
Abstract
This article critically analyses and theoretically conceptualises the links between settler colonialism, planning and health. Based on the case of the Bedouin community in the Negev/Naqab, we argue that the production of settler colonial space has a profound impact on health, and should therefore be referred to as a specific category for analysing health disparities, simultaneously entangling territorial control and biopolitics towards indigenous communities. Furthermore, we suggest that this relationship between space and health constructs stigma that justifies and facilitates – in turn – the ongoing territorial control over the indigenous Bedouin population in Israel. By reviewing existing data on health and planning, especially in relation to infrastructure and access to services, we contribute to the growing literature on the nexus of settler-colonialism/health with urban and regional planning. Importantly, throughout this paper we refer to the Bedouin localities as part of the production of urban territory, illuminating the urban as a multidimensional process of political struggle, including the metropolin informal fringes.
Introduction
In 2005 a petition was filed to the Israeli Supreme Court of Justice on behalf of Ennas Al-Atrash by the Association for Civil Rights in Israel and the Physicians for Human Rights. Ennas was a three-year-old childliving in an unrecognised Bedouin villagewho was diagnosed with aggressive Rhabdomyosarcoma cancer in her chest. Following sessions of chemotherapy and surgery for the partial removal of the tumour, Ennas needed constant antibiotic treatment and injections to strengthen her immune system; medication that must be stored at temperatures of 0°C–4°C. A hygienic, air-conditioned environment was also essential for her recovery, especially during the hot summer days. 1 The appeal to the Supreme Court was filed against the Minister of Health, the Minister of National Infrastructure and the Minister of Interior Affairs. It demanded that the child’s homebe connected to the electricity distribution network in order to allow herproper healthcare. The petitioners emphasised that the state, in refusing to provide the girl’s home with an electricity supply, had violated its commitment to protect children and to place the welfare of the child above bureaucratic, land and ideological considerations.
The Supreme Court rejected the appeal, and accepted the state’s proposal to provide the child’s family with 16,000 NIS (3500 GBP) in order to purchase fuel for a generator owned by their neighbours, which the family had been using. Although the judges stated that this solution was far from adequate, they did not obligate the state to connect the home to the electricity network, claiming that the child’s parents had chosen to live in an unrecognised village ‘knowing that they would therefore not be able to connect to basic infrastructures’. 2 However, in their decision the judges did not ignore the claims of the petitioners, that the child’s right to life overpowers planning and bureaucratic considerations, and declared their ‘hope and prayer that [Ennas] will fully recover’. 3 The court recommended that the family move from their home in an unrecognised village to a formally planned township in which houses and proper infrastructure are provided. Ennas and her parents were therefore left to face her illness and treatment on their own.
The above case illustrates the entanglement of orientalist stigmatisation and spatial control that characterises Israel’s attitude towards the Bedouins; constructing the image of the Bedouins as irrational invaders who chose to live in unrecognised, un-serviced space. Such linkage between illegality and backwardness is central in stigmatising the Bedouins, exemplified in Moshe Dayan’s (former Chief of the General Staff in the IDF, then the Minister of Agriculture) famous quote from 1963: The Bedouins should be made into urban workers […]. It is indeed an acute transition. It means that the Bedouin will not live on his lands with his herds but become a city man that comes home in the afternoon and wears slippers. His children will get used to a father that wears trousers, without a Shabriyah, and does not remove lice in public. They will go to school combed with parted hair. It will be a revolution, but it can be fixed within two generations. Not by force but with governmental guidance this reality named Bedouins – will be gone. (in Abu-Saad, 2004. Emphasis added)
Though the case of Ennas Al-Atrash is not unique, and other instances show similar characteristics (Filc, 2009: Chapter 3), it is used here as an illustration of our main argument, namely that the production of settler colonial space has a profound impact on health and should therefore be referred to as a specific category for analysing health disparities, simultaneously combining territorial control and biopolitics towards indigenous communities (Shalhoub-Kevorkian, 2014; Wolfe, 2006). Furthermore, we argue that this relationship between space and health constructs stigma that justifies and facilitates – in turn – the ongoing territorial control over the indigenous Bedouin population in Israel. 4
In this paper we therefore illustrate the profound impact the production of settler colonial urban territory has on populations’ health using the case study of the Bedouins in the Negev (in Hebrew)/Naqab (in Arabic) in Israel. Based on empirical data sources produced mainly by human rights organisations, we critically discuss this case study with regard to the settler colonial spatial logic as well as the stigmatisation of the settler colonial indigenous subject. Considering that space is a social product which produces and reproduces power relations and inequality (Lefebvre, 1991), the fact that premature death, diseases and suffering are disproportionally concentrated within poor communities and minorities located in specific locations stresses the necessity to consider space when discussing health.
