
Abstract
Religion has received a large amount of scholarly attention for its role in promoting pro-social outcomes for a community. One of the areas in which religion may demonstrate a positive effect is suicide. The role that religion plays in reducing suicide within a community has long roots in sociology. Émile Durkheim suggested that religion would have a pro-social effect in decreasing suicide. Religion should reduce suicide by establishing values and norms that integrate individuals into society and regulate the behavior of the members of a society. However, the presence of many different religions could erode the social integration and regulation effects of religion. This would cause suicide to increase as individuals become confused as to what values and norms are to be followed. The current analysis uses the religious fractionalization index to examine the effect of religious heterogeneity on suicide. The findings demonstrate that increased religious heterogeneity increased suicide for a sample of countries.
Introduction
Religion has received a large amount of scholarly attention for its role in promoting pro-social outcomes for a community (Ellison, 1992; Ellison et al., 1997; Lim and MacGregor, 2012; Regnerus et al., 1998). One of the areas in which religion may demonstrate a positive effect is suicide (Huang, 1996; Stack and Kposowa, 2011). Consideration of the role that religion plays in reducing suicide within a community has long roots in sociology. Émile Durkheim (1951 [1897]) suggested that religion would have a pro-social effect in decreasing suicide.
Durkheim analyzed the effect that Protestant and Catholic beliefs might have on suicide rates. He found that areas that were dominated by the Protestant faith had higher suicide rates than areas that were dominated by the Catholic faith. According to Durkheim, the Church itself was not responsible for reducing the incidence of suicide; rather, it was the values of the Catholic faith, which promoted social integration and regulated behaviors within the community. The Protestant Churches, on the other hand, operated on a more individualistic basis, which did not promote social integration and could not regulate the behavior of the people in the community.
Research on Durkheim’s levels of suicide and Catholic versus Protestant beliefs has produced mixed results (Ellison et al., 1997). However, many studies have examined Durkheim’s constructs of social integration and social regulation and their connection to suicide (Ellison et al., 1997; Kushner and Sterk, 2005; Moore et al., 2014). Others have examined suicide and social capital, which is the level of social integration and regulation in society (Flavin and Radcliff, 2009; Kelly et al., 2009).
Research has demonstrated that religious belief does reduce suicide both cross-nationally (Huang, 1996) and in the United States (Ellison et al., 1997). However, it is not clear how religious diversity affects suicide rates. Durkheim contended that Catholic belief reduced suicide because of the faith’s ability to exert its values of social integration and regulate the behavior of the people in the community. Yet, if the Catholic faith is present in a community but is one religion among many, it might not have the same ability to integrate and regulate. Individuals in the community would have many different beliefs and values and would not be bound to one dominant value and belief system. Therefore, the power of religion to decrease suicide may erode as individuals are not being regulated by a single religion and integrated into one community.
In the current analysis, I examine how religious diversity affects suicide cross-nationally. I first explore Durkheim’s argument of social integration and social regulation in more detail. Next, the analysis examines the literature on suicide and religion. Third, I examine the research on fractionalization to understand the links with religious diversity in other areas. Finally, I examine 41 countries using the religious fractionalization index, which throws light on the question of whether diversity in religion might erode the safeguards against suicide.
Literature review
Émile Durkheim believed that the most important aspect of religion was to be found in its effect on community (Roberts, 1984). According to Durkheim, individuals had created the term God to represent the idea of ‘society’; thus, individuals who worshiped God were actually worshiping society and, in doing so, acknowledging how individuals should behave in society. For example, Roberts (1984) pointed out that people internalize a norm when they understand how a particular behavior affects society. A husband refrains from cheating on his wife because he has internalized how cheating would destabilize the family, and hence destabilize society. Durkheim suggested that religion aids us in understanding the collective identity of society. Religion is the glue that bonds people together in society (Roberts, 1984). Religion helps us to define ourselves as a community with common values and norms. Therefore, religion aids in social integration and social regulation.
Durkheim’s four types of suicide
In 1897 Durkheim wrote Le Suicide, which discussed how social integration and regulation might affect the suicide rate. If, as Durkheim suggested, religion’s main function was to regulate and integrate social behavior, then any disruption in a religion’s ability to do so could produce suicide. Examining different rates of suicide across many different countries, Durkheim suggested that society generated four different types of suicide: egoistic, altruistic, anomic, and fatalistic. The core argument that Durkheim made about the different types of suicide was that they were determined by the level of integration and regulation of the society, which affected the individual.
When individuals do not feel integrated into society, they may commit egoistic suicide (Ritzer and Goodman, 2004). Individuals who are not well integrated into society feel as if they are not part of the community, but the community also feels that the individuals do not fit with their lifestyle. The sense of isolation resulting from not being part of society leaves the individual without the moral guidance needed to operate in the social environment. Without any guidance, the individual might turn to suicide as a way to deal with his or her isolation.
