
Abstract
This article focuses on the struggles of people with Long COVID to obtain diagnoses and treatment in the face of medical dismissal and ignorance. Drawing on interviews with people with Long COVID who have engaged in self-tracking activities, it illustrates how these practices proved a valuable, if not completely successful, way to challenge medical dominance and epistemic privilege in relation to this contested illness. Furthermore, study findings demonstrate the important yet understudied role of online Long COVID patient communities in supporting self-tracking. The capacity for sharing patient-generated information through these communities offers a way for collective knowledge and interpretive resources to be amassed that can support communities of practice and mitigate hermeneutical injustice. The article contributes to scholarship on the role of digital apps, devices and communities in the generation and distribution of lay knowledge relating to Long COVID, as well as to the sociology of diagnosis and contested illnesses.
Keywords
Introduction
Long COVID (also referred to as ‘post-acute sequelae of COVID-19’) is a newly recognised multisystemic condition following infection with SARS-CoV-2 (Peluso and Deeks, 2024). It is likely driven by several, potentially overlapping, biological factors (Davis et al., 2023). There is now a large body of research on Long COVID, which has documented hundreds of biomedical findings and proposed multiple mechanistic pathways including viral persistence, immune dysregulation, mitochondrial dysfunction, complement dysregulation, endothelial inflammation and microbiome dysbiosis (Al-Aly et al., 2024; Altmann et al., 2023). Evidence for Long COVID treatments is still limited, with a slow rollout of clinical trials, but is starting to emerge (Peluso and Deeks, 2024). Treatments have been identified that can help manage some symptoms associated with the condition and, to some extent, improve quality of life (e.g. Taub et al., 2021). Despite this growing body of research, a number of studies have demonstrated that people with Long COVID still report discrimination, dismissal, ignorance of the science, lack of validation and stigma when they seek medical care (Bergmans et al., 2024; Clutterbuck et al., 2024; Mullard et al., 2024).
In this article we draw on a set of 30 semi-structured interviews conducted with people living with Long COVID who engage in self-tracking to monitor their symptoms and health states. Our research is sited within the literature on the tensions between medical dominance, medical uncertainty, contested illnesses, patient empowerment, lay expertise, patient activism and the operation of epistemic injustice in medical domains. We engage with this longstanding scholarship to explore how, in the context of a highly politicised disease and a novel and contested chronic health condition, practices of self-tracking Long COVID and generating and sharing personal health data in online patient communities intertwine with these tensions. We begin with an overview of relevant literature, and then introduce our ‘Tracking Long COVID’ study and provide findings. Our findings demonstrate how our participants used patient-created knowledge from digital media and devices to challenge medical dominance and epistemic injustice. We show how self-tracking – supported by guidance from online patient groups – can contribute to greater epistemic justice for people with Long COVID but in a way that is still limited by the imbalance of power between patients and medical practitioners.
Background: Contested Illnesses and Epistemic Injustice
Since the 1970s, an extensive body of literature has been published on power relations in the medical encounter in the context of contested illnesses: that is, those health conditions where aetiology is difficult to identify, complex, understudied or poorly understood, and which are therefore subject to differing claims concerning their legitimacy as illnesses (Dumit, 2006; Moss and Teghtsoonian, 2008). From this perspective, health states are sites of struggle between those with power and status and those without (Cockerham and Scambler, 2021; Lupton, 2012). In the contemporary era, contested illnesses are debated in an environment in which ‘empowered’ patients are expected to take more control in the medical encounter but yet are continually faced with medical authority in relation to diagnosis and treatment, which is very difficult for lay people to challenge (Dumit, 2006; Moss and Teghtsoonian, 2008).
People living with rare, invisible, under-researched or novel health conditions have historically struggled to gain recognition from medical practitioners across health systems. Experiencing long-term illness symptoms or chronic illness can cause disruptions to everyday life and identity. These conditions and associated social changes are major challenges to people’s mental health and well-being (Aughterson et al., 2022). The sociology of diagnosis has shown that diagnosis, as a gate-keeping practice that is highly regulated by members of the medical profession, can be a particularly contested phenomenon (Jeske et al., 2024; Jutel, 2014). People with unrecognised conditions often long for a diagnosis so that they can give a label to their suffering that can legitimise it in the eyes of others, and potentially find a pathway for treatments (Dumit, 2006). When this diagnosis is not forthcoming from the medical professionals from whom they seek help, feelings of frustration, grief and hopelessness are frequently the outcomes. This situation creates ‘fragile disease identities’ – those that are continually open to contestation and doubt from others (Roth and Gadebusch-Bondio, 2022).