Urban theorists have been well aware of the impact of space on social relations. A critical body of literature doubts the myth that planning and urban development are rational and objective professional activities that generate social equity. Rather, this literature points to the oppressive power of planning which is used as a tool for social control, and proposes that urban space reflects and often reproduces power relations (Sandercock, 1998; Yiftachel, 1998). Various studies have highlighted the influence of planning over urban governance, deliberative practices (Forester, 1999), the mobilisation of social movements (Castells, 1983), economic and social stratification (Harvey, 1996), and access to urban services such as public housing and employment. Nevertheless, very little has been written specifically about the effects of the organisation of space, especially in the urban context, upon health. Jason Corburn’s work is one of the few that discuss the links between health and planning, by posing questions such as: how can planning return to its health and social justice roots? What are the connections between planning and health equity? What new political processes can help reconnect planning and public health, with a focus on addressing the social determinants of health (Corburn, 2009: 1)?
However, these questions assume the existence of a common liberal social contract and ideological context, overlooking structural-political mechanisms of colonial domination (Roy, 2006; Salamanca, 2016) and view planning and the urban as detached from their origins in the global centres of power (Watson, 2009). Indeed, the links between planning, health and control are inherent to the history of colonial cities. Providing measures to secure and improve public health, particularly among the lower classes of society, has been one of the main missions of urban planning from its initiation (King, 1990; Sandercock, 1998). The perception that unplanned and informal urban spaces equal illness and filth (and hence should be demolished and their inhabitants evicted) are deeply rooted in the practical and bureaucratic logic that guides planning (Njoh, 2009).
With the above in mind, let us mention the work of several scholars who have noted the links between settler colonialism and health. Richmond et al. (2005), for instance, identified a number of processes through which the people of the Namgis First Nation in Canada have experienced decreased access to and control over environmental resources within their traditional territory, which had a detrimental impact on community health and well-being. In research that focused on the indigenous people in Winnipeg, Canada, Snyder and Wilson (2015) demonstrated how mobility is an intergenerational phenomenon, influenced by colonial practices. They concluded that although migrations of indigenous communities can contribute to positive health experiences, in many cases residential mobility, which is largely involuntary and linked to stressors such as neighbourhood safety, results in negative health effects. Hudson-Rodd (1998) shows how controlling the places of First Nations affects the health and healing practices of indigenous people, while Patrick (2011) points to the way in which technocratic approaches to ‘fix’ water quality problems have resulted in only limited success among First Nations in Canada. Smit et al. (2015) examine how economic, social and political forces affect non-communicable diseases (NCDs) in Khayelitsha, a low-income area of Cape Town, South Africa, by shaping the built environment. They show two main pathways through which the built environment impacts NCDs: by forming a complex food environment in which it is difficult to achieve food security, and by creating an environment that is not conducive to safe physical activity and that generates high levels of depression and stress.
While focussing on health, the above scholars implicitly – we suggest – highlight the spatial factors that characterise settler colonial geographies which are the subject of slow violence and echo Nixon’s (2011) notion of ‘unimagined communities’, those who are ‘internal to the space of the nation state… [and] whose ‘vigorously unimagined condition becomes indispensable to maintaining a highly selective discourse of national development’ (p. 151). Accordingly, isolation, segregation, limited mobility, control and exploitation of environmental resources mentioned above, affect indigenous people health and wellbeing.
In this paper we aim to take this insight as a vehicle for developing our argument, and to contribute to this evolving conversation by explicitly interweaving the nexus of settler-colonialism/health in urban territories in general and in the case of the Bedouins in Israel in particular. The significance of our attempt, which is too often neglected from the literature, was recently highlighted by Qato (2020) who claims that settler colonialism is not a social or political determinant of health. Rather, she argues: […] settler colonialism precedes and is fundamental to all other determinants of health—be they clinical, economic, social, or political. Settler colonialism is woven, in ways both known and unknown, into these determinants. In its direct attacks on us and on the environments in which we live and seek care, settler colonialism distorts our relationships with our bodies. (p. 9)
Throughout this paper we refer to the Bedouin localities as part of the production of urban territory. Such a reference is not reflected in the literature, which tends to focus on unrecognised localities as a non-urban phenomenon (Meir and Karplus, 2017). It was Cedric Parizot, a French anthropologist, who suggested ‘another approach to the Negev Bedouins in the Israeli-Palestinian space’, linking their economy, social ties, employment, political activity and personal connections to the wider territory that includes the urban centres, including Beer Sheva (Parizot, 2001). Indeed, our approach to refer to it as part of the urban process stems from growing urban studies literature suggesting that we combine the ‘non-urban’ with the study of the urban itself (Walker and Leitner, 2011). Though it is not within the scope of this paper to discuss in detail this emerging discussion, let us mention Brenner and Schmid (2015) who call for reconceptualising the urban as ‘… an essential epistemological and political pre-condition for understanding the nature of society itself’ (p. 6). They further suggest that there is a necessity to illuminate the urban as a multi-layered process of social, spatial and economic transformation (Brenner and Schmid: 16). In order to understand urbanisation as such, urban theory must widen its spatial scope and pursue an ‘urban theory with an outside’ (Jazeel, 2018; see also Goonewardena, 2012; Roy, 2009).
