
Abstract
High level of mental health problems are a critical concern among youth experiencing or at-risk of homelessness. Using data from a randomized controlled trial on Housing First in Canada, this study examined the risk factors and protective resources associated with mental health recovery among 215 homeless youth with mental illness at baseline and at a 24-month follow-up. At study entry, higher levels of recovery were associated with a lower number of adverse childhood experiences, less frequent presence of mental health symptoms, higher level of satisfaction with social relationships, and a higher level of psychological integration at baseline. At 24-months, a lower frequency of experiencing mental health symptoms and a higher level of psychological integration were associated with a higher level of recovery. The study’s findings highlight the importance of protective resources, notably having supportive social relationships and a sense of belonging in the community as contributors to mental health recovery
Mental health recovery is a personal process wherein individuals with mental illness can live satisfying and meaningful lives in the community (Davidson et al., 2005; Substance Abuse and Mental Health Services Administration [SAMHSA], 2012). A sense of empowerment, hope, identity, meaning and purpose, and a renewed sense of self are central to many definitions of recovery (Corrigan et al., 1999; Davidson et al., 2005; Ellison et al., 2018; Shanks et al., 2013; van Weenghel et al., 2019). Researchers emphasize that the recovery process differs for youth from adults (Lavik et al., 2018; Rayner et al., 2018). Thus, it is imperative to understand how the realities of youth experiencing homelessness affect their recovery journeys.
Youth homelessness is a complex social problem compounded by the pivotal developmental stage of adolescence. It is multidimensional, impacted by individual risks, system failures, and structural factors. In contrast to adults experiencing homelessness, youth may lack the necessary skills to live independently. System failures include barriers to accessing public support and services, and inadequate transitions from the child welfare system, correctional services, or hospitals (Dworsky et al., 2013; Fowler et al., 2017). Structural factors such as poverty, stigma, discrimination, and the scarcity of affordable housing can also play a role in youth homelessness (Sample & Ferguson, 2020).
Youth comprise approximately 20% of the homeless population in Canada and the United States (Duchesne et al., 2019; Henry et al., 2021). High levels of mental illness, problematic substance use, and suicidality are among the most prominent risk factors for youth who are homeless (Cronley & Evans, 2017; Narendorf et al., 2017; Perlman et al., 2014). In a recent pan-Canadian study of 1,363 youth experiencing homelessness, 74% reported experiencing mental health symptoms and high levels of distress (Kidd et al., 2021). Further, approximately one-third had at least one suicide attempt and have been hospitalized for a drug overdose.
There is limited research on the recovery processes of youth with mental illness who have experienced homelessness and housing instability. Padgett, Smith, et al. (2016) highlight the adversities associated with homelessness (e.g., victimization, social exclusion, and incarceration) that complicate the recovery processes of adults experiencing homelessness. However, compared to adults, distinct factors set youth experiencing homelessness apart, marked by the challenges associated with transitioning to adulthood (Barker et al., 2015; Gurdak et al., 2022).
Despite the limited research on mental health recovery among youth experiencing homelessness, we can draw comparisons from the literature on youth with mental illness and homeless adults with mental illness. Notably, mental health symptoms and physical health impairments have been found be negatively associated with recovery (Ecker et al., 2012; Kerman et al., 2019; Stumbo et al., 2015). The instability youth face interferes with their ability to navigate developmental stages, such as being a student, finding a career path, and making major life decisions surrounding relationships (Clark & Unruh, 2009).
Being integrated physically, socially, and psychologically in one’s community is a fundamental human need and a determinant of mental well-being, regardless of age (Baumgartner & Susser, 2013). Physical integration refers to having access to and participation in community activities, social integration refers to having supportive individuals one can rely on, and psychological integration refers to feeling like you belong to your community. Many youth rely on social networks for housing, day-to-day survival, and emotional support (Fulginiti et al., 2022; Joly & Connolly, 2019; Kidd & Shahar, 2008; Miller & Bowen, 2020). Researchers have consistently found that community integration and social support are positively associated with mental health recovery (Dang, 2014; Ecker et al., 2012; Kidd et al., 2013; Kerman et al., 2019).
Among individuals with histories of homelessness, housing is foundational to establishing quality of life in the community that enables positive life changes (Kirst et al., 2014; Macnaughton, 2016). Meeting basic needs and having a stable home environment allows people to take action to address their health instead of being in a survival mode (Kirst et al., 2014; Macnaughton, 2016). Housing plays an instrumental role in mental health recovery. Homeless adults with mental illness identify stable housing as the first step toward rebuilding their life, experiencing a new sense of self, and becoming autonomous (Kirst et al., 2014).