These struggles have been described as an example of ‘epistemic injustice’ (Blease et al., 2017; de Boer, 2021): a concept that refers to inequalities in the generation of and access to knowledge. As outlined by philosopher Miranda Fricker (2007) in her foundational book Epistemic Injustice: Power and the Ethics of Knowing, epistemic injustice is a distinctive mode of the operation of power and the entrenchment of injustice, involving ‘a wrong done to someone specifically in their capacity as a knower’ (Fricker, 2007: 2). Knowledge is epistemic privilege, which can be founded on expert training and education or on lived experience. There is often asymmetry in epistemic privilege, with expert knowledge frequently having greater authority than lived experience. Fricker specifies two forms of epistemic injustice. The first is testimonial injustice, occurring when prejudice against a speaker results in their words being discredited and losing authority. The second form is hermeneutical injustice, caused by a gap in collective interpretive resources, with the consequence that some individuals or social groups are placed at an unfair disadvantage when attempting to understand their experiences.
In the domain of medicine and healthcare, epistemic injustice is evident in the ways that only those with medical authority have the power to legitimise people’s suffering, discounting or even rejecting the lay expertise that has accumulated. From this perspective, both the medical profession and patients have a right to epistemic privilege and authority, but due to the high status and professional accreditation of medical practitioners, the knowledge that lay people and patients derive from their and others’ lived experiences is treated as irrelevant or inferior. Particularly if the medical condition is rare or novel, or its pathophysiology has not yet been established, people often find themselves battling for recognition of their suffering from medical practitioners in the context of asymmetry of power between the medical profession and patients (Blease et al., 2017; Carel and Kidd, 2017; de Boer, 2021). Conditions such as chronic pain and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) are prominent examples of contested illnesses involving significant struggles over a long period of time for patients to be taken seriously and receive diagnoses and validation of their suffering (Blease et al., 2017; Dumit, 2006).
In recent times, digital devices and platforms have provided unprecedented opportunities for patients to gather and share information about contested, new or rare conditions (Lupton, 2016b, 2017; Marent and Henwood, 2021). Indeed, in the case of Long COVID – a condition that is not rare, but novel and under-researched (despite a growing body of biomedical studies) – digital communities have made a crucial contribution to the generation and distribution of lay knowledge. From the early days of the COVID pandemic, it was patient communities who came together on social media and other digital platforms to identify the condition and share information: often in the face of medical ignorance and initial outright discounting of their illness. Online patient communities have also provided significant validation and social support for people with Long COVID (Mullard et al., 2023; Roth and Gadebusch-Bondio, 2022; Russell et al., 2022). These activities have contributed to epistemic authority on the part of Long COVID patients. Despite these successes, multiple studies have demonstrated that people with Long COVID continue to encounter barriers in obtaining a diagnosis and medical support, and still experience dismissal, stigma and discrimination. They are therefore still struggling for epistemic justice, with women, people of colour and other marginalised groups particularly affected (Bergmans et al., 2024; Clutterbuck et al., 2024; Mullard et al., 2024).
In this article, we contribute to scholarship on the struggles of people with Long COVID to obtain medical support and the role of digital communities in the generation and distribution of lay knowledge through a focus on our participants’ use of self-tracking technologies and practices as a strategy to gain epistemic authority. There is an emerging body of research that has examined how self-tracking technologies are being used – or could be used – for the self-management of chronic illness (Ancker et al., 2015; Davies et al., 2019; Lomborg et al., 2020; Lupton, 2016b; Riggare et al., 2019). Most of this research has focused on self-tracking in the context of illnesses with well-established diagnostic and treatment pathways, such as Parkinson’s disease and diabetes. While some of these studies have suggested that self-tracking can enable patients to better understand the particular ways in which their illness manifests, take more effective decisions regarding selfcare and communicate more accurately with medical practitioners, they have also cautioned that not all patients may be equipped to effectively utilise such technologies (Ancker et al., 2015; Riggare et al., 2019; Lomborg et al., 2020).
Much less explored has been how patients with contested or novel illnesses may engage with self-tracking. Some initial studies, which have investigated the use of self-tracking by people with Long COVID, have highlighted its value for pacing and the validation and encouragement people may derive from their self-tracking data, apart from illustrating how self-tracking Long COVID can be challenging and frustrating work (Homewood, 2023; Homewood et al., 2024; Jayadeva and Lupton, 2025). We build on and extend this previous research by adopting a health sociology lens and focusing on the broader relations of power and tensions over epistemic authority involved when people with Long COVID engage in self-tracking as part of efforts to achieve validation, acknowledgement, diagnosis and support from the medical profession. Furthermore, our findings demonstrate the important yet understudied role of online patient communities in enabling and supporting our participants’ productive engagement with self-tracking practices.
Methods
The ‘Tracking Long COVID’ study received ethical approval from the Department of Sociology at the University of Cambridge. Thirty study participants were recruited through three online Long COVID support groups. The project’s Call for Participants, inviting people who were using self-monitoring practices in relation to their Long COVID symptoms to participate in an online interview, was posted in each of these groups with permission from the group administrators. All those who expressed interest in participating were interviewed.
Interviews were conducted in 2023 by Author 1. To reduce the physical and cognitive exertion of participating in interviews, which could exacerbate participants’ symptoms, and to support the inclusion of people with more severe symptoms (who are often excluded from research) in the study, all interviews were conducted online. Furthermore, participants were offered several options for participating in interviews: on MS Teams, with cameras on or off; in one session or across two to three sessions spread over several days; or fully or partially asynchronously, via text messages or email. The semi-structured interviews began with asking participants about their experiences of Long COVID and seeking diagnoses and treatment. Questions then moved on to exploring participants’ use of self-tracking in relation to their illness, and their engagements with Long COVID groups on social media. All participants were given pseudonyms to protect their identity.