According to Durkheim, excessive integration into society can also lead to suicide. He called this type of suicide altruistic suicide (Ritzer and Goodman, 2004). Durkheim suggested that when the individual is too integrated, the pressure to succeed for the greater good can be overwhelming. Individuals who are expected to succeed but do not may turn to suicide. For instance, a samurai warrior who does not live up to expectations will commit suicide because he was too integrated into society. In other situations, individuals commit suicide because they believe it is good for their society (e.g., suicide bombers).
Moore et al. (2014) provided evidence in support of Durkheim’s egoistic and anomic suicide models. They examined 2,193 counties in the United States and found that counties with low integration and low regulation had increased suicide rates (egoistic and anomic suicide, respectively).
Society also has to regulate the behavior of the individual. Durkheim described anomic suicide as suicide when the regulation of society is disrupted (Ritzer and Goodman, 2004). The disruption can occur during an economic boom or depression. The disruption leaves individuals with little guidance as to the norms and values that apply in the new situation, or those that they should be following. This lack of regulation leaves some individuals feeling overwhelmed and increases suicide in the society.
Ritzer and Goodman (2004) pointed out that fatalistic suicide is discussed by Durkheim only in a footnote. Fatalistic suicide occurs when the regulation of society is excessive. For example, a slave may commit suicide because of his hopeless position. Individuals who feel that they have no control of their lives are more likely to commit suicide.
Religion and suicide
Research on the effect of religion on suicide has demonstrated that suicide is reduced by the presence of religion (Ellison et al., 1997; Huang, 1996); suicidal attitudes are also reduced (Stack and Kposowa, 2008, 2011). Huang (1996) examined cross-national suicide rates for 48 countries. To measure the level of religion in his sample of countries, Huang used the data from the World almanac and book of facts. He created a dummy variable for the level of religiosity for each country, countries that were over 85% Catholic or Muslim being considered ‘religious.’ The findings of the study demonstrate that countries high on his religion scale had lower levels of suicide.
Stack and Kposowa (2008) examined suicide rates and suicidal attitudes in a sample of 31 countries. Using data from the World Values Survey, the scholars created two variables to measure the role religion played in suicide: religious identification and religious attendance. For religious identification, Stack and Kposowa (2008: 48) aggregated the responses to the item ‘independently of whether you go to church or not, would you say you are … (1) a religious person; (2) not a religious person; or (3) a convinced atheist.’ To create the religious attendance variable, Stack and Kposowa (2008: 48) used the question ‘apart from weddings, funerals, and christenings, about how often do you attend religious services these days?’ Using a hierarchal linear model, the study found that individuals who attend church more often were less accepting of suicide and individuals who identified as religious were less supportive of suicide. Moreover, Stack and Kposowa (2008) found that suicide rates were lower in more religious countries. Stack and Kposowa (2011) further examined suicide acceptability (i.e., thoughts and attitudes favorable to suicide) and found that religion reduced suicide acceptability.
While religion has been demonstrated to reduce suicide and suicidal attitudes, the effect that religion can have when there are many different faiths in one country is not as clear. Ellison et al. (1997) examined religious homogeneity and suicide rates in 296 metropolitan areas in the United States. Using 1980 data from the Glenmary Institute, the researchers created a religious homogeneity index for eight denominations: conservative Protestant, moderate Protestant, liberal Protestant, miscellaneous Protestant, Catholic, Orthodox, Jewish, and Mormon. The authors also created an index including 111 religious families to compare the eight index measure to the 111 index measure. This allowed them to examine whether the two indices provided different results when examining suicide. They also controlled for the percentage of the metropolitan area that was Catholic and for church membership within the metropolitan area. Their findings illustrated that the greater the religious homogeneity in an area, the lower the suicide rate, demonstrating that heterogeneity of religion may reduce the norms and beliefs that protect individuals against suicide.
Suicide and social capital
Given Émile Durkheim’s contention that the real power of religion lies in its ability to create a community value system, it may be illuminating in terms of Durkheim’s conceptualization of religion to examine the relationship between social capital and suicide. Social capital is defined as ‘connections among individuals – social networks and norms of reciprocity and trustworthiness that arise from them … in a sense social capital is closely related to what some have called “civic virtue”’ (Putnam, 2000: 19). In communities that have high social capital the beliefs and norms within the community are known by its members. They know what is expected of them and what is not expected. In other words, the individuals in high social capital communities are socially integrated and regulated by the society, which is similar to the Durkheim’s perspective on how religion affects a community.