Extended urbanization involves, first, the operationalization of places, territories and landscapes, often located far beyond the dense population centres, to support the everyday activities and socioeconomic dynamics of urban life. The production of such operational landscapes results from the most basic socio-metabolic imperatives associated with urban growth—the procurement and circulation of food, water, energy and construction materials; the processing and management of waste and pollution; and the mobilization of labour-power in support of these various processes of extraction, production, circulation and management. (Brenner and Schmid, 2015: 18).
We join the above by discussing the Bedouin localities not as spatial configurations but rather as vibrant, relationally developing entities which configure and re-configure the urban territories and communities residing in them (Massey, 2005). They struggle for access to urban services and goods (such as health), and for the power to re-produce them (Harvey, 2012). Our case falls into this category not solely from a spatial perspective but also from economic, cultural and social angles, as well as by virtue of the use of services by the Bedouin community (including health and welfare, for example, on the metropolitan scale). The stigmatisation of the Bedouins as invaders at the frontier of the metropole as well as their forced urbanisation further emphasises the relevance of the urban context to the study of the Bedouin localities.
In the next section of the paper we will focus on settler colonialism in Israel and its specific impact on the Bedouin population. We will then review existing research and data that exposes the crucial effect of spatial organisation on the health of the Bedouin population. In the final part of the paper we contextualise the empirical evidence regarding the health-space nexus in the political context of settler colonialism. We examine the ways health inequalities are spatially produced, and are in turn mobilised to stigmatise indigenous communities as part of the settler colonial spatial project of dispossession and displacement.
Settler colonialism and the Bedouins in Israel
Settler colonial society is based on a project of settling newcomers on contested ‘frontiers’ in order to achieve political control as well as to access key resources (Stasiulis and Yuval-Davis, 1995). It is based on the desire to create a new society through the cultivation of what is considered as terra nullius, a land under no formal ownership, awaiting to be seized and used by the modern, advanced nations of the world, displacing its native communities. 5 Settler societies may be ‘external’ or ‘internal’; the former relates to the organised movement of people across borders, often into other continents, as in the period of European colonialism. The latter refers to the planned ethnicisation of ‘internal frontiers’ in which the state manipulates the local geography to further the interests of a dominant group (Falah, 2003; Plonski, 2018; Yiftachel, 2006). Both processes produce uneven patterns of ethnic, race and class segregation, as exemplified in the case of the Negev/Naqab region in Israel. 6
Several researchers have identified Israel with the settler society model (Shafir, 1989; Shalhoub-Kevorkian, 2016; Yiftachel, 2006). In such societies, some broad ‘ethno-class’ categories tend to form over time: the ‘founders’, the ‘immigrants’, the ‘locals’ and most recently, the ‘foreigners’ (Stasiulis and Yuval-Davis, 1995). These ethno-classes are created by geographical processes of expansion and settlement, and by the associated flows of resources and development which are determined by, and hence reflect, power relations between groups. This creates structural economic and political stratification, in which ethnic origin and class affiliation largely overlap. The founding group gains a dominant status during the critical formative period of the new state. In Israel, this group is mainly composed of Ashkenazi Jews, the ‘founders’ of Zionism and the state. The second group is comprised of various non-Ashkenazi ‘immigrants’, most notably the Mizrahi ethno-class, and recently also Jews from the former Soviet Union and Ethiopian Jews, who have joined the ‘founders’ in their national project of settlement, albeit from an inferior economic and cultural position (Tzfadia and Yacobi, 2011). The third local group are Palestinian-Arabs (including the Bedouin indigenous population) 7 who resided on the land for generations prior to the arrival of most settlers (Falah, 2003). They are largely excluded from the process of constructing the new nation and are trapped within their inferior ethno-class status. The Bedouin population is further weakened in this settler-colonial hierarchy, based on the refusal to recognise their land rights and the ‘unrecognised’ status of their localities, as will be further detailed in this paper.
The Negev/Nagqab is the southern region of Israel, where a large Bedouin population – estimated between 65,000 and 90,000 people – lived before 1948. During the war in 1948, large parts of this population were deported from the area or fled to Jordan, Gaza and the West Bank (Abu-Saad, 2004). Today, the remaining Bedouin population currently numbers around 270,000 who live in three types of localities: (i) governmental planned townships, (ii) recognised villages and (iii) unrecognised villages. There are 46 Bedouin localities of which 35 are unrecognised by the authorities, and the population living in them is estimated at 65,000 people (Rotem, 2017).