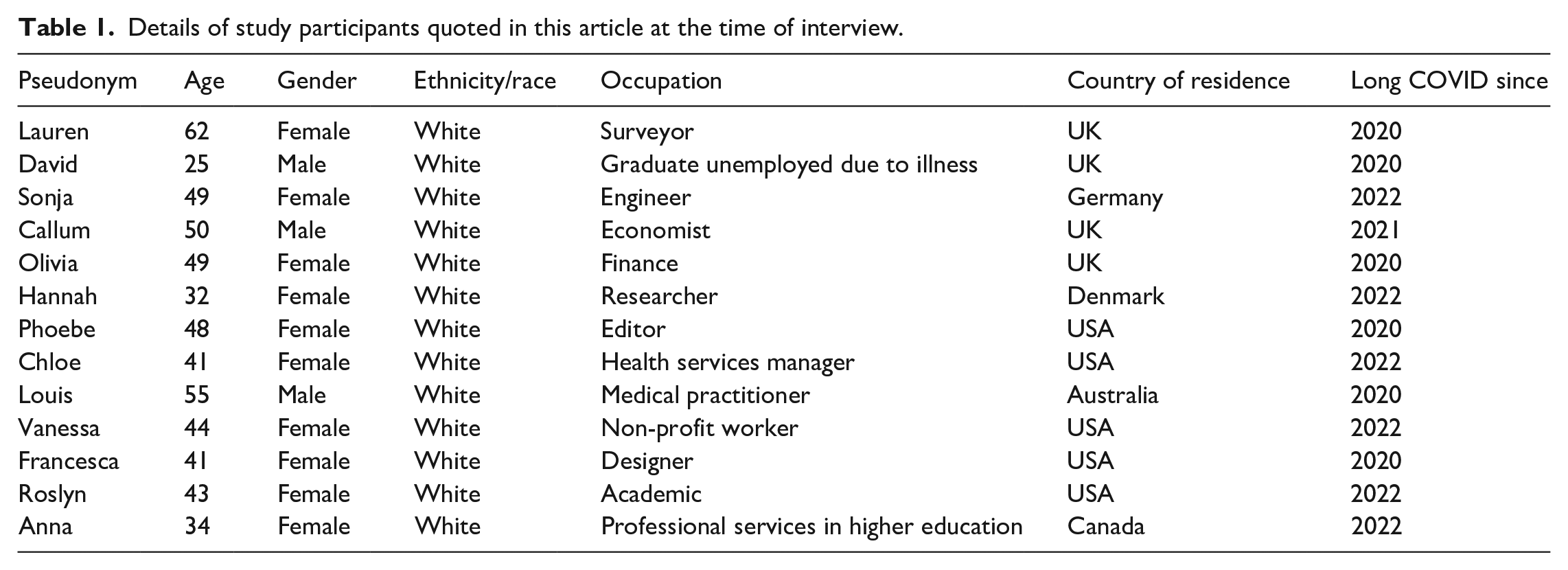
Table 1 provides socio-demographic details of the participants cited in this article. As a group, the 30 interviewees mirrored the typical predominantly White socio-economically privileged individual who engages in digitised self-tracking practices (Findeis et al., 2023), with the exception of their gender. Five participants identified as male, 24 as female and one as non-binary, reflecting epidemiological findings showing that more women than men report experiencing Long COVID (Robertson et al., 2023). This group was also somewhat older than the usual self-tracker (Findeis et al., 2023), reflecting the distribution of Long COVID across age groups, with both young and middle-aged adults affected (Robertson et al., 2023). The mean age of the study participants was 46. The youngest participant was 25 years old, while the oldest was aged 62. Two participants were of South Asian origin and the remaining participants identified as White. They were all highly educated and employed in professional occupations (although more than half were unable to work at the time of the interview because of their illness). All resided in wealthy countries; the majority in the USA (14) or UK (10), with smaller numbers in Australia (2), Germany (2), Denmark (1) and Canada (1). While 21 participants described themselves as living in large or relatively big cities, eight lived in small cities and towns, and one person lived in a rural area.
Details of study participants quoted in this article at the time of interview.
Interviews were recorded with permission and transcribed in full. An iterative thematic analysis of the interview transcripts was then conducted with the help of qualitative data analysis software, ATLAS.ti 23. Drawing on an inductive reflexive analysis approach (Braun and Clarke, 2023), we used open coding to identify themes in the interviews. As the analysis proceeded, the themes were refined and developed. The memo function of ATLAS.ti was used to connect themes and archive illustrative quotations. This process was augmented with both authors reading through the transcripts, independently developing themes based on individual readings and bringing their interpretations together as the analysis progressed. We identified epistemic injustice and epistemic authority as overarching topics in the data, which connected several key themes: participants’ experiences of seeking medical treatment (including having their accounts of their illness disbelieved, minimised or psychologised by medical practitioners, and encountering medical practitioners poorly informed about Long COVID); their experience of trying to make sense of their symptoms (through self-tracking and online patient groups); and their reasons for, experience of and outcomes from drawing on self-tracking data and patient-generated knowledge in engaging with the medical system.