The Current Study
This study addressed two research questions: (1) What are the predictors of recovery among youth with mental illness and lived experience of homelessness? and (2) What are the predictors of change in recovery over time among youth with mental illness and lived experience of homelessness? Predictors were categorized as risk factors and protective resources and informed by SAMHSA’s (2012) four-dimensional framework, which recognizes the importance of health, purpose, community, and housing in recovery.
Risk and protective factors are internal and external aspects considered to impact the ability of an individual to adapt. Whereas risk factors are understood to act as a barrier to adaptation, protective factors are expected to support adaptation over and above the impact of risk factors (Masten, 2001). Risk factors may include individual or family mental health difficulties, exposure to stressful life experiences (e.g., childhood abuse and maltreatment), and indicators of precarious life circumstances (e.g., low socioeconomic status and low education). Protective factors may include close relationships with trusted adults, close friends and romantic partners, self-control, and effective emotion regulation.
Researchers identified risk factors for achieving recovery. Experiencing trauma (e.g., abuse and neglect) before becoming homeless can derail healthy developmental trajectories (Coates & Mckenzie-Mohr, 2010, Grattan et al., 2022). It is therefore hypothesized that a higher number of adverse childhood experiences, the presence of mental health symptoms, and increased substance use are associated with lower recovery levels.
SAMHSA’s (2012) four-dimensional framework recognizes the critical importance of positive social relationships and adequate housing as contributors to recovery. Based on this framework and previous research (e.g., Baumgartner & Susser, 2013; Kerman et al., 2019, it is hypothesized that a higher level of satisfaction with social relationships, greater community integration, housing stability, and a higher level of satisfaction with one’s living situation is related to a higher level of recovery.
This study used data from the At Home / Chez Soi demonstration project, a multi-site 24-month randomized controlled trial of Housing First (HF) conducted in five Canadian cities. HF is a recovery-oriented approach to ending chronic homelessness among people with mental illness (Padgett, Henwood, et al., 2016). In contrast to treatment first approaches, HF provides immediate access to scattered-site housing selected by individuals and without pre-conditions (e.g., adherence to a treatment plan, abstaining from substance use) and mental health support focused on community integration in the form of Assertive Community Treatment or Intensive Case Management (Aubry et al., 2015; Stefancic & Tsemberis, 2007).
Methods
Participants
Participants were recruited for the trial from community organizations serving people who are homeless (e.g., emergency shelters and soup kitchens) in five Canadian cities: Moncton, Montreal, Toronto, Winnipeg, and Vancouver (Goering et al., 2011). Inclusion criteria were: (1) having a mental disorder as determined by the Mini International Neuropsychiatric Interview (Lecrubier et al., 1997); (2) being absolutely homeless (i.e., no fixed place to stay for the past seven or more nights) with no prospect of being able to regain stable housing within the next month or precariously housed (i.e., living in a rooming house and having had two or more episode of homelessness in the 12 months before entering the study); and (3) being 18 years of age or older (19 in Vancouver). Participants were randomized into two groups: HF and treatment as usual (TAU; i.e., access to all other health and social services available in the community). Further details about the trial are available in the study’s protocol (Goering et al., 2011).
Of the 2,255 individuals recruited, 215 were 18 to 24 years old (Canadian Observatory on Homelessness, 2016) and included in this analysis (58% in HF, n = 124; 42% in TAU, n = 91). Three participants died before the 12-month follow-up and were excluded from the 24-month analysis (N = 212).
Measures
Demographic characteristics
The Demographics, Housing, Vocational, and Service Use History Questionnaire (Mental Health Commission of Canada, 2010) was developed for the At Home/Chez Soi study and used to collect basic information about participants. Dichotomized data on gender (male/female), level of education (less than high school/high school or higher), and involvement in work (unemployed/employed), as well as age and duration of homelessness, were used in the present study.
Risk factors
Adverse childhood experiences (ACE) were examined using the 10-item ACE Questionnaire, assessing if participants experienced psychological, physical, and sexual abuse before age 18 (Felitti et al., 1998). Each item was scored dichotomously (yes/no), yielding a total score ranging from 0 to 10. The ACE Questionnaire had good internal consistency for this sample (α = .82).
The Colorado Symptom Index (CSI) is a 14-item measure that assesses the presence and regularity of psychiatric symptoms in the past month. The CSI uses a 4-point Likert scale, ranging from 0 (not at all) to 4 (at least every day). A total score was computed, with higher scores indicating an increased presence of mental health symptoms. The CSI has adequate test-retest reliability, content validity, and construct validity (Boothroyd & Chen, 2008; Conrad et al., 2001). Internal consistency for this sample was excellent (baseline α = .88; 24-month α = .9).