Most of the Bedouin localities were established before 1948 as part of the sedentarisation process of nomadic communities under British rule (Falah, 1985; Nasasra et al., 2015). Some villages were also established during the 1950s by Bedouin clans. These were transferred from other parts of the Negev/Naqab into a restricted zone in its north. In the newly created land registration and planning system in Israel, these Bedouin localities were not taken into account (Plonski, 2018; Yiftachel, 2009). The property registration system according to which the Bedouin population operates was not recognised by Israeli law and hence the Bedouin localities ‘…which bear the literal designation of nonrecognition, provide a near-transparent instance of the perilous effects of the state’s refusal to recognise the legal and historically based rights of the Bedouin to their land’ (Bhandar, 2018: 115). Despite being formal citizens, they were defined as invaders who hindered the development and planning of the region (Nasasra, 2017; Nasasra et al., 2015), and as noted by Plonski (2018), several decades of settler colonialism created a situation through which ‘Israeli-Jewish settlers were turned into indigenous land-owners, and indigenous Bedouin-Palestinian communities were turned into infiltrators and trespassers’ (p. 1349).
The Bedouins reacted to land expropriation and to their living conditions by rapid informal construction, which was defined by the authorities as illegal. These unrecognised villages received no basic infrastructure, nor services. The Israeli authorities view the expansion of informal Bedouin localities as a threat to state control over land, and therefore regularly demolish these illegal shelters (Falah, 2003; Fenster, 1993; Kedar et al., 2018; Yiftachel, 2009). Since the mid-1960s, the Israeli government has followed a plan for re-settling the Bedouins in towns in the Negev/Naqab, where housing, infrastructure, education and health services have been partly supplied (Yacobi, 2004). In order to be eligible for subsidised plots of state-land in the new Bedouin towns, families that moved into them had to withdraw any claim on their unregistered land or informal houses.
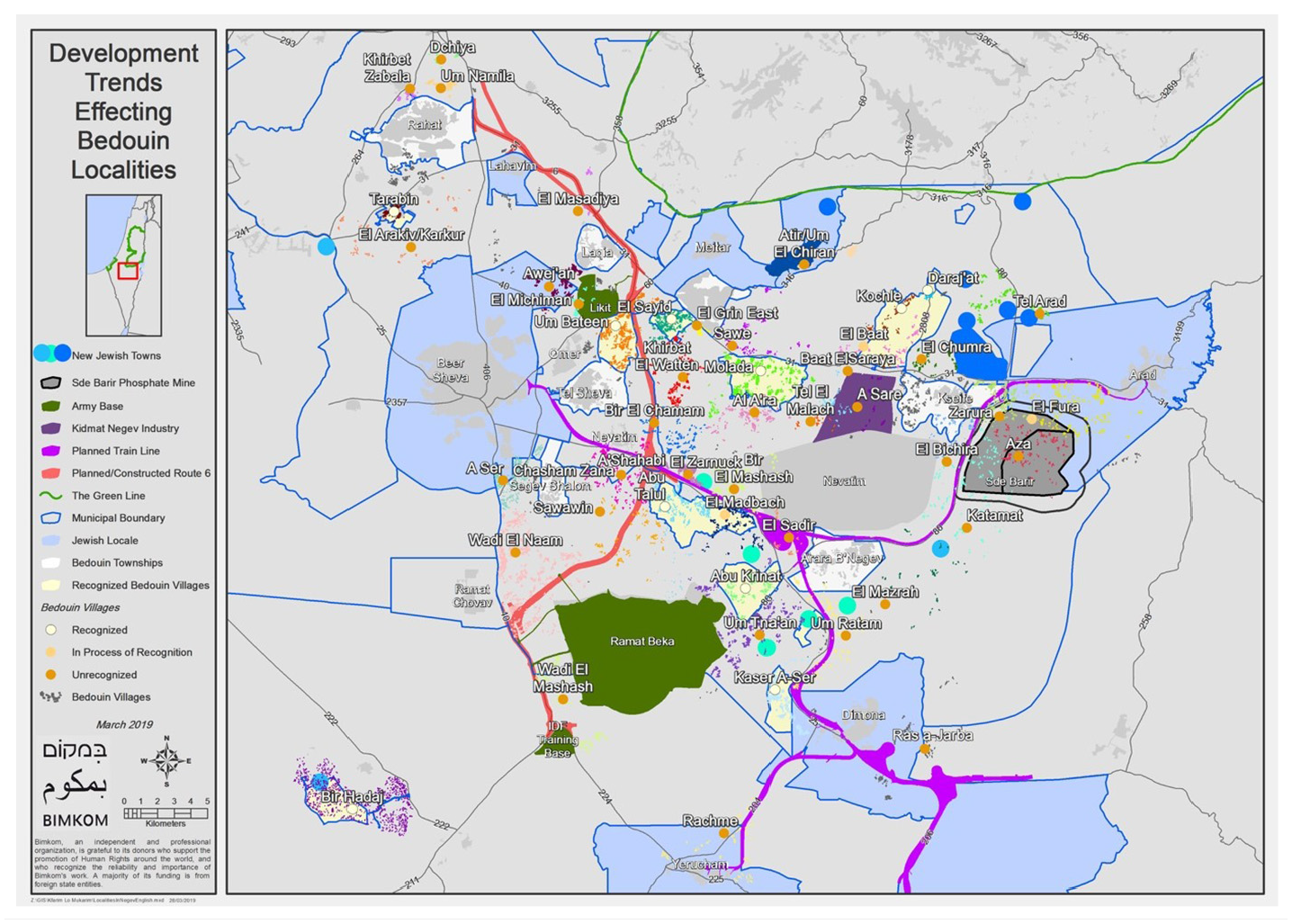
The planned towns partially materialised the state’s aspirations to forcefully urbanise the Bedouin population. Their construction was countered by opposition as they did not fit with the traditional way of life (Fenster, 1996). The infrastructure provided in these townships is inadequate, and their residents suffer poverty and social immobility. A large population therefore remained in the unrecognised villages which also lack infrastructures such as transportation, electricity, running water, schools, welfare and health services (Filc, 2009; Rotem, 2017) (Map 1).