We view the lived experiences as well as previous training of the researchers as central to the study design and interpretation and offering important insights rather than as ‘bias’ (Braun and Clarke, 2023). In this reflexive spirit, we disclose that Author 1 has lived experience of Long COVID. Author 1’s familiarity with Long COVID helped inform how the interviews were conducted, with special care taken to ensure accessibility (as described above). The fact that Author 1 has lived experience of Long COVID was stated in the Call for Participants and reiterated at the start of interviews. Many of the participants expressed interest, at various points in the interview, in hearing about specific aspects of Author 1’s illness experience and Author 1 freely shared this information. This helped build rapport and likely contributed to establishing the interview as a safe space in which to share difficult experiences. Indeed, a number of interviewees expressed that being in conversation with another person with Long COVID had been a cathartic experience for them. Author 2 is a sociologist and communication scholar who brought to the project a longstanding research interest and expertise in the politics of chronic illness and disability, experiences of the COVID pandemic, digital health and digitised self-tracking. Author 2 had no lived experience of Long COVID. The involvement of Author 2 in the framing of interview questions and the interpretation of interview data offered an ‘outsider’s perspective’ that complemented Author 1’s ‘insider’s perspective’.
The Struggle for Medical Support and Treatment
Roughly equal numbers of participants had developed Long COVID in 2022 (15 participants) and 2020 (12 participants), while the remaining three had begun experiencing symptoms in 2021. There were major differences between participants in the medical care and support they had been able to access. While 12 of the participants had had a relatively straightforward experience of obtaining a diagnosis of Long COVID (or, particularly in the first wave of the pandemic, ME/CFS or post-viral illness) based on their symptoms, others had struggled, facing gatekeeping from the medical practitioners they consulted. This latter experience was especially common among those who had developed Long COVID in 2020 rather than in later years, by which time the condition had become more recognised as a health problem.
Lauren and her adult son David, both interviewed for the study, recounted their experiences of poor treatment from the medical profession. They had both developed severe acute COVID symptoms in early 2020, at which point COVID tests were not widely available, and their doctor had refused to consider they could have COVID. When they subsequently developed Long COVID, it had once again been a struggle to get doctors to take their symptoms seriously, much less view the symptoms as related to their initial COVID infections. David reflected: ‘It was a nightmare. They were basically gaslighting us, saying that we didn’t have [COVID] in the first place.’ It was only months later, when Lauren tested positive on a private COVID antibody test, that her doctor had agreed that she and David likely had Long COVID. In this instance, patients’ reporting of their suffering was discounted until a medical test provided ‘proof’ that it was warranted.
While participants who developed Long COVID in the later pandemic years of 2021 and 2022 had typically had an easier time achieving a diagnosis, some had still needed to see multiple doctors and advocate for themselves. Importantly, receiving a diagnosis of Long COVID was not necessarily a path to accessing medical care or having their symptoms taken seriously by the medical professionals from whom they sought help. Several participants described how, despite a diagnosis, medical practitioners had been largely dismissive of their accounts of their illness and had psychologised their symptoms. For example, when Sonja initially approached her doctor about her recurring low-grade fevers (one of her more debilitating Long COVID symptoms), the doctor had suggested that they were a psychological manifestation of her fear of work:
So the Long COVID doctor I saw, he knows some things and also he calls himself a specialist. But, on the other hand, he applies gaslighting and uses some weird explanations for some things. With the recurring fevers, he was just like, ‘uh, you are afraid to go back to work’. And I was like, ‘no, [. . .] I really want to go back to work!’
It was only after Sonja presented the doctor with a few months of data from her digital thermometer, showing the proportion of days on which she had developed a fever, that he was willing to investigate further and prescribe treatment.
Participants’ perceptions of their symptoms not being taken seriously by medical practitioners in many cases also related to the lack of appropriate treatment they had received. When Callum had approached his doctor after developing debilitating symptoms following an acute COVID infection, he had received a diagnosis of Long COVID but little by way of treatment or support:
[The doctor] basically said, ‘You need to take some Vitamin D, come back to me in Eight weeks.’ And I was just like, ‘Oh, I can’t do anything. My entire life is like – I literally, I don’t have my life anymore. You want me to sit around and wait for eight weeks?!’