The Global Assessment of Individual Needs-Substance Problem Scale (GAIN-SPS; Dennis et al., 2006) was used to assess the presence of substance use. A total score for the past month was computed using four items and ranged from 0 to 4, with higher scores indicating the presence of more substance use problems in the past month.
Protective resources
The Residential Timeline Follow-Back (RTLFB; Tsemberis et al., 2007) was used to collect comprehensive information about people’s housing experiences over a given time, including the number of times moved, the reason for moves, types of residences lived in, and household composition. The RTLFB has good 1-to-2-week test-retest reliability and good concurrent validity, as assessed by the associations between agency and self-report (Tsemberis et al., 2007). The percentage of days in stable housing in the 3 months before the study was used to measure housing stability at baseline. The percentage of days across 24 months during the study was used to measure housing stability at 24 months.
The Community Integration Scale (CIS; Goering et al., 2011) is composed of two subscales independently assessing psychological (e.g., sense of belonging) and physical (e.g., participating in community events) integration. The psychological integration subscale has four items rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). A total score was computed, ranging from 4 to 20. The physical integration subscale examined community participation in the past month using seven dichotomous items. A total score from 0 to 7 was computed. Higher scores on both CIS subscales reflect greater community integration. The CIS underwent pre-testing and piloting to ensure the measure was relevant and applicable for people with serious mental illness (Goering et al., 2011). The internal consistency of this sample’s psychological and physical community integration subscales was fair (baseline αpsychological integration = .69, αphysical integration = .62; 24-month αpsychological integration = 68, αphysical integration = .62).
The Quality of Life Interview (QoLI-20; Uttaro & Lehman, 1999) is composed of 20 items assessing satisfaction with seven areas of one’s life (i.e., living situation, everyday activities, family, social relationships, finances, safety, and overall satisfaction with life). Items were scored on a 7-point Likert scale from 1 (terrible) to 7 (delighted). Only two subscales – (1) social relationships (4 items; range = 4–28; baseline α = .76; 24-month α = .81) and (2) living situation (single item) – were used as predictors in the present study.
Mental health recovery
A 22-item version of the Recovery Assessment Scale (RAS-22; Corrigan et al., 1999) was used to assess subjective ratings of recovery. Domains assessed by the RAS-22 included personal confidence and hope, willingness to ask for help, goal and success orientation, reliance on others, and freedom from illness symptoms. The measure used a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Items were summed to compute an overall score (range = 22–110), with higher scores reflective of greater mental health recovery. The internal consistency of the RAS-22 for the sample was excellent (baseline α = .88; 24-month α = .91).
Data Analysis
Hierarchal multiple regression models were fitted to examine the study’s two research questions. The predicted outcomes were overall ratings of recovery. For the model predicting recovery at baseline, predictor variables were entered sequentially in three blocks: (1) demographic characteristics: gender, level of education, and employment status; (2) baseline risk factors: frequency of mental health symptoms, presence of substance use problems in the past month and number of ACES (collected at the 18-month follow-up); and (3) baseline protective resources: quality of social relationships, level of physical integration in the community, level of psychological in the community, percentage of time stably housed in the past 3 months, and quality of their living situation.
For the model predicting recovery at 24 months, recovery scores at baseline were inputted as the first predictor to assess residual change over time. Risk factors and protective resources remained the same, though 24-month assessment scores were used with the exception of the ACE score that was collected at 18 months, and the percentage of time stably housed was based on the past 24 months. The intervention group was included with the demographic characteristics in the first block.
Assumptions of the regression model were not violated at baseline or 24-months. Multiple imputation was used to address missing data, ranging from 0.5% to 28.8%. Ten imputations, with 50 iterations each, were performed using a linear regression algorithm. Findings are presented using pooled estimates of the multiply imputed datasets. All statistical analyses were performed using SPSS 28.
Results
Sample Characteristics
The study sample comprised 215 youth between 18 to 24 years of age (Mage = 22.26; 61% male, 36% female). The characteristics of the sample are presented in Table 1. More than half of participants had a major depressive episode at baseline (51.2%), with 42.8% indicating moderate to high suicidality.
Demographic and Clinical Characteristics of the Study Sample (N = 215).