Development trends effecting Bedouin Localities.
In 2008 a public committee headed by retired Supreme Court Judge, Eliezer Goldberg, was set up in order to find possible solutions for the regulation of Bedouin localities. This committee aimed to end six decades of land disputes. The Goldberg Committee’s recommendations included the formation of a legal and planning apparatus that would allow partial recognition of Bedouin land ownership. Planning the Bedouin’s re-settlement, according to the committee, should take into consideration traditional housing and land use (Goldberg Committee Report, 2008). The Committee’s recommendations were partially implemented to solve the land dispute, which was named after its formulators: MK Beni Begin and Ehud Prawer, Head of the Department of Policy Planning in the Prime Minister’s Office. This plan integrated the Bedouin localities into TMM 23/14/4, the master plan for the Be’er-Sheva metropolin.
However, the plan included some discriminatory restrictions on the Bedouins which were not applied to the Jewish settlements in the same area. For example, the Begin/Prawer Layout did not recognise some Bedouin villages, claiming that they were too small to be acknowledged as localities. At the same time, small Jewish settlements were included in the plan and recognised institutionally. The Begin/Prawer Layout and a law for its implementation were submitted for the approval of the Knesset in 2013. Fierce resistance from both sides of the political divide, caused by the discriminating restrictions for the left, and by the partial recognition of the Bedouins’ land claims for the right, led to the termination of the discussion and, in fact, to the shelving of the Layout and the proposed law. 8
Health inequalities and spatial (non-)planning
In this section we present the findings of studies revealing the relationship between land, (non-)planning, infrastructure and the deteriorated health of the Bedouin population. Despite the recognition of some Bedouin villages and the urbanisation which was accompanied by the supply of infrastructure and services, health disparities between the Bedouins and the general Israeli population still exist (Filc, 2009). A telling illustration lies in the difference in life expectancy between the Arab and Jewish populations in Israel. The Central Bureau of Statistic’s report indicate that the life expectancy of Jewish women is 85.1 and 81.8 for Jewish men, while in the Arab population this number is 81.9 for women and 78.1 for men (Koch-Davidovich, 2020: 5). 9 Since in Israeli statistics the Bedouins are included in the general Arab population, no exact numbers can be found regarding this specific population. However, their life expectancy is significantly lower even in relation to other Arab communities (Alpasi-Henly, 2016). The statistics regarding the different regions in Israel support this claim, with the southern region of Israel (including the Negev/Naqab) having the lowest life expectancy in Israel) (Ibid: Ibid).
We will explore the space-health nexus that emerges from these studies, highlighting the role of infrastructure, environmental (in)justice and health care provision and their effect on everyday life and health. Our main argument here is that the right to land – and hence recognition and the provision of urban infrastructure – is the condition for the right to health, and that inaccessibility to water, electricity, or proximity to environmental hazards, are not neutral facts but rather the results of policy and planning (Yacobi, 2019).
Infrastructure
As widely discussed, infrastructure connects people and goods and is also a focal element through which we can understand the formation of the political (Annand, 2018). However, infrastructure also has a violent side (Rodgers and O’Neill, 2012), restricting access to essential resources and services to the marginalised. The latter, in our case, is based on the state’s ‘Dead Negev Doctrine’, that is, the use of Western and colonial land claims by the state to dispossess the Bedouins (Kedar et al., 2018) and justifies the state’s withdrawal from any responsibility of providing services. A telling illustration is reflected in the inaccessibility of clean water and electricity that has a critical influence on the Bedouin population’s health. According to a UN Resolution from 2010, ‘equitable access to safe and clean drinking water and sanitation’ are ‘an integral component of the realisation of all human rights’. The UN therefore ‘recognises the right to safe and clean drinking water and sanitation as a human right that is essential for the full enjoyment of life and all human rights’ (United Nations, 2010).
Water infrastructure is not provided to the unrecognised villages, which consequently suffer severe water shortages for drinking, cooking and hygiene purposes. A special committee of the Israeli Water Authority is responsible for approving such connections due to ‘humanitarian considerations’. Between 1997 and 2010 only 106 out of 675 submitted requests were approved (Bas Spektor, 2011). The committee usually argues that these connections weaken water pressure in the pipeline, or that such connections will make it more difficult to evict inhabitants from the unrecognised villages. Importantly, as of 2015, nine villages were still not connected to any water system (Rotem, 2015: 5).