Very few participants had been able to access tests and investigations that might have helped identify problems causing their symptoms and open treatment pathways. For instance, although Postural Orthostatic Tachycardia Syndrome (POTS) is experienced by a large proportion of people with Long COVID (Davis et al., 2023), most participants had needed to advocate to get tested for it. Indeed, many reported that their doctors – even those practising in Long COVID clinics – had been largely unaware or poorly informed about syndromes commonly experienced by Long COVID patients such as POTS. Moreover, several participants had been given medical advice that had worsened their symptoms. Most commonly, they had been advised to exercise to aid their recovery. However, for those who suffered from post-exertional malaise (PEM) – a symptom experienced by a large proportion of people with Long COVID (Al-Aly et al., 2024) – exercising had resulted in deteriorations in health (see Appelman et al., 2024). Because of limited clinical trials and a lack of established guidelines for treating Long COVID, even those participants who had succeeded in finding doctors who were informed about Long COVID had only been able to access a limited range of treatments that helped reduce the severity of some of their symptoms to some extent.
When speaking about their challenging experiences of trying to obtain medical support, some of the female participants observed that women were often treated dismissively in healthcare contexts and described feeling pessimistic about being believed by doctors. A number of participants, however, also reflected, without prompting, on the various positions of privilege they occupied – for example, as White women, as White men, as highly educated people who could understand research papers, as healthcare professionals themselves, as people who felt confident enough to advocate for themselves in medical contexts – questioning how much more challenging the experiences of less advantaged people with Long COVID must be.
Suffering from debilitating symptoms and unable to access adequate medical support, participants had turned to self-tracking technologies and online Long COVID patient communities to learn more about Long COVID and how to navigate their illness.
Finding a Way Forward: Patient Groups and Self-Tracking
Long COVID online patient groups and communities on Facebook, Discord, Slack, Reddit and Twitter were described by participants as being invaluable sources of information and support. As other researchers have found (Callard and Perego, 2021; Homewood et al., 2024; Rushforth et al., 2021), especially for those who had developed Long COVID in the first wave (early 2020), the patient groups and communities provided their first opportunity to meet others who were suffering from the same types of symptoms. Becoming aware of many others with similar symptoms helped participants see their illness as legitimate. During her interview, Olivia paused for a moment before beginning to discuss her experience of joining an online patient group:
I’ll probably start crying because it’s still quite emotional for me. [Patient Group] was the only place [where] people were [. . .] experiencing the same ridiculous symptoms like I get. [. . .] I was like, ‘there’s something desperately wrong here that nobody knows about except for us’. Well, [Patient Group] basically is the thing that saved me emotionally, physically, medically, everything.
In addition, participants explained how these groups and communities had helped inform them about Long COVID and the types of symptoms and syndromes commonly associated with the illness. Learning for the first time about POTS and PEM through the patient groups, for example, had enabled a number of participants to make sense of their symptoms. Furthermore, information acquired through the patient groups was discussed as having provided crucial insight into possible medications, non-pharmaceutical therapies and behavioural modifications that could be used to manage different symptoms and problems. Callum observed: ‘doctors don’t have really any estimation of how long it’s going to be or really what you have to do to get better. So you’ve got to look to other patients.’
For many participants, Long COVID patient groups had also been their introduction to using self-tracking technologies to monitor and understand symptoms and evaluate and experiment with interventions. Strikingly, most of our participants had not used self-tracking technologies prior to developing Long COVID. They had begun self-tracking for the first time in an often-desperate effort to make sense of and find ways to cope with their Long COVID symptoms. Several participants attributed their decision to begin self-tracking entirely to suggestions by other members of their patient group/s. For example, Hannah observed:
I was kind of reading about this idea [of self-tracking] on that Facebook group. I started seeing people say that they were using apps or that they were using smartwatches. And this GP [a member of the group] had had this idea about keeping your heart rate low. [. . .] I thought this idea of tracking and trying to manage my symptoms by keeping my heart rate low was a really attractive idea. So I read people’s posts for a few weeks and then bought this [smart]watch around six weeks ago.
Furthermore, a number of participants discussed how they had chosen the wearable or tracking app they were using based on information they had acquired in patient groups. For example, Phoebe recounted:
And then last fall, I got this, the Garmin [wearable device], because everybody [in Patient Group] had been talking about [Garmin’s] ‘Body Battery’ [feature]. [. . .] I have followed a lot of conversations that I’ve learned from, where other people are discussing [self-tracking]. And, you know, it’s because of those conversations that I bought the Garmin.
Especially for those participants who had been too unwell to look into the different trackers on the market, the recommendations of other Long COVID patients held significant weight. Callum, for instance, noted: ‘The guy who started it [the Facebook group], he’d done his research and he recommends Garmin. I was just too ill to research, so I just followed his guidance.’ Several participants also discussed how, after gaining experience with self-tracking, they had helped other members of their patient groups choose which device or app to use.
Long COVID patient groups had also provided participants with guidance about how to collect, interpret and use their self-gathered data. As most participants used devices and apps that were not specifically designed for monitoring illness, how to monitor Long COVID was not always self-evident. Through these groups, many participants described learning about the meaning of different metrics – such as Heart Rate Variability, Resting Heart Rate, ‘Stress’ scores on wearables like Garmin – and how these could be used to gain insight into their bodies and monitor their health. Many discussed deriving inspiration from the self-tracking practices of others in the group. Chloe, for instance, reflected on how seeing other group members share their self-tracking experiences and even screenshots of their data had given her ‘clues’ about what she could look out for in her own data. One participant, Louis, had even started an extremely popular patient group himself, focused on sharing guidance about using wearables for understanding and managing Long COVID. In his group, Louis had a series of ‘pinned posts’ in which he outlined his approach to self-tracking using the Garmin smartwatch. He also made videos from time to time to share further guidance and ideas. Louis described how he too had learned ‘heaps of things’ from other group members that he had not been aware of, and it was an ethos of collaborative learning and mutual support that characterised the group.