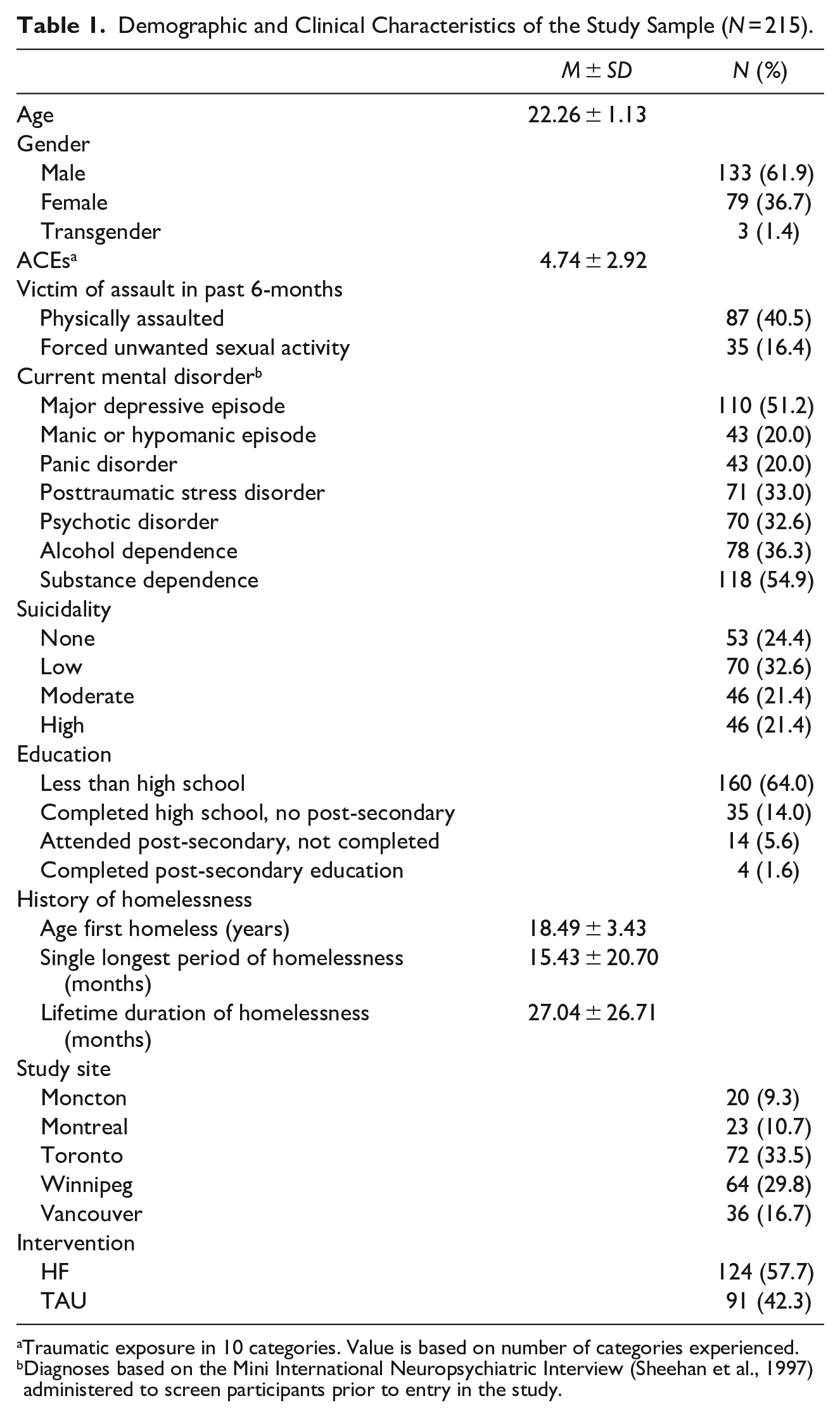
Traumatic exposure in 10 categories. Value is based on number of categories experienced.
Diagnoses based on the Mini International Neuropsychiatric Interview (Sheehan et al., 1997) administered to screen participants prior to entry in the study.
The mean rating of overall recovery at baseline was 79.40 (SD = 12.69) and 86.12 (SD = 12.93) at 24 months. The difference in recovery between baseline and 24-months was significant, t(425) = −5.42 (95% CI −9.16 to −4.28), p < .001, d = 0.52. The effect Baseline RAS-22 scores were also transformed into mean item scores as opposed to a sum (M = 3.62, SD = 0.58) to enable comparisons of the sample’s level of recovery to other research samples of people with mental illness.
Predictors of Recovery
Recovery at baseline
Results of the hierarchical multiple regression predicting recovery at baseline are presented in Table 2. Gender was significantly associated with subjective recovery (β = .15, p < .05), indicating participants who identified as women were more likely to report a lower level of recovery. Risk factors accounted for 20% of the observed variance of recovery, F(6,208) = 9.82, p < .001. A higher number of adverse experiences in childhood (β = -.18, p < .01) and an increased presence of mental health symptoms (β = -.36, p < .001) were associated with a lower level of recovery. Inclusion of protective resources in the regression model predicting recovery accounted for a further 9% of variance, F(11, 203) = 9.08, p < .001. A higher level of satisfaction with social relationships (β = .21, p < .01) and a higher level of psychological integration (β = .20, p < .01) were associated with a higher level of recovery.