Studies have demonstrated that areas with high levels of social capital do have decreased suicide rates. Kelly et al. (2009) examined the level of social capital and suicide rates in 11 European countries. Using suicide data from the World Health Organization (WHO) and social capital data from the European Social Survey (ESS), they found that social capital reduced suicide. Therefore, areas where there is a clear belief and value system, much like a religious faith, have less suicide.
However, other analyses of social capital and suicide have illustrated that areas high in social capital have increased suicide rates (Flavin and Radcliff, 2009; Kushner and Sterk, 2005). Flavin and Radcliff (2009) examined social capital and suicide by state in the United States. Using Putnam’s social capital index the authors found that as the social capital index increased, suicide rates increased. Thus, they argued that social capital increased suicide. This finding is in line with the arguments made by Kushner and Sterk (2005), who examined Durkheim’s arguments about social integration and social regulation. They argued that high levels of social capital should increase suicides and asserted that high levels of social integration were correlated with suicide. Thus, Flavin and Radcliff (2009) and Kushner and Sterk (2005) demonstrated that high levels of social integration may make people more likely to commit suicide because they cannot live up to the beliefs and norms of the society. Areas with a high level of religious beliefs and values may also make individuals more likely to commit suicide, as the individuals cannot live up to the beliefs and values of the religion.
Methods
Sample
I collected suicide rates for 2000, 2005, and 2008 from the WHO, which accumulates suicide rates for countries across the world. The average of the three time periods was calculated and utilized for the current analysis. Researchers routinely use average suicide rates to control for the wide variation that can occur from year to year (Flavin and Radcliff, 2009; Kelly et al., 2009).
Another problem with cross-national suicide data is that many countries do not regularly report suicides to the WHO or collect information on the number of suicides within the nation. Countries sometimes report suicides for two time periods, but not a third. Using averages allows researchers to include a larger sample of countries in their analyses. If only one time period was used, certain countries would have to be excluded from the analysis because the rate for that particular year was not be available, and important outcome data could be lost. For example, the Dominican Republic reported suicides to the WHO for 2000 and 2005. Thus, the country was included in the current analysis, the two reported time periods being averaged. All the countries in the current analysis have reported figures to the WHO in at least at least two of the three time periods. Due to suicide data being unavailable for multiple years for a variety of countries, the final sample size of the current analysis was 41 (see Appendix).
The sample is relatively small, which could lead to problems in the statistical analysis. However, the sample size is similar to those of previous cross-national studies of suicide and other forms of deviance. For example, Flavin and Radcliff (2009) examined suicide rates across states in the United States with a sample size of 48. Other studies examining suicide cross-nationally have had a similar number of countries in their analyses, such as Chew and McCleary (1995) n = 28, Girard (1993) n = 49, Huang (1996) n = 48, Kelly et al. (2009) n = 11, Stack and Kposowa (2008) n = 31, and Stack and Kposowa (2011) n = 56. Small sample sizes are also prevalent in cross-national examinations of other types of deviance. For example, examining homicide cross-nationally, Pridemore (2008) had a sample size of 46, Pratt and Godsey (2003) 46, Savolainen (2000) 39, and Fajnzylber et al. (2002) 39. While not optimal for statistical analysis, the current analysis is consistent with other cross-national research studies and could be used as a guide for future analyses.
Independent variable
Alesina et al. (2003) created an ethnic, linguistic, and religious fragmentation index that can be applied to the different groups found within a country. I created my religious fractionalization index on the basis of their model:
where sij is the share of the group i (i =1…N) in country j. The index ranges from zero to one. A scores of zero refers to a perfectly homogeneous country (i.e., everyone in the country identifies with the same religion) and a score of one indicates a highly heterogeneous country (i.e., many different religions are practiced by members of the country). I used the CIA world factbook to collect information on religious diversity in the countries in the current analysis, as did Alesina et al. (2003) in their analysis.
I used the religious fractionalization index exclusively in the current analysis for several reasons. First, as Alesina at al. (2003) pointed out in their analysis, religion provides clearer boundaries than race and ethnicity. Second, the religious fractionalization index is less controversial because religion is not as susceptible to arbitrary classification as are ethnic and racial backgrounds. Third, ethnic and racial classifications are more subject to change than are religious classifications. Sociologists have demonstrated that an individual’s self-identification can change over time based on the social, economic, and political circumstances of the country (Alesina et al., 2003). In their examination of Somalia, McCleary and Barro (2006) demonstrated how ethnic classifications can change. Before the civil war in 1991, 85% of individuals residing in Somalia classified themselves as Somalis. After the war, the dominant ethnic classification became based on clan membership. Therefore, Somalia became heterogeneous as a result of social and political changes.