Identifying Symptoms and Testing Interventions
Through a combination of self-tracking and guidance from members of their Long COVID patient group/s, many participants had been able to identify patterns and correlations between their symptoms, activity and exertion levels, diet, medications and key metrics (e.g. heart rate, heart rate variability, oxygen saturation, sleep data), which they felt they would have been unlikely to notice otherwise. In several cases, identifying such patterns, correlations and trends had enabled them to discover thus far undiagnosed problems or syndromes that were responsible for some of their symptoms.
For instance, Hannah had experienced intense discomfort when upright for over a year. Upon joining a Long COVID patient group, she encountered many others who had the same symptoms and described them as being POTS related. Hannah had never heard about POTS prior to this but quickly learned – through a combination of reading other group members’ posts about POTS and looking up information about the condition on medical websites – that it was characterised by an abnormal increase in heart rate (30 beats per minute or more) upon assuming an upright position. She began to pay attention to her heart rate readings on her smartwatch and how they changed when she was upright, which confirmed her growing suspicion that she had POTS. Hannah highlighted the potential of patient groups and self-tracking technologies to reduce diagnostic delays in conditions like POTS:
I was reading some information about POTS, it was like, oh people experience a diagnostic delay of like an average of four or five years. And so that’s one huge benefit of both the watch and the [patient] groups. It’s like that significantly reduces that diagnostic delay because you’re like, ‘ok, everyone in this group seems to have POTS or like some sort of dysautonomia’. So you zero in on that and then you can use the technology to check whether that’s kind of reflecting your own experience.
Similarly, Vanessa noted how, after sharing her symptoms with members of her online Long COVID group, she had been advised by them to use her tracker to monitor changes in her heart rate when she moved from a supine to upright position, as her symptoms could be related to POTS. Vanessa, who had first learned about POTS through the group too, noticed a clear pattern in her data: when she was upright, her heart rate would spike significantly. She observed: ‘[I was] so blown away with all this data. [. . .] I don’t think I would have known what to look for or how to interpret [the data] without these, like, amazing expert voices.’
Apart from supporting participants with understanding their symptoms, Long COVID patient groups and self-tracking technologies also informed participants’ efforts to find ways to cope with these symptoms. To begin with, self-tracking was perceived as a valuable tool to evaluate the impact of various interventions aimed at reducing and managing Long COVID symptoms – from medications to non-pharmaceutical interventions. For example, participants described observing sharp changes in the trendlines of metrics such as heart rate data upon beginning specific treatments. In some cases, these data had corroborated participants’ perceptions that a particular intervention was helping them or making them worse. In other cases, they had helped participants assess and unravel the impact of interventions in a way that would have been very hard to achieve from just subjective experience. As Francesca put it: ‘when there’s so much going on and you’re trying medications, and the symptoms are fluctuating. . . I mean, unless you have superpowers, I think [self-tracking is] the only way to actually see things clearly.’
In addition, the Long COVID patient groups were described by several participants as having been an important source of guidance, information and ideas about interventions that they could try to address and alleviate various symptoms. Many participants had first heard about – or been motivated to try – specific prescription and over-the-counter medication and supplements after reading about the experiences of other members of their patient group who had tried them and, in some cases, seeing screenshots of data from their trackers. Moreover, in a context where many participants had been urged by medical practitioners to exercise and increase activity, the importance of rest and pacing was something that participants discussed having learned primarily through patient groups. Roslyn recounted:
I think even before I had a device to self-track, I had been following the advice from folks from [Patient Group] that, like, you just don’t ever want to push it with Long COVID, because when you push it, you get worse. Just rest [. . .] track your heart rate. Once you can control that, you can start expanding your baseline a little bit. So, I think it completely shaped my plan for how to try and take care of myself. Because obviously, like, my doctor wasn’t taking care of me, you know?
Participants also discussed sharing their own experiences and self-tracking data – or insights from this data – with their patient groups, in response to questions posed by other members, or because they felt this information could be helpful to others.
Medical Advocacy
Participants emphasised that having a better understanding of their symptoms and possible treatment pathways – as a result of self-tracking and guidance from Long COVID patient groups – had informed how they engaged with the medical system, in a context where many felt they needed to take an active role in managing their care. As Chloe remarked: ‘The truth of the matter is most people with Long COVID are their own doctors. Like, we have doctors, but they’re not directing our care. We are.’ Participants discussed how their self-tracking data, and the insights they had derived from it, enabled them to provide doctors with a concrete account of their illness, and equipped and emboldened them to advocate for the types of tests and treatments that they believed would be helpful, and to refuse treatments and interventions that they felt would not benefit them or could harm them (e.g. exercise therapies). As Anna observed:
It’s really empowered me to direct my treatment a lot better because I just have so much evidence and information of what’s impacting me [. . .] Like I do not think I would have had the treatment I have had, if I didn’t have the data that I have from my tracking.