Hierarchal Multiple Regression Predicting Recovery at Baseline.
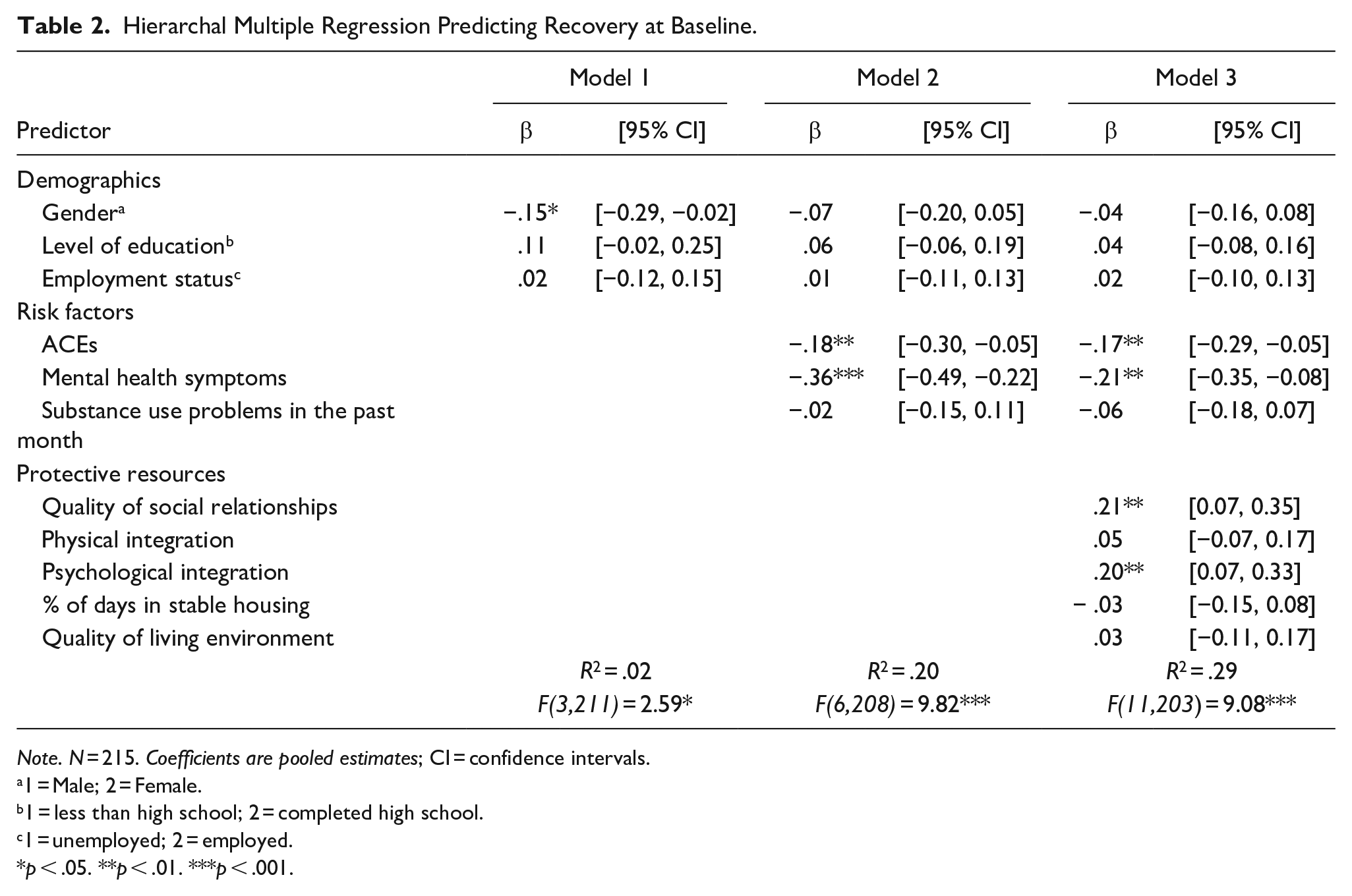
Note. N = 215. Coefficients are pooled estimates; CI = confidence intervals.
1 = Male; 2 = Female.
1 = less than high school; 2 = completed high school.
1 = unemployed; 2 = employed.
p < .05. **p < .01. ***p < .001.