Water supply is also provided by ‘water centres’, as the one presented in Figures 1 and 2, that consist of central pipes to which families can connect a water metre and a secondary pipe. Water centres operate in the recognised villages of the Abu Basma Regional Council. 10

Water centre in the recognised village Um Batin.

Water supply from the water centre to housing compound in Um Batin.
In 2010, a request was submitted to the Parliamentary Finance Committee to order the establishment of ten more such water centres in the Abu Basma localities, stating that water centres will constitute ‘an efficient temporary solution for more than 90% of the unrecognised villages’ residents’ (Physicians for Human Rights, 2010). A common way of transporting water is via plastic or metal tanks, filled outside the village and delivered to houses by trucks. Other than the problems caused by the high price of water and its transportation, these tanks are kept outside, exposed to the sun, and tend to develop mould, rust, algae and other infections that cause gastrointestinal diseases.
As mentioned at the opening, electricity is not provided to Bedouin localities (both recognised and unrecognised). Some residents use generators, which operate between 1 and 4 hours a day, or solar systems that provide low outputs. Both alternatives are expensive and are therefore rare. Lack of electricity is particularly detrimental to the health of chronic patients, who receive regular medications but are unable to store them in proper conditions. A survey (Abas and Alon, 2008) found that 21% of the Bedouin population had chronic diseases, out of which 58% were children. The most common diseases were respiratory, diabetes, heart diseases and mental disorders. Electricity is essential for the treatment of respiratory diseases: electric oxygen generators are cheap and efficient replacements for expensive oxygen tanks. BIPAP machines, which regulate air pressure in patients’ lungs, do not have a non-electric alternative and their absence causes frequent hospitalisations, deterioration in health and death.
State unrecognition of land ownership means a lack of services such as the collection of waste and sewage disposal facilities, such as presented in Figure 3, which pose severe risks to the Bedouin’s health.

Sewage water flows next to housing in Um Batin.
Improvised septic pits used in unrecognised villages attract pests, constitute a smell hazard and cause the seepage of sewage into water sources. The estimated amount of waste produced in the Bedouin localities (as opposed to the assumptions of the Strategic National Plan) is an average of 0.73kg per person per day: less than half the average in Israel. In spite of this relatively small amount of waste, improvised solutions for its disposal, such as burning, cause both air pollution and intense smell hazards. House demolitions also constitute an environmental risk linked to waste disposal, since the debris is never cleared from such sites (Abu-Ras, 2011).
Environmental (in)justice
Analyses of the influence of environmental conditions on the Bedouins’ lives reveal the devastating effects of environmental injustice on the community’s health and life. The lack of recognition of the villages plays a major role in their increased exposure to environmental hazards and their effect on health.
A factor in the Bedouin population’s degraded health is living in desert conditions with no infrastructure, thus exposing the people to extreme temperatures, sandstorms and poisonous animals. These conditions are worsened in many localities by their proximity to industrial plants and chemical waste disposal areas, to quarries and phosphate mining areas and to army training zones.
Lack of recognition ‘means the failure to consider the location of these populations in the planning process of industrial and military infrastructures’ (Bas Spektor, 2011: 16). The industrial plant (IP) Ramat Hovav, for example, includes about 20 chemical industry facilities. The minimal safety radius around such a plant should be 5km, while the unrecognised village of Wadi al-Na’am is located only 1km away. According to epidemiological researches, Bedouin populations residing up to 20km away from the IP suffer from increased mortality rates due to symptoms/ill-defined conditions and non-external causes (Karakis et al., 2008; Sarov et al., 2008) (Figure 4).

Wadi al-Na’am housing in proximity to a high voltage line.
A study by The Ministry of Health (2011) indicates that living up to 20km from Ramat Hovav is related to significantly higher rates of Bedouin infants suffering from congenital malformations and severe defects in their nervous, heart and skeletal systems. These may cause mental retardation, disability, miscarriage and the death of the infants. Neighbours of Ramat Hovav also suffer from significantly higher rates of respiratory diseases such as asthma and pneumonia. These findings include both adults and children, and are characteristic of Bedouin communities as well as Jewish Kibbutzim in the region. Another hazard that is expected to pose severe potential health risks to the residents of Bedouin localities is the planned phosphates mining site in Sde-Barir, to which several objections were submitted. Professional reviews demonstrate that the mining of phosphates at such proximity to villages will expose the population to respirable particles containing radioactive materials, causing respiratory illnesses and lung cancer (Spektor Ben-Ari, 2013). The plan for Sde-Barir will clearly have detrimental effects on the health of the adjacent Bedouin communities such as Al-Furaa’, where the school is located only 1.5km away.
Our discussion above echoes Nixon’s notion of ‘unimagined communities’ presented at the opening of this paper and exemplifies how the toxic and polluted environment, which is actually an outcome of the state’s policy, not only risks the health of the Bedouins, but also excludes them from resources such as land that previously offered them livelihood and health.