Use of a linguistic fractionalization index is also problematic, as language is used as an indicator, or even the main determinant, of ethnicity, such as Belgium and Switzerland. Therefore, we often encounter similar problems in using language to determine fractionalization as in using race. (Other countries, such as Bolivia, use racial distinctions as their main determinant of ethnicity.) Thus, to avoid some of the problems that ethnic and linguistic fractionalization indexes present, I used a religious fractionalization index to measure diversity across the countries in the sample.
Covariates
Control variables were collected from the World Bank Development Indicators. Variables were chosen as controls on the basis of their inclusion in previous cross-national research models. Population density was included in the current analysis based on Durkheim’s conceptualization of suicide. Durkheim suggested that as interactions between people became more frequent, there would be more competition for scarce resources. This ‘dynamic density’, as Durkheim termed it, would lead to more individualism (Ritzer and Goodman, 2004). The competition and individualism that occurred as people became more packed together would produce what Durkheim termed anomie. Anomie is the state of normlessness and could be characterized by feelings of loneliness, which could lead to various forms of deviance, including suicide. A number of other cross-national studies have used population density as a proxy measure of anomie (Avison and Loring, 1986; Hansmann and Quigley, 1982; LaFree and Kick, 1986; Lee, 2001; Messner, 1982; Messner and Rosenfeld, 1997; Neapolitan, 1996). The distribution of the population density in the current study was skewed. To correct for the skewed distribution, natural logarithmic transformation was used. The percentage of the population living in urban areas was also included in the current analysis, similarly based upon Durkheim’s modernization and anomie argument in relation to suicide.
To measure the level of economic inequality in a country, the GINI index was used. Scholars have pointed out some of the problems with attempting to measure economic inequality (Stack, 1984). However, the GINI index is the most common measure of inequality currently available to researchers, and its use is consistent with other research (Fajnzylber et al., 2002; Jacobs and Richardson, 2008; LaFree and Tseloni, 2006; Neumayer, 2003; Pridemore, 2008). Moreover, scholars have used the GINI index in other studies of cross-national deviance (Messner, 1982, 1989; Chamlin and Cochran, 2005) and in studies exploring development and social change (Cifuentes et al., 2008).
The level of democracy was determined by using the Freedom House (2013) democracy measure. Freedom House publishes a report on the level of civil liberties and political freedom in each country, which has been utilized in other cross-national studies. For example, Lee (2001) and Neumayer (2003) both used the data from Freedom House in their cross-national analyses of homicide, while Kedzie (2002) used Freedom House data in his analysis of technology’s influence on economic development. Level of democracy is scored on a scale of 1 to 7, with 1 representing the highest level of civil rights and political freedom and 7 the lowest level. For this analysis, the civil liberties and political freedom scores were added and then divided by two to produce an overall democracy score.
The Human Development Index (HDI) was included in the analysis as a measure of overall well-being. The Index was acquired from the United Nations Development Programme’s (UNDP) Human development report 2010. The HDI is composed of life expectancy, mean years of schooling, expected years of schooling, and gross national income per capita. Lower scores on the HDI indicate less socially developed countries.
The current analysis conducted two regression analyses. Model 1 was conducted with the HDI in the regression analysis. Because the VIF score of the HDI was .429, a second model (Model 2) was run to ensure that multicollinearity was not present in the regression analysis. Three countries that were included in the Model 2 did not have an HDI score: the Dominican Republic, India, and Nicaragua.