Residual change in recovery at 24 months
Risk and protective factors predicting recovery at 24 months after controlling the level of recovery at baseline are shown in Table 3. Demographic characteristics and randomization to either HF or TAU did not significantly predict recovery, accounting for only 1% of the variance. The inclusion of risk factors was significantly associated with changes in recovery at 24 months (ΔR2 = .05, p < .001), with a greater presence of mental health symptoms (β = -.23, p < .01) being significantly associated with lower levels of recovery at 24 months. The inclusion of protective resources in the regression model accounted for another 8% of the variance, F(13,198) = 7.32, p < .001, with a higher level of psychological integration in the community (β = .20, p < .01) being associated with a higher level of recovery at 24 months.
Hierarchal Multiple Regression Predicting Recovery at 24-Months.
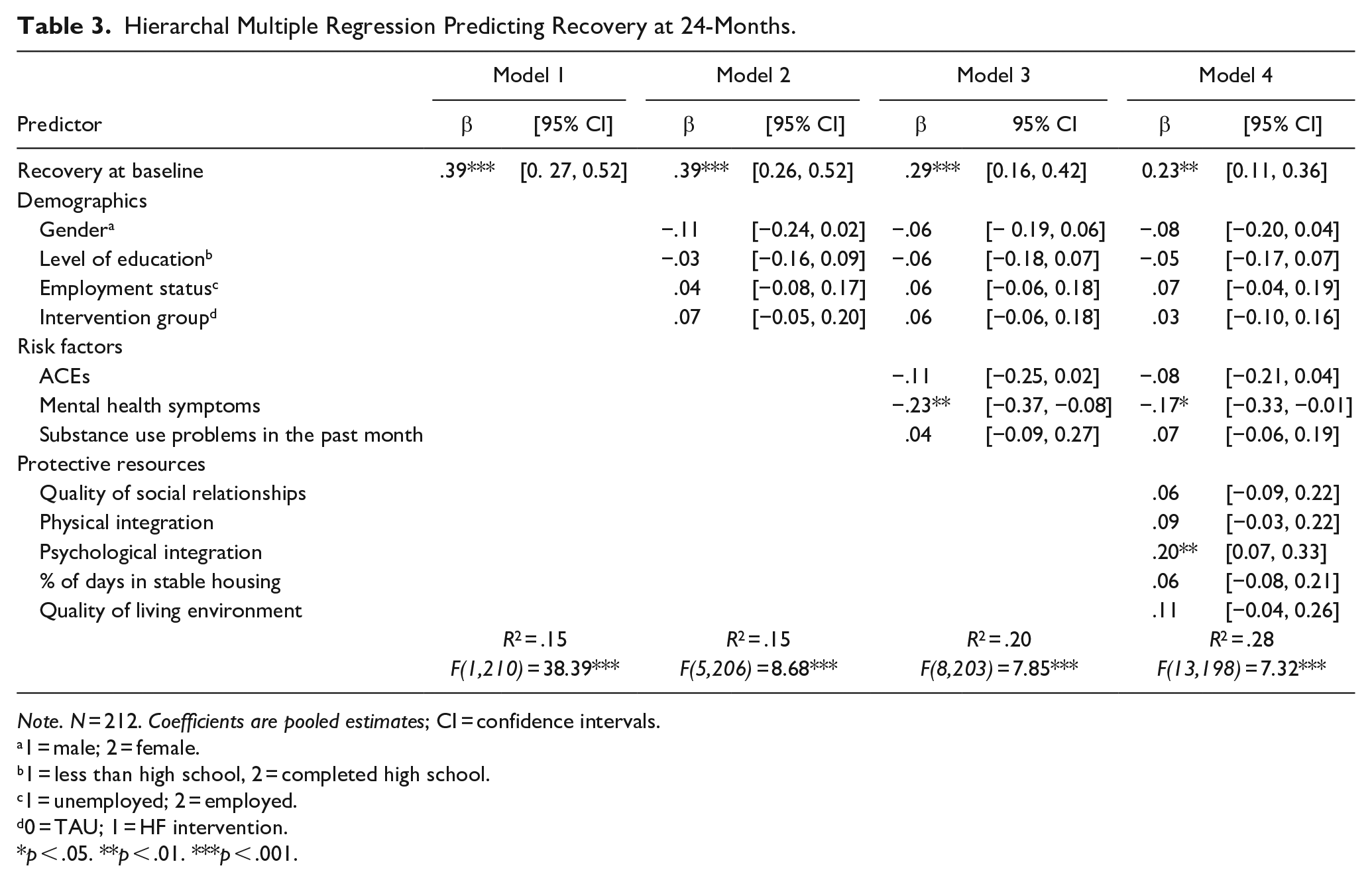
Note. N = 212. Coefficients are pooled estimates; CI = confidence intervals.