Health services
Non-recognition also has a major effect on the accessibility of health services. In accordance with the Israeli National Health Insurance Law, most of the Bedouin population is insured in one of the Health Funds operating in Israel (Filc, 2009). The first clinic was established in 1994 in the unrecognised village of Al-Grien. Most other clinics were established following petitions to the Supreme Court by a coalition of human rights NGOs. By 2011 there were 12 clinics in such villages. According to some reports (Abas, 2009, Davidovich, 2020), the clinics operate in temporary structures such as caravans. Though they are connected to water infrastructure and have adequate sanitation, electricity is not regularly supplied, and it is impossible to keep equipment and medication that requires cooling (Koch-Davidovich, 2020) (Figure 5).
Health clinic linked to generator the doctor-population ratio in Israel is one.
The doctor-population ratio in Israel is one doctor to every 1200–1400 people, whereas in the Bedouin localities this ratio is one doctor to every 3116.7 people. According to the 2009 survey, clinics operate 13 weekly hours to every 1000 people, while clinics in neighbouring Jewish localities operate 21 weekly hours. The doctors working in the clinics in the Bedouin villages are general practitioners; there are no specialists such as gynaecologists or paediatricians. Research conducted in 2008 found that ‘Bedouin children arrive to the emergency room in critical stages of the disease, due to late diagnosis resulting from the lack of medical services’ (Abu-Sharab, 2008: 8). Furthermore, the lack of pharmacies in the localities limits the medicine inventory available.
The lack of convenient transport infrastructure further affects accessibility to health services. For example, residents of Tal al-Malah, where there is no clinic, use the clinic in Kseifa, located 15–18km from their houses. The average arrival time using public transport is 2.5 hours in each direction. Transportation problems also affect the arrival of the staff to the clinics, causing ‘late arrivals and early departures of some of the staff, thus shortening the clinic’s official reception hours’ (Abas, 2009: 15).
The health crisis in the Bedouin population most prominently affects two vulnerable groups: children and women. For example, mother-child health stations providing antenatal care are essential in a community with high birth rates such as the Bedouin community. However, only after a petition was filed to the Supreme Court (High Court Appeal 7115/97), six stations were established in the villages in 2001. In 2015, there were still only six active stations in the localities. A portable station, which had travelled between the villages, had stopped operating (Rotem, 2015: 11) and the active stations had similar problems to the other clinics. The lack of specific health services for women such as gynaecologists and antenatal care in their communities (given that, as mentioned by Gottlieb et al.(2011), women are dependent on male chaperoning to go outside of their communities), has indeed a critical effects on women’s health.
The physicians of space: Promoting stigmatisation and dispossession
In an attempt to regulate the Bedouin localities, seven townships were built by the state during the 1970s and 1980s: Tal Sheva (Tal al-Saba’, established in 1968), Rahat (1972), Segev Shalom (Shqeib al-Salam, 1979), Kseife (1982), Ar’ara BaNegev (‘Ara’ra al-Naqab, 1982), Lakiya (1985) and Hura (1989). The state’s formal narrative for moving the Bedouins to these townships was access to services and infrastructure, which the unrecognised localities lacked. In critically examining the findings reviewed in the previous section, we conclude that the lack of infrastructure, the intensive exposure to environmental hazards and the lack of accessibility to health services are therefore not the result of negligence or a ‘blind spot’ in the planning of the region. They are inherent to the mobilisation of spatial planning to the settler colonial production of space and the effort to dispossess the Bedouins and push them into the designated, limited area of the new townships.
The systematic violation of the Bedouins’ right to health, we conclude, has to be understood not solely as public health concerns. They should be contextualised within the settler colonial planning and urban framework, which is the very ideological and legal basis for the production of informal urban territories. In their analysis of inequalities in non-communicable diseases between population groups in Israel, Muhsen et al. (2017) conclude that despite universal health coverage and improvements in the overall health of the Israeli population, substantial inequalities persist. This fact, they suggest, might be explained by gaps in the social determinants of health (SDoH)-namely people’s ‘access to health care, schools, and education, their conditions of work and leisure, their homes, communities, towns, or cities’ (CSDH, 2008: 1). The SDoH are defined by the World Health Organization (WHO) as ‘the causes of causes’ of health inequality. Reducing health inequalities by improving SDoH is possible, according to the WHO, by tackling ‘Inequitable distribution of power, money, and resources’ (CSDH, 2008: 2). To this end, it is necessary to have ‘a strong public sector that is committed, capable, and adequately financed. […] legitimacy, space, and support for civil society, for an accountable private sector, and for people across society to agree public interests and reinvest in the value of collective action’ (CSDH, 2008).