Findings
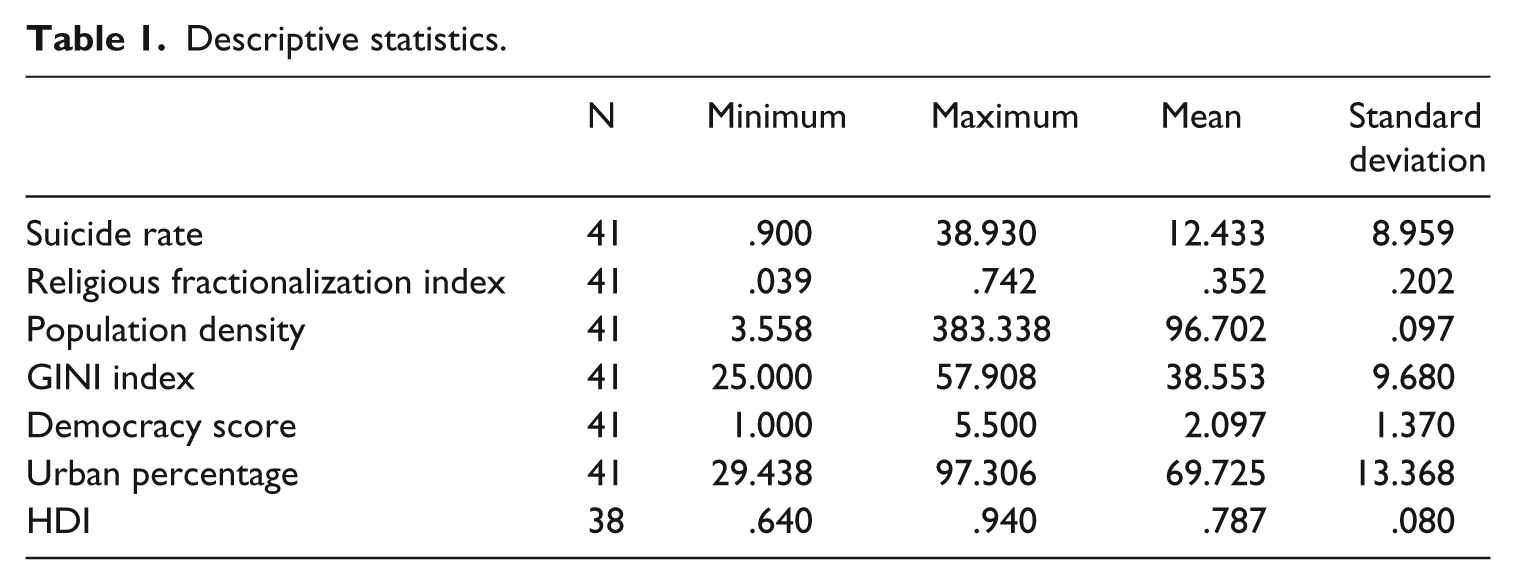
Table 1 includes the mean religious fractionalization index score for the countries in the current analysis, which was .352. Greece had the lowest level of religious diversity, with a religious fractionalization index score of .039. Venezuela (0.0776) and Ecuador (0.095) also had low levels of religious diversity as measured by the religious fractionalization index. Estonia had the highest score on the religious fractionalization