1 = male; 2 = female.
1 = less than high school, 2 = completed high school.
1 = unemployed; 2 = employed.
0 = TAU; 1 = HF intervention.
p < .05. **p < .01. ***p < .001.
Discussion
Results of this study suggest having experienced more ACEs and being satisfied with one’s social relationships are important predictors of recovery among youth with lived experience of homelessness and serious mental illness. Over time, psychological integration, which entails experiencing a sense of belonging in the community, emerges as a critical protective resource for improving feelings of recovery in the lives of youth who are homeless or unstably housed living with mental illness. A less frequent presence of mental health symptoms was also associated with a higher level of recovery and its improvement over time.
The baseline analyses showed cisgender women rated their recovery lower than cisgender men. According to Schwan et al. (2020), women are more likely than men to experience sexual exploitation, sex trafficking, and gender-based violence. Moreover, researchers have suggested that young women are more likely to remain in precarious housing due to unsafe living situations on the streets (e.g., increased risk of abuse or exploitation; Bretherton, 2017; Schwan et al., 2020).
The findings extend earlier research demonstrating that experiences of ACEs have profound negative implications for youth experiencing homelessness (Kidd & Shahar, 2008). It is well documented that exposure to ACEs is associated with suicidality, mental illness, substance use, and victimization (Liu et al., 2021). Given the prevalence of early trauma, providers need to be trained in trauma-informed care and programs to build trauma-informed principles into their services (Hopper et al., 2010). Intervention addressing early trauma is vital to prevent long-term impacts.
Timely and accessible assessment of mental health problems among youth is critical. In a recent large-scale meta-analysis, Solmi et al. (2021) found that the median age of onset for mental health disorders is 18. Findings from this study show that the increased presence of mental health symptoms have a significant negative relationship with mental health recovery among youth experiencing homelessness. Given this, increasing mental health services directed at youth and making them more easily accessible is essential.
The perceived quality of social support available to youth is an essential predictor of recovery among those experiencing homelessness. While some youth may continue relationships with friends acquired before becoming homeless and maintain contact with extended family, others may form social circles and support networks in the subculture of street life, referred to as street family (Bender et al., 2018; Frederick, 2019). Having shared experiences in these relationships provides the opportunity for support, validation, and safety. Peer support interventions are one approach for leveraging the benefits derived from shared experiences of homelessness while mitigating the potential harms of victimization (Kidd, 2019; K. Stewart & Townley, 2020). They enable building a community of young people with similarities in lived experience. The benefits of social support from youth who have navigated similar stressors and challenges are invaluable to youth who may feel ostracized from mainstream society (Kidd, 2019; K. Stewart & Townley, 2020).
Despite this group’s high rates of victimization, youth experiencing homelessness are less likely to seek help (Heerde & Pallotta-Chiarolli, 2020). Common barriers to seeking help include lack of support from a trusted adult, previous negative experiences and diminished trust in support services, individual shame, embarrassment, and stigma (Bender et al., 2018; Heerde & Pallotta-Chiarolli, 2020). Furthermore, individual barriers include denial of problems, pressure to focus on basic resources, and fears of not being taken seriously.
Psychological integration in the community among youth experiencing or at risk of homelessness has been an understudied area of research (Thulien et al., 2019). Based on the findings of this study, we can show that access to positive social relationships and a sense of belonging are protective factors associated with mental health recovery. A sense of belonging in the community continues to be a significant predictor of changes in recovery over time. This suggests that fostering community connection with peers, service providers, and family through interventions, such as family reconnection and school integration, targeted at youth experiencing homelessness may support mental health recovery while simultaneously offering tools and a network to help reintegrate themselves into society.
We did not find a significant relationship between housing, substance use, and recovery. Achieving stable housing may not be sufficient to effect recovery (Kozloff et al., 2016). Further, youth may not have received support targeted at improving psychosocial outcomes. Social support and psychological community integration are notable predictors of recovery; teaching life skills, supporting the confidence to live independently, and reducing loneliness and isolation are essential when considering housing interventions for youth.
When assessing the non-significant relationship between substance use and recovery, it is crucial to question the normative assumptions of adaptive versus maladaptive behavior (Kolar et al., 2012; Roebuck & Roebuck, 2016). Kolar et al. (2012) highlight that youth emphasize the importance of protecting peers and putting the safety of others above their own when discussing substance use. Due to their socioeconomic circumstances, drug dealing and stealing were seen as means of survival (Roebuck & Roebuck, 2016).