Participants described how their self-tracking data had been very important for translating their subjective experience of illness into ‘objective’ quantified data that they believed was more likely to be taken seriously by medical professionals. Indeed, some noted that it was because of their self-tracking data that they had been able to get referrals to tests or specialists, and subsequently obtain formal diagnoses and access treatment. For example, Chloe explained:
I really had to be like, ‘No, look! Look at what [my heart rate’s] doing, you know, not just when I’m in the doctor’s office’, and convince [my physician] to send in the referral for both a cardiologist and for [the POTS diagnostic test]. Because she wasn’t going to do anything. [. . .] I think having that [data] definitely gave me more like, say, as a patient. Because they can’t deny that. When you show them these charts from Scanwatch, it’s like, no, I didn’t make that up, I’m not exaggerating, it’s not just anxiety.
A few participants also recounted how through presenting their doctors with their self-tracking data, they had been able to more effectively demonstrate the severity of a symptom, which they felt had contributed to getting prescribed specific treatments. Participants with cognitive symptoms, particularly, stressed that difficulties with remembering and articulating their symptoms had on occasion made them doubt their own accounts of their illness, as well as struggle to communicate what they were experiencing to medical practitioners. Having concrete data to refer to before medical appointments was experienced as a crucial aid in navigating the medical system.
However, not all participants felt their doctors would be interested or willing to hear about or look at their self-tracking data. Callum recounted his experience of trying to discuss his heart rate data with his doctors:
I have sometimes explained to them that I do this [self-tracking using a smartwatch], but their eyes glaze over. They’re not really interested in my experience. So I just don’t go into that. [. . .] I think they think, ‘Oh, well, it’s not actually a medical grade device.’
Some participants also worried that sharing self-tracking data with a doctor might inadvertently lead to the doctor feeling as if their expertise was being challenged. Vanessa, for instance, highlighted how she had to be cautious in how she approached discussing self-tracking data with doctors in the same way that people needed to be cautious in trying to bring relevant research papers to the attention of their doctors:
So I’ve brought up some studies a couple of times and I have kind of felt the tension around that. [. . .] I feel like it’s been similar to that. It’s best to say [. . .] ‘Hey, I’m having this experience’ without maybe bringing up the watch.
Nevertheless, even in cases where they had not shared their self-tracking data or had their self-tracking data taken seriously by a doctor, participants believed that as a result of paying close attention to their bodies and documenting their symptoms and key metrics over time, they had become confident in their knowledge of what they were experiencing, which made them more likely to stand up for themselves in medical contexts and less susceptible to medical gaslighting. Vanessa reflected:
I know that I have been consistently feeling X symptom because I have reported it [on the tracking app] that many times. I think that’s given me a lot more confidence when I’ve gone to doctors’ appointments [. . .] Like, if they have been dismissive of some of my symptoms, I’ve known, ‘hey, maybe this isn’t the doctor for me’. Instead of taking that in and being like, ‘oh, maybe I’m not really having this symptom’ or doubting myself.
Discussion and Conclusion
Our study has therefore brought together the literature on self-tracking and online patient communities with that on contested illnesses, fragile disease entities and epistemic injustice in the context of the significant problem of Long COVID. We show how the practices of self-tracking and sharing self-generated data and other information about Long COVID through online patient groups have intersected with the forces of medical dominance and authority. A strong body of literature has established that people with Long COVID have struggled with receiving diagnoses and accessing medical care and support (Baz et al., 2023; Bergmans et al., 2024; Clutterbuck et al., 2024; Mullard et al., 2024). Our study, conducted in 2023, demonstrates that despite a growing body of biomedical research on Long COVID, and despite being relatively privileged in some respects, many of our participants experienced testimonial injustice when their experiences of Long COVID were discounted, disbelieved, underplayed or ignored by their medical practitioners. Participants, in many cases, were also subjected to hermeneutical injustice arising from their medical practitioners’ lack of interpretive resources to identify and support the management of their symptoms.
Our article contributes to research on how patients resist and navigate epistemic injustice in healthcare contexts (Carel and Kidd, 2017) by demonstrating how self-tracking, supported by online patient communities, can offer an important pathway to strengthening epistemic authority and challenging, to some extent, testimonial and hermeneutical injustice. The apparently more ‘objective’ forms of information generated with wearable devices and apps were used by our participants to prove the validity of bodily experiences, when qualitative accounts of symptoms and experiences were treated dismissively. Notably, while in existing scholarship self-tracking has been framed as encouraging patients to develop a more biomedical concept of their illness (Ancker et al., 2015) as part of dominant ideas about patient empowerment, our participants described such data as bearing the potential to help their clinicians accept a more biomedical framing of their condition. In addition, the capacity for sharing patient-generated information and guidance on Long COVID and self-tracking through Long COVID patient communities offered a way for collective knowledge and interpretive resources to be amassed, supporting patients to better understand their illness and more effectively advocate for themselves within healthcare contexts, thereby reducing hermeneutical injustice.