index, at .742. Canada and Germany had the next highest scores, at .722 and .687, respectively.
Descriptive statistics.
From this, an argument can be made that less developed and authoritarian countries are more homogeneous with regard to religion. However, the correlations shown in Table 2 reveal that the religious fractionalization index is not strongly correlated with the level of democracy score (-.204).
Correlations.
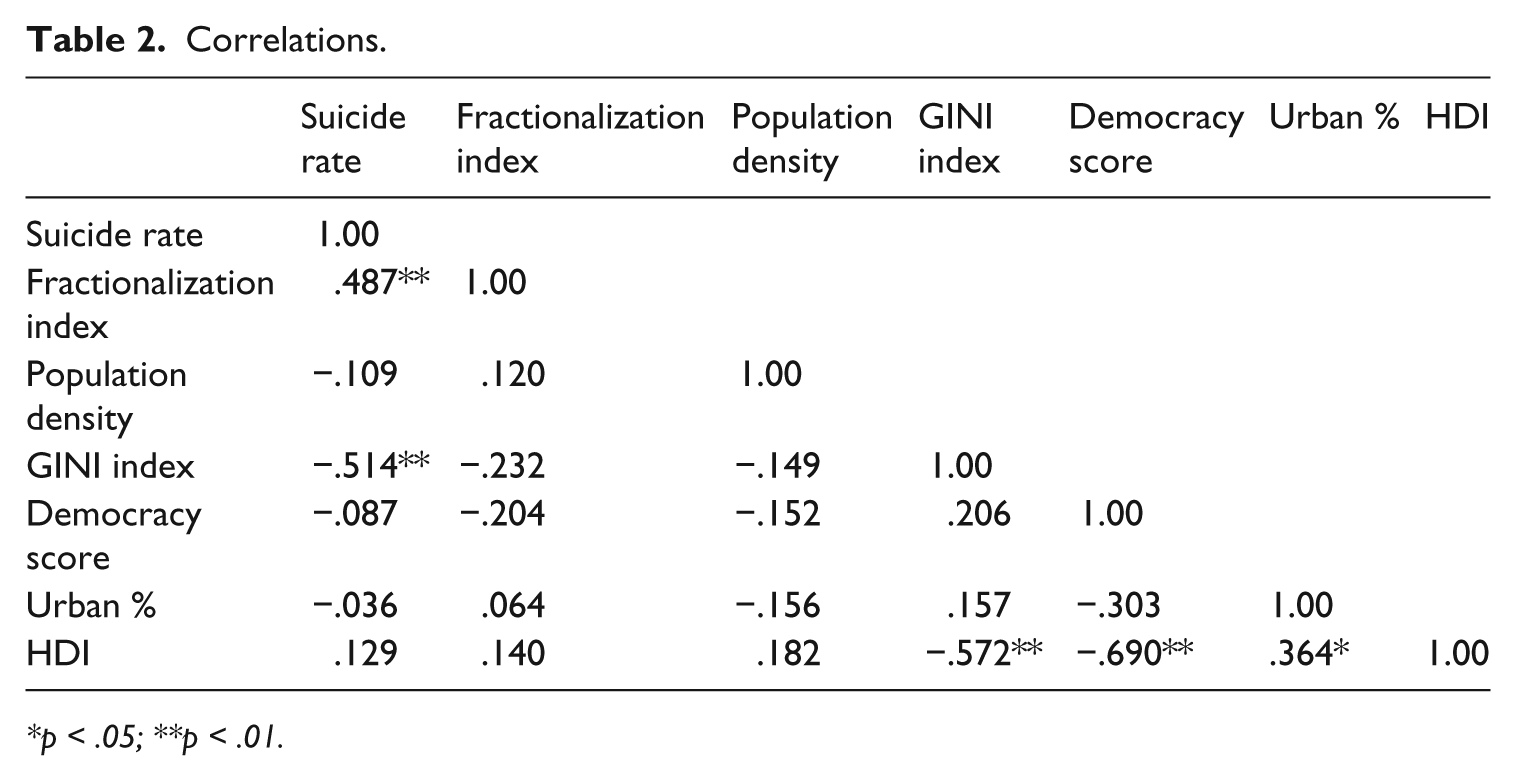
p < .05; **p < .01.