The study’s findings highlight the importance of protective resources for youth, such as having access to social support and experiencing a sense of belonging, in achieving mental health recovery. Findings from this study suggest youth would benefit from having a supportive network of friends and peers, natural mentors (i.e., extended family or non-kin relationships, such as teachers), and trusted service providers who can offer spaces for open communication, understanding, and connection (DuBois & Silverthorn, 2005). One avenue for achieving this would be integrating supports in HF that help youth return to school, a setting that can offer a sense of community, social support, and meaning and purpose.
While there is a lack of research on programs that support homeless youth to return to school, we can build on literature addressing barriers to education for youth experiencing homelessness. Ausikaitis et al. (2015) highlight accessibility needs for youth who have dropped out and want to return to school or are on the verge of leaving school, including transportation and having an environment of trust and respect. Schools’ involvement can also minimize feelings of isolation, increase community connection, and significantly impact subjective quality of life (Moses & Villodas, 2017; Thielking et al., 2017). M. Stewart et al. (2010) emphasize the desire for non-judgmental and understanding support regardless of the current circumstances.
Limitations and Future Directions
This study addressed a gap in the evidence on homeless youth, supporting the need to understand recovery for this unique and vulnerable population. Youth experiencing homelessness need to be credited for their ability to persevere and overcome their current situation, especially given the challenging developmental period in which youth navigate the transition to adulthood.
Our study has several limitations. Given the sensitivity of the measures, such as the ACEs questionnaire and the longitudinal nature of the project, there was a limitation of missing data. This was addressed using multiple imputation. At Home/Chez Soi aimed to test HF as an intervention for homeless adults of legal age with mental illness. Two limitations arise from the trial’s inclusion criteria: (1) The findings may not generalize to youth under the age of 18; (2) factors particularly important to this younger subgroup were not included in this study (i.e., sexual identity/orientation, the reason for leaving home).
Lesbian, gay, bisexual, transgender, queer, questioning, and two-spirit (LGBTQ2S) youth make up a disproportionate number of the homeless youth population in North America (I. A. Abramovich, 2012; Choi et al., 2015; Durso & Gates, 2012). LGBTQ2S youth comprise nearly 20% to 40% of the overall youth homelessness population (Durso & Gates, 2012; Kidd et al., 2021). Future research should investigate the link between mental health recovery among youth who self-identify as LGBTQ2S in the context of homelessness. Additionally, it would be beneficial to consider reasons for leaving home, as youth who have been forced to leave home have a greater risk of mental health difficulties than youth who decide on their own to leave home (A. Abramovich & Shelton, 2017).
Research on the effectiveness of HF with adults is abundant, but little has been done on the value of this approach for youth (Kozloff et al., 2016). Moreover, exploring how to effectively implement HF to address the developmental needs and life skills of youth experiencing homelessness is essential. Gaetz (2014) emphasizes that HF models adapted for young people must incorporate preconceived understandings of youth development, social, and legal needs. It is essential that the youth intervention does not simply mirror the adult models but rather be tailored to their needs and abilities. This can include improving communication and problem solving, rebuilding natural supports (i.e., family reconnection), and facilitating access to education and work opportunities, (Gaetz, 2014; Munson et al., 2017; M. Stewart et al., 2010).
The results of this study have several implications for service providers and policy advisors. It is suspected that programs and services aimed at early intervention for mental health will positively impact youths’ perceptions of personal confidence, prevent isolation, and increase willingness to ask for support when needed. Such interventions can include teacher and peer support, which fosters a sense of belonging, trust, and improvement in daily emotional affect (Altena et al., 2010; Griffin et al., 2019). For youth diagnosed with psychotic disorders, early psychosis interventions are effective in facilitating community participation, maintaining social networks, resuming normal social roles, and improving psychological well-being (Cotton et al., 2016). Risk factors and protective resources have been linked to recovery in youth experiencing homelessness, and services must be tailored to facilitate community support and connection.
Footnotes
Acknowledgements
The authors thank Jayne Barker (2008–11), Ph.D., Cameron Keller (2011–12), and Catherine Hume (2012–2013) Mental Health Commission of Canada At Home/Chez Soi National Project Lears, the late Paula Georing, Ph.D. the National Research Lead, the National Research Teams, the five site research teams, the Site Co-ordinators, and the numerous service and houinsg providers, as well as persons with lived experience who have contributed to this project and the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been made possible through a financial contribution from Health Canada provided to the Mental Health Commission of Canada. The Mental Health Commission of Canada oversaw the design and conduct of the study and has provided training and technical support to the service teams and research staff throughout the project. The views expressed herein solely represent the authors.