Scholars have warned of the individualism and focus on self-responsibility that dominate discourses of ‘the quantified self’ (Lupton, 2016b). When people with Long COVID have shared knowledge about their own health states with others in online communities, this individualism and self-responsibility is to some extent sidestepped. This is the ‘communal self-tracking’ mode, in which groups of self-trackers consensually share their self-generated personal data with each other as a form of distributed knowledge (Lupton, 2016a). It also represents an example of ‘digital caring practices’, which are networked with and between online platforms (Zakharova and Jarke, 2024) and a communal rather than individualised mode of strengthening epistemic authority. This approach to self-tracking is far less concerned with achieving the ‘optimal self’ that is one of the catch-cries of the quantified self movement (Lupton, 2016b) but rather is a way of achieving validation as a form of soft resistance to medical dominance and epistemic privilege.
Nevertheless, our participants still faced major barriers to legitimacy in the face of the epistemic authority and gatekeeping exercised by the medical practitioners from whom they had sought help. They had the challenging task of negotiating the fine line between both developing their own epistemic authority and attempting to contribute to their doctors’ knowledge base without unduly provoking resistance on the clinicians’ part. They spoke of the ‘empowerment’ they felt when generating and sharing information from self-monitoring practices, but this was still often stifled in the medical encounter. However, even when participants were unable – or felt unable – to successfully challenge their medical practitioners’ epistemic authority, many still described benefiting from self-tracking through becoming more convinced of and confident about their own epistemic authority and directing their care in more subtle and strategic ways.
Beyond the specific case of Long COVID, our article also contributes to the sociology of self-tracking in the context of illness more broadly. While a number of studies have highlighted how self-tracking can enable patients with chronic illnesses to communicate more accurately and actively with their clinicians and more effectively self-manage their illness (Ancker et al., 2015; Riggare et al., 2019), our study is one of the first to demonstrate the role of self-tracking as a tool of validation and medical advocacy in the context of novel, invisible or contested illnesses.
Furthermore, our article responds to calls for empirical research that illuminates how people with health conditions engage with self-tracking data to make these data useful (Lomborg et al., 2020). Scholars have questioned whether the popularity of self-tracking technologies is likely to extend beyond the tech-savvy or quantified-self enthusiasts, and if patients who fall outside these groups will actively engage with such technology (Ancker et al., 2015). In line with broader criticisms of the ‘empowered patient’ (Baru and Mohan, 2018; Gaffney, 2015), it has been argued that not all patients will necessarily be able to make use of commercial self-tracking devices in ways that benefit them. For people who lack the resources and capacities to meaningfully interpret and utilise their self-tracking data, are too ill or disabled, or feel ‘pushed’ to self-monitor their condition rather than do it voluntarily (Lupton, 2016a), these practices can become a burden, introducing new uncertainties and anxieties (Ancker et al., 2015; Lomborg et al., 2020; Lupton, 2017).
For self-tracking devices to be beneficial in a healthcare context, patients require interpretive aid that enables them to make ambiguous data meaningful and useful (Lomborg et al., 2020). While such aid could come from within the care infrastructure, our study illuminates how, in the case of Long COVID, online patient groups have emerged as a key source of support with not just interpreting self-tracking data but also with finding ways to usefully engage with self-tracking technologies, more broadly. The value of online patient communities has been widely acknowledged in the sociology of health and illness (Lupton, 2017; Marent and Henwood, 2021) and there is an emerging body of literature on the support people with Long COVID are able to access through these groups (Day, 2022; Mullard et al., 2023; Russell et al., 2022). However, our study is the first to highlight the role that these groups can play in the uptake and productive utilisation of self-tracking technologies by people with limited to no previous experience or interest in tracking. It is notable that the majority of our participants had not engaged with self-tracking devices prior to developing Long COVID. The guidance from patient groups about both self-tracking and Long COVID played a major role in many participants’ decisions to begin self-tracking as well as how they engaged with and benefited from these technologies and practices.
What remains important is for medical practitioners to be more open to quantified self-tracking data and other forms of patient-generated expertise. Epistemic justice for people with Long COVID and other contested illnesses will never be fully achieved until the medical profession can develop greater epistemic humility and takes steps to redress testimonial and hermeneutical injustice.
Footnotes
Acknowledgements
First, we would like to express our gratitude to all the study participants for taking the time to participate in this research and for sharing their experiences and insights with us. We would also like to thank Hélène Brunerie for support with transcribing the interviews. In addition, we are grateful to Sam for useful discussions about medical literature.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: We acknowledge funding from the University of Cambridge (Career Support funding awarded to Sazana Jayadeva) and the Australian Research Council Centre of Excellence for Automated Decision-Making and Society (CE200100005).
Ethics statement
The ‘Tracking Long COVID’ study received ethical approval from the Department of Sociology at the University of Cambridge.