded as the most common SES proxies (Ware, 2019), we are unable to draw conclusions about the mechanism driving the observed moderating effects of family SES. Thus, future research should further investigate the dimensions/mechanisms of family SES at play in the intertwined relationship between MHDs, school-to-work trajectories and gender.
Conclusion
The aim of the present study was to examine the impact of adolescent boys’ and girls’ internalizing and externalizing disorders on the precarity of school-to-work trajectories and how family background moderated these associations. Compared to previous studies relying on measures of single status transitions, an advantage of our study is the use of the badness index developed by Ritschard (2021), allowing us to explore school-to-work trajectories as a complex process in the life course capturing the evolution of social position over time. The results, based on high-quality registry data, show that adolescent MHDs are a risk factor for entering precarious school-to-work trajectories, implying the cruciality of supporting this group of vulnerable youth in this lifecycle phase to minimize the ‘scarring’ effects of future employment opportunities and earnings (OECD, 2019). Moreover, we found that high family SES compensates for the negative impact of boys’ externalizing disorders and partly for that of girls’ internalizing disorders, amplifying existing inequalities in school-to-work trajectories. Interestingly, adolescents from privileged families with gender-atypical disorders (i.e., boys with internalizing and girls with externalizing disorders) seem to suffer an equal or even greater risk of entering precarious school-to-work trajectories than adolescents from less-privileged families. In conclusion, the study broadens current perspectives on how social inequality in school-to-work trajectories is a multifaceted and interrelated process associated with differentiation in type of mental disorder, gender and social class. By broadening these perspectives, the paper draws attention to the diversity of young people and the complexity of their problems, which social policy must act upon to ensure successful trajectories from school to work for as many young people as possible.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The work was undertaken as part of the C-LIFE and WELLIFE projects, funded by Nordforsk [grant numbers 75970 and 83540].