SDoH as an explanatory framework for health inequalities and the active approach for their amelioration are therefore defined and understood in the context of liberal socio-political conditions. Applying this approach in analysing health disparities in Israel, specifically in regards to the Bedouin population, fail to consider the very political context in which they are produced. Settler colonialism is about the erasure and replacement of indigenous communities based on the devaluation of their claimed rights to the land (Milner, 2020). Providing solutions for the Bedouin health crisis in the spirit of the WHO’s understanding of SDoH stands, hence, in stark contradiction to the political logic of this project.
Rather than SDoH as the ‘causes of causes’ of health inequalities in the Negev/Naqab, we therefore conclude that the settler colonial logic and ideology is the main cause. Access to water, electricity and services, or proximity to environmental hazards, are not neutral facts but rather the results of intentional policy. As illustrated throughout this article, since health determinants are spatial, the colonial project of appropriating, controlling and ordering space is crucial to understanding the institutional foundations that produce health disparities: In contrast to the abundant research mapping prevalence of health outcomes and deploying ostensibly definable and quantifiable explanatory variables, there has been little substantive exploration, if any, of what it would mean to incorporate settler colonialism into our models of health. We must stimulate new ways of integrating understandings of settler colonialism’s logics and mechanisms into our public health research and, perhaps to some degree, data. (Qato, 2020: 10).
Furthermore, planners, policymakers and similar ‘physicians of space’ (Lefebvre, 1996: 99) play a major role in defining these policies, and therefore in the settler colonial project as the ‘cause of causes’ of health inequalities. Under the guise of professional, benevolent neutrality, planners use their authority and expertise to promote the goals of the settlers (Njoh, 2009: 4), clearly exposing the oppressive side of planning.
The systematic production of health inequalities, we further suggest, shape the stigma of Bedouins as invaders and criminals who threaten not only urban residents but also the well-being of the environments in which they live. Israel’s Strategic National Plan frames the Bedouin population as an ‘environmental hazard’, devoting a distinct section to the negative effect of the Bedouins on the environment that results not solely from ‘over-usage’ of resources and the increased production of waste (Abu-Ras, 2011) but also as an outcome of natural growth (The National Development Strategic Plan for the Negev, 2005: 9–10). The health inequality created in the Bedouin community, we suggest, is part and parcel of the work of settler colonialism, aspiring to dispossess the Bedouins and to forcefully relocate them into townships, where conditions are not necessarily better. Producing health inequalities facilitates the stigmatisation of the Bedouins as backward and unhealthy, a community that should be contained in designated areas where it can be forced into modernisation and urbanisation. This stigma is then mobilised for justifying the dispossession of the Bedouins through forced urbanisation and an attempt to transfer them into the planned townships.
Going back to the case of Ennas Al-Atrash, the suggested solution for the family was indeed moving to the planned town, which involved the withdrawal of their claim to their land in the unrecognised village. The family’s refusal of this solution allows for further justifications of the policy of forced urbanisation, backed by a stigmatising rhetoric of backwardness and child neglect. The stigmatisation of the Bedouins as unclean and unhealthy is interwoven into the image of them as the racialised invader and criminal, that was historically constructed already with the establishment of Israeli state in 1948. Unauthorised housing construction results from the very basic need to supply shelter and protect land rights. Yet this phenomenon significantly contributes to the criminalisation of the Bedouins. It is an image that has been transformed into a ‘social problem’ and attached to the discourse of ‘illegality’ that ‘endangers’ the Be’er-Sheva metropolin. 11
The above is also expressed in the words of Israeli Prime Minister Benjamin Netanyahu, who commented in a government meeting about the ‘demographic threat’ of losing the Jewish majority in the Negev/Naqab region. His argument, which followed the demolition of houses in one of the Bedouin’s unrecognised villages, exposes the logic behind the production of a settler colonial space, saying that ‘…different elements will demand national rights within Israel, for example, in the Negev, if we allow for a region without a Jewish majority’. 12 Violence, destruction and erasure of landscapes and communities contributes to state narratives of contamination which are not detached from biopolitics over the colonised subjects, and this, in turn, affects health (Baldwin and Rawstrone, 2019). Stigma, as we have shown, functions indeed ‘as a means of formal social control’ (Goffman in Tyler and Slater, 2018: 729).
In conclusion, spatial changes initiated by the state and resulting from planning (such as those created in the planned townships), or from legal processes (such as the recognition of informal villages) are not sufficient to reach health equity. A profound political and institutional change is requested in order to improve the health of disadvantaged urban dwellers and to ‘… move urban politics towards planning more healthy and equitable cities’ (Corburn, 2009: 2). Rather than assuming liberal political conditions in which formal spaces are serviced and informal spaces are not part of the spatio-political system, we follow Roy (2009) who suggested that informal settlements cannot be viewed as external to the planning system and thus to health disparities. Within the settler colonial context, housing and infrastructure are marked by deep patterns of inequality and exclusion that minimise the control of minority members over resources and territory. This situation, in turn, dictates health disparities. Dealing with health should therefore go beyond physical, psychological and social determinants; rather, the political project of exclusion should be understood as the ‘cause of causes’.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.