To examine the role that religious fractionalization plays in suicide, an Ordinary Least Squares (OLS) regression was used. With a small sample size, the model may be susceptible to multicollinearity. Thus, Variance Inflation (VIF) Scores were used to check for the presence of multicollinearity. Some argue that VIF scores above 10 indicate the presence of multicollinearity (Neter et al., 1989); other scholars in macrosociology have suggested that VIF scores above 5 indicate the presence of multicollinearity (Ouimet, 2012). Neither model in the current analysis had a VIF score above 5 (see Table 3). The R2 of .506 for Model 1 indicated a good fit. Furthermore, the model explained 41.1% of the variance in suicide rates for the countries in this model. This level of variance suggests an acceptable goodness-of-fit of this model considering the wide variation in heterogeneity found in each country and the cross-sectional design of the current study. The F-ratio, F(6,31) = 5.300, p < .001, for Model 1 also demonstrated that the regression model is a good fit for the data.
Ordinary Least Squares Regression analysis of suicide rates.
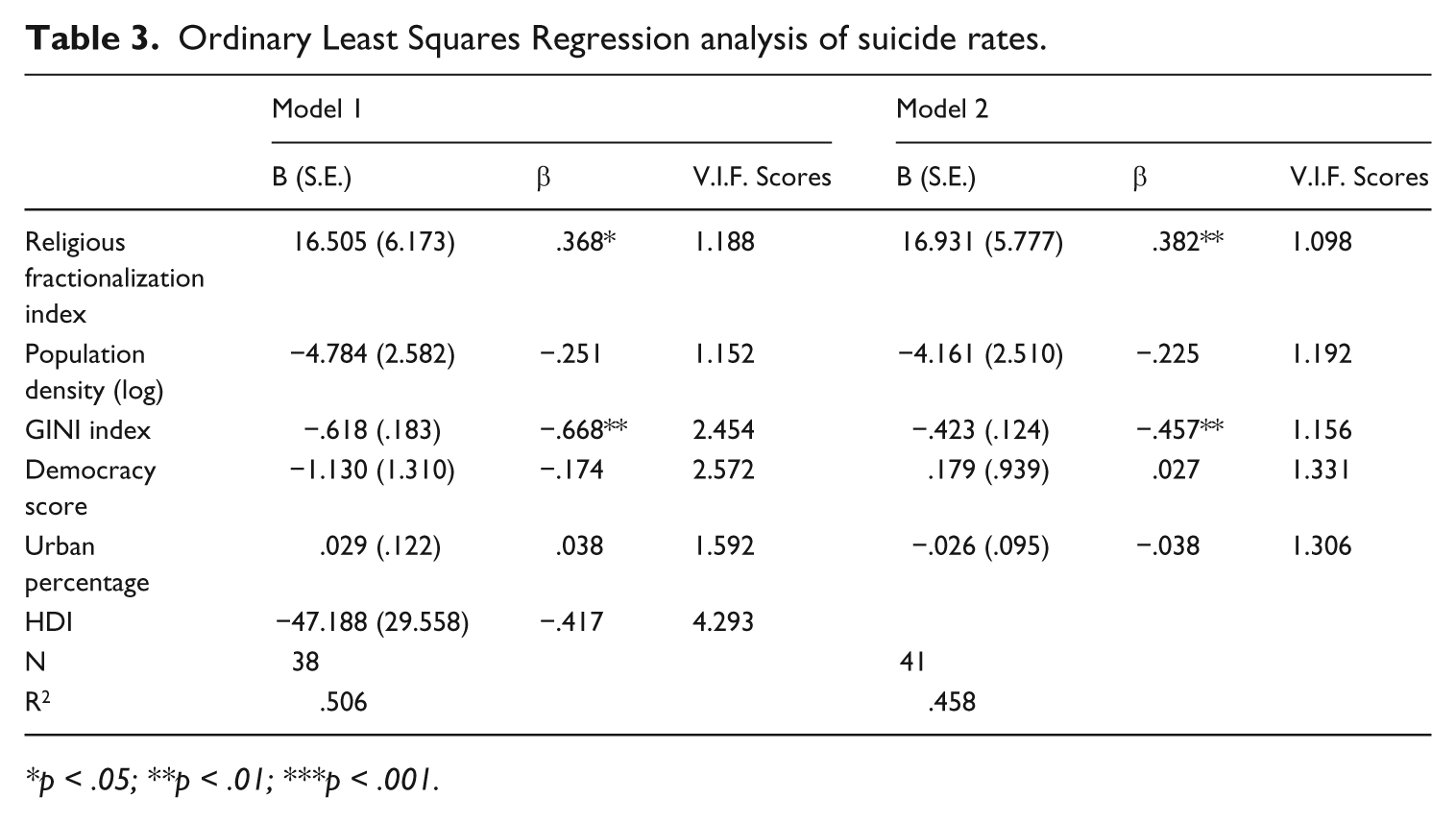
p < .05; **p < .01; ***p < .001.
Because of the small sample sizes in such cross-national analyses, any violation of the regression assumptions can have a large effect on the outcome of the analysis. A number of steps were taken to prevent any violation from biasing the results and to ensure the accuracy of the results. First, as any outliers in the model can have a large influence on the results of a regression analysis, these were controlled for. Lewis-Beck (1980) suggested that one way to deal with an outlier is to remove it from the regression analysis and examine whether any of the results change. On examination of the standard deviations and histogram plots, Lithuania was identified as an outlier for the suicide rate (38.93). Lithuania was therefore removed from the analysis, but this did not affect the results. Second, Lewis-Beck (1980) suggested that variables could be transformed to compensate for any distortion caused by outliers. Population density was therefore transformed in the current analysis to create normal distribution that would not bias the results.
The current analysis used VIF scores and examined residual plots to ensure that multicollinearity did not bias the results. The VIF scores were within the range recommended by scholars (Neter et al., 1989; Ouimet, 2012). Moreover, the residual plots did not indicate that multicollinearity was present in the current analysis. Finally, a second regression analysis was conducted without the HDI to examine whether any multicollinearity was present. The HDI had a VIF score of 4.293. While this score is under the limit suggested by Ouimet (2012), it was nevertheless the highest VIF score and was moderately correlated with the percentage of the population that lived in urban areas (-.572) and the democracy score (.690). The results of the regression with the HDI removed were not significantly different from those with the Index included. Table 3 shows the second model in the regression analysis. Model 2 explained 38.1% of the variance in suicide rates for the countries in this model. Furthermore, the F-ratio, F(5,35) = 5.917, p < .001, for Model 1 demonstrated that the regression model is a good fit for the data.
In Model 1 the religious fractionalization index was significant and positive (β = .368; p < .05). As the religious fractionalization index increased by one unit, the suicide rate increased by 16.505. This indicates that countries with more religious diversity have higher suicide rates. This finding is similar to that of Ellison et al. (1997), who found that metropolitan statistical areas in the United States with more religious heterogeneity had higher suicide rates. It also indicates that areas high in religious fragmentation do not produce the levels of social integration and social regulation that Durkheim described. Because of the different norms and values found in the different religions, there is not a consistent and overarching set of norms and values for individuals to understand and adhere to. Thus, it is likely that individuals do not become as integrated in the community. Moreover, the lack of a dominant religion implies a lack of consistent regulation of the behavior of the residents of the community. Different messages are relayed from the many different religions and none can impose its values and norms on the entire community.
The GINI index was also significant in Model 1, but negative (β = -.668; p < .01). As economic inequality decreased, the suicide rate increased. Countries with lower levels of economic inequality have increased suicide rates. Many studies on cross-national suicide fail to account for economic inequality (Huang, 1996; Kelly et al., 2009; Stack and Kposowa, 2011). However, analyses of homicide often demonstrate that economic inequality is a strong predictor (Jacobs and Richardson, 2008; Messner, 1982; Ouimet, 2012; Savolainen, 2000). The finding that more equal societies experience increased levels of suicide may seem to the opposite of what would be expected. However, Table 2 shows the correlation that the correlation between the GINI index and the suicide rate is negative. Furthermore, the HDI, which is not significant in our analysis, has a positive correlation with the suicide rate. This correlation also suggests that more socially developed countries have higher suicide rates. Moreover, in an analysis of counties in the United States, Moore et al. (2014) found that areas where the population had higher paying jobs had increased suicide rates. All of these findings may be an indication that suicide is more likely in areas that are more developed. Future cross-national studies of suicide should explore and include a measure for economic inequality to continue to examine the role played by economic inequality in suicide.
In Model 2, as can be seen in Table 3, the religious fractionalization index was significant and positive (β = .382; p < .01). As the religious fractionalization index increased by one unit, the suicide rate increased by 16.931. The GINI index was also significant and negative (β = -.457; p < .01) in Model 2. The similar results in Model 2 demonstrate that the HDI did not bias the results found in Model 1.
Conclusion
Research findings have demonstrated that religion can promote a number of pro-social beliefs and norms for a community (Ellison, 1992; Ellison et al., 1997; Lim and MacGregor, 2012; Regnerus et al., 1998). Religion has also been shown to reduce suicide (Ellison, 1992; Ellison et al., 1997) and suicidal attitudes (Stack and Kposowa, 2011). In the 19th century, Émile Durkheim contended that religion was a powerful community tool that could be used to promote pro-social outcomes, including the reduction of suicide. The current analysis was a further examination of the role that religion plays in the reduction of suicide.
Using a religious fractionalization index, it was found that countries that had many different religions rather than one dominant religion had higher suicide rates. This is in line with the findings of Ellison et al. (1997), who found that religious diversity increased the rate of suicide in metropolitan areas of the United States. Diversity of religion does not allow a common belief system and norms to be communicated to the members of the community. Instead, the many different norms and beliefs of the multiple religions leave the residents unaware of how they should behave in society.
Durkheim suggested that the real power of religion was its ability to integrate people into society and to regulate their behavior. Durkheim explained that there could be four different types of suicide, according to the degree of integration and regulation of society. Two of the four types could help to explain why religious heterogeneity would produce an increased level of suicide. Egoistic suicide occurs when an individual does not feel integrated into society (Ritzer and Goodman, 2004). A society with many different religions would not provide a community with one value system. When members of a community hold many different values and beliefs, there is less guidance as to which value system should be followed, and individuals might turn to suicide as a way to deal with their isolation.
Anomic suicide was described by Durkheim as suicide that occurs when the regulation of society is disrupted (Ritzer and Goodman, 2004). When there is one dominant religion, the values and beliefs would be clear to the society, and thus the residents would be clear on what behaviors are appropriate. They would be well regulated by the religion. Religious heterogeneity would disrupt the regulation by producing different values and norms. Therefore, individuals would not have a clear understanding of the proper behaviors and beliefs, and some individuals would turn to suicide as a way to deal with the disruption in regulation.
The current analysis provides evidence in support of Durkheim’s egoistic and anomic forms of suicide, in that religious heterogeneity tends to produce low regulation and integration for the members of the society.
Any research analysis has a number of limitations, and the current analysis is not exempt. First, the current analysis examined suicide cross-nationally with a sample size of 41. This is a small sample for statistical analysis. However, the sample size is similar to those of previous cross-national studies of suicide and other forms of deviance (Chew and McCleary, 1995; Flavin and Radcliff, 2009; Fajnzylber et al., 2002; Girard, 1993; Huang, 1996; Pratt and Godsey, 2003; Pridemore, 2008; Savolainen, 2000; Stack and Kposowa, 2008, 2011). Second, cross-national suicide data can be difficult to work with as many countries do not regularly report suicides to the WHO or collect information on the number of suicides within the nation. Thus, even when studies are well designed, it is difficult to gather a large number of countries to provide for a robust analysis of suicide.
Footnotes
Appendix
Countries included in the analysis.
| Argentina | Ireland |
| Armenia | Israel |
| Austria | Italy |
| Azerbaijan | Kazakhstan |
| Belgium | Lithuania |
| Brazil | Mexico |
| Bulgaria | Nicaragua |
| Canada | Norway |
| Chile | Panama |
| Colombia | Paraguay |
| Costa Rica | Poland |
| Croatia | Romania |
| Dominican Republic | Russia |
| Ecuador | Serbia |
| El Salvador | Spain |
| Estonia | Sweden |
| Finland | Switzerland |
| Germany | Ukraine |
| Greece | United States |
| Hungary | Venezuela |
| India |
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author biography
Address: Department of Sociology and Criminal Justice, Rasmussen Center 128, Des Moines, IA 50316, Grand View University, USA.
Email: