
Abstract
Varus posteromedial rotatory instability (VPMRI) is one of the types of complex elbow instability, which was initially proposed by O ‘Driscoll in 2003. Its typical clinical manifestations are anteromedial coronoid fracture (AMCF), injury of lateral collateral ligament complex (LCL), widening of the lateral humeroradial space, and subluxation of the coronoid process relative to the medial edge of the humeral trochlea. However, it presents diagnostic challenges due to its low incidence, complex mechanisms of injury, and radiography reveals only isolated coronoid process fractures without obvious joint space mismatch. In addition to this, the current best treatment plan for VPMRI is still controversial. Misdiagnosis and mistreatment may lead to complications such as post-traumatic arthritis, heterotopic ossification, and joint stiffness. Therefore, enhancing recognition and suspicion of VPMRI and investigating its injury mechanism, treatment strategies, surgical approaches, and internal fixation methods are essential. This narrative review conducts retrospective analysis from different perspectives, and provides imaging examples and related schematic diagrams, aiming to provide a certain reference for the precise diagnosis and treatment of VPMRI.
Keywords
Introduction
Varus posteromedial rotatory instability (VPMRI) was first proposed by O'Driscoll 1 in 2003 based on the concept of posterolateral rotatory instability (PLRI). It represents a distinct instability pattern, typically caused by varus stress, axial load, and posteromedial rotational force of the elbow joint. 2 Typical clinical manifestations include an anteromedial coronoid fracture (AMCF), injury to the lateral collateral ligament complex (LCL), widening of the lateral humeroradial space, and subluxation of the coronoid process relative to the medial edge of the humeral trochlea. In severe cases, the medial collateral ligament complex (MCL) may also be involved. 3 Although studies on VPMRI have increased in recent years with notable advances in imaging and surgical techniques, its unique injury mechanism and low prevalence continue to limit comprehensive understanding of the pathology,2,4 and the optimal choice of treatment options has not reached a consensus. This narrative review was conducted following the methodological framework of the Scale for the Assessment of Narrative Review Articles (SANRA). 5
Relevant English literature was retrieved using databases such as PubMed and Web of Science, with a search strategy that combined terms related to VPMRI and keywords associated with coronoid process fractures as well as medial and lateral collateral ligaments. This aims to elucidate the distinctive features of VPMRI from anatomy, injury mechanistic, and imaging perspectives to enhance surgeons’ recognition and management of the condition. Furthermore, it discusses appropriate management strategies to minimize therapeutic pitfalls.
Anatomical considerations
The elbow complex comprises three articulations: the humeroulnar, humeroradial, and proximal radioulnar joints.6–8 Joint stability is principally ensured through static constraints (bone, capsular and ligaments) and dynamic constraints (muscles surrounding the elbow).8,9 Based on their importance as static stabilizers, these structures are classified into primary stabilizers (the humeroulnar joint, LCL and the anterior bundle of the medial collateral ligament) and secondary stabilizers (the humeroradial joint, the common extensor group and the common flexor–pronator group).2,7 The humeroulnar joint serves as the primary stabilizing mechanism due to its unique anatomical configuration: the coronoid and olecranon form a 170° arc that encloses the trochlea, providing essential osseous containment.10,11
The coronoid has a tripartite structure consisting of the anteromedial facet (AMF), the anterolateral facet (ALF), and the sublime tubercle (ST).11,12 This critical osseous prominence enhances elbow stability through multiple mechanisms: it deepens the trochlear notch to stabilize the humeroulnar joint, resists posterior ulnar displacement, and counteracts rotational forces from posteromedial and posterolateral vectors.3,6,10,11,13 Compared with ALF, the AMF is wider and taller, 14 and nearly 60% of its structure lacks direct ulnar metaphyseal support,4,15,16 making it more susceptible to fracture. Closkey et al. 17 demonstrated that coronoid height reduction exceeding 50% significantly compromises elbow stability and functional outcomes. According to O'Driscoll's classification of coronoid fractures, larger AMF fractures or higher subtypes correlate with heightened joint instability and accelerated arthritic degeneration. 18
The LCL consists of three distinct components: the lateral ulnar collateral ligament (LUCL), the radial collateral ligament (RCL), and the annular ligament (AL). Together, these ligaments provide critical support for the humeroulnar joint. Cadaver research by Axford et al. 19 confirmed the essential role of the LCL in resisting varus stress, a finding corroborated by subsequent biomechanical analyses. 20 VPMRI typically involves avulsion of the LCL from its origin at the lateral humeral epicondyle, with radiographic evidence occasionally showing bony avulsions. Mclean et al. 21 reported universal LCL involvement in their case series. Combined AMCF and LCL injuries increase humeroulnar contact pressures, potentially inducing posteromedial subluxation and subsequent arthritis degeneration. 18
The MCL consists of three functional components: the anterior bundle (aMCL), posterior bundle (pMCL), and transverse ligament. While most literature22–24 identifies the aMCL as the primary valgus stabilizer, this appears contradictory to the injury mechanism of VPMRI, where aMCL involvement is considered rare. However, McLean's study 21 found that aMCL injury in VPMRI is more common than previously thought. Particularly for ST fracture, which is the bony insertion point of aMCL, we should be alert to the possibility of concomitant aMCL injury. The fan-shaped pMCL is traditionally considered a secondary stabilizer. However, recent biomechanical evidence3,25 has demonstrated that the pMCL plays a significant role in stabilizing the humeroulnar joint and preventing posterior subluxation of the proximal ulna. Combined pMCL tears and coronoid fractures may induce joint space widening even with an intact LCL. 25 Hwang et al. 3 demonstrated that severe elbow subluxation occurs only in the presence of an AMF fracture, an LCL tear, and a pMCL rupture.
The periarticular musculature acts as a dynamic secondary stabilizer, demonstrating particular clinical significance in chronic instability patterns. 11 Historically, injuries to the common extensor origin (CEO) and common flexor-pronator origin were rarely described in detail. Tension in the CEO muscles peaks during full pronation, enabling their maximal effect as varus stabilizers. 26 The elbow musculature serves as a dynamic restraint against varus and posterolateral instability. 11 In VPMRI patients, extensor injuries are more common; most occur at the lateral humeral epicondyle and frequently coexist with LCL injury. 21
Mechanism of injury
VPMRI most commonly occurs during a backward fall. In this scenario, the shoulder is internally rotated, the forearm is pronated, and the elbow is subjected to a combination of varus, axial, and posteromedial rotational stress. This injury involves sequential failure of key stabilizers through three progressive stages. In the initial stage, varus stress causes avulsion of the LCL from its origin at the lateral humeral epicondyle. This results in widening of the lateral humeroradial joint space. In severe cases, this avulsion may manifest as an avulsion fracture of the lateral humeral epicondyle. At this point, the radial head displaces away from the humeral head, so injuries typically do not occur.1,27 In the second stage, forearm pronation combined with sustained varus stress causes coronoid impingement against the humeral trochlea, resulting in a characteristic AMCF. When a greater force causes ST fracture, concomitant injury to the aMCL insertion should be suspected. 3 In the final stage, pMCL disruption leads to instability. The critical transition to complete instability occurs when posteromedial rotational forces overcome pMCL resistance, causing posteromedial subluxation of the humeroulnar joint 3 (Figure 1).

Typical damage mechanism diagram of VPMRI. (a) Varus force results in avulsion of the proximal lateral collateral ligament (a) and widening of the humeroradial joint space. The anteromedial articular surface of the coronoid will impinge on the trochlea, resulting in AMCF (b). (b) Further progression of the injury can result in rupture of the pMCL (c) and posterior displacement of the proximal ulna relative to the humeral trochlea (d).
Classification of coronoid fractures
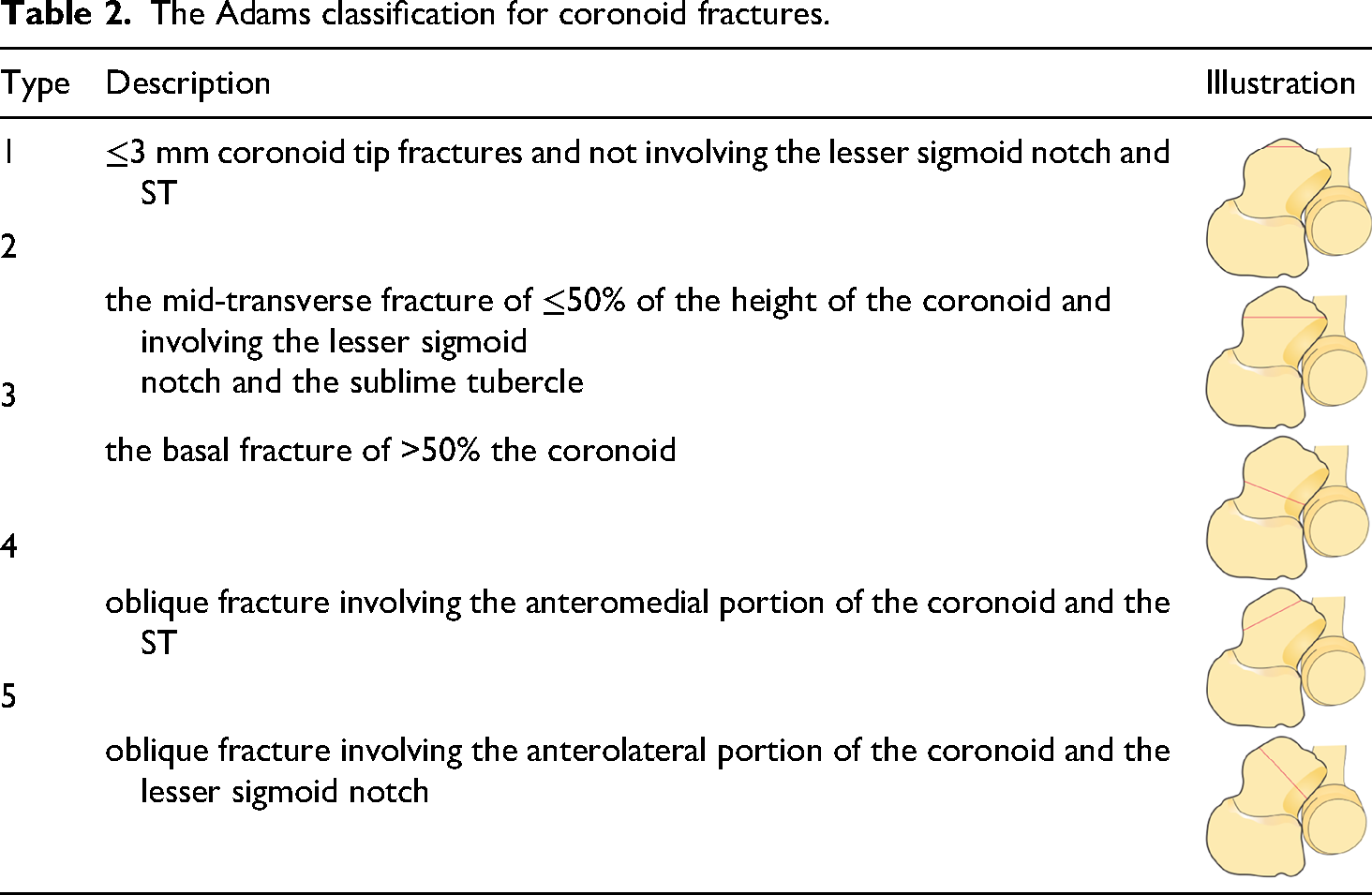
In 1989, Reagan-Morrey 28 classified coronoid fractures into three types based on fracture height observed on lateral radiographs. In 2003, O'Driscoll 1 established a refined classification of coronoid fractures based on fragment size, location, and injury mechanism, and first proposed the concept of VPMRI, establishing a correlation between this injury pattern and AMF (Table 1). In 2012, Adams et al.29 reviewed CT imaging of coronoid fractures and classified them into five subtypes with the goal of more effectively guiding clinical treatment (Table 2). Based on contemporary understanding of injury patterns and treatment needs, Wrightington classification, 6 proposed in 2019 and founded on the “three-column theory of the elbow”, provides a systematic categorization of complex elbow fracture-dislocations. This classification explicitly defines AMCF as Type A, noting its frequent association with injuries to LCL and pMCL, thereby accurately delineating the injury pattern of VPMRI. This treatment-oriented classification offers clear strategic guidance for the clinical management of VPMRI.
The O’Driscoll classification for coronoid fractures.

The Adams classification for coronoid fractures.
Diagnosis and differential diagnosis
Patients frequently present with a clear history of trauma. A meticulous inquiry should focus on the positional relationships among the shoulder, elbow, forearm, and the direction of the fall during injury. In addition to imaging and routine physical examinations, dynamic assessment for VPMRI should be performed using excessive pronation and gravity-induced varus stress tests, while varus and valgus stress tests or the posterolateral drawer test may also be utilized to evaluate elbow stability. Yet, physical examination may yield limited findings due to pain-induced muscle guarding, which often masks dislocation sensations. In VPMRI, AMCF is often considered a diagnostic linchpin. However, not all AMCF originate from the injury mechanism of VPMRI. Overly conflating AMCF with VPMRI may lead to misconstruing the nature of the injury. Therefore, distinguishing between AMCF with true VPMRI mechanics and AMCF without posteromedial rotational instability holds significant clinical value for accurate diagnosis and the selection of treatment strategies (Table 3).
Features of AMCF with true VPMRI vs. AMCF without PMRI.

PMRI: posteromedial rotatory instability.
Additionally, VPMRI is one type of complex elbow instability, and differentiation from PLRI (such as the terrible triad of the elbow) is particularly important. We attempt to distinguish them through the following points and elaborate on the special circumstances.
Firstly, radial head fractures are common in PLRI but uncommon in VPMRI. This is because the dominant varus stress in VPMRI causes the radial head to translate away from the capitellum.1,27 However, in 2006, Doornberg and Ring 27 reported that in some injuries presenting with the so-called “terrible triad” lesion (i.e. elbow dislocation, radial head and coronoid fractures). They suggested that the injury mechanism might involve varus posteromedial rotational forces rather than the typical posterolateral rotational forces. Such injury patterns increase diagnostic and therapeutic complexity, indicating that the underlying biomechanical mechanism may result from combined stresses. For these complex injuries, treatment decisions should not rely solely on the ‘terrible triad’ appearance but should include a detailed assessment of the morphological features of the coronoid fracture (such as whether imaging findings are consistent with VPMRI) and the specific instability pattern of the elbow under stress. This enables the formulation of an individualized surgical plan, which may involve addressing both bony structures and ligamentous injuries. Secondly, coronoid fracture fragments in PLRI reflect its injury mechanism, typically located at the coronoid tip and relatively small. Conversely, VPMRI fractures are often large and involve the AMF. Therefore, when the terrible triad lesion caused by VPMRI occurs, fracture morphology helps to distinguish the two types. For coronoid fractures, VPMRI management emphasizes rigid bony fixation, while the terrible triad of the elbow prioritizes soft tissues repair such as the elbow muscles and joint capsules.
Additionally, ligament injury patterns differ between these two instability types. For MCL, VPMRI typically involves pMCL lesions, while PLRI more commonly involves aMCL lesions. Of course, with current research advancements, isolated ligament injury alone does not reliably distinguish them.
Imaging examination
X-rays
On an anteroposterior radiograph, the typical findings of VPMRI include widening of the lateral humeroradial joint space, narrowing or overlap of the humeroulnar joint space, accompanied by discontinuity of the coronoid bone cortex. On a lateral view, the “double crescent sign” may be observed, which refers to the presence of two parallel or nearly parallel curved lines of high density in the coronoid region on a standard lateral elbow radiograph.2,21,30 Additionally, posterior subluxation of the elbow joint may also be present. However, due to pain after injury, patients often struggle to achieve perfectly standard anteroposterior and lateral views. It is worth emphasizing that even if a typical sign like “double crescent sign” appears on an X-ray, it cannot be directly equated with VPMRI; it is merely an important clue, not a diagnostic gold standard. Consequently, X-ray examination should serve only as a hint and preliminary reference in the diagnosis, not as the imaging basis for a final conclusion. For clinically highly suspicious cases, further CT scanning is recommended to confirm the diagnosis (Figure 2). Additionally, isolated coronoid fractures may appear on radiographs without gross malalignment, potentially leading to diagnostic oversight.

A man in his early 40 s with AMCF (a)-(d). (b) Lateral projection shows the appearance of the “double crescent sign” (arrows). (c) Humeral subtraction view shows a fracture line with medial obliquity and a concave morphology. (d) The fracture line does not extend to the anterior cortex of ST (arrow).
CT
When radiographs suggest a coronoid fracture or show no joint malalignment, three-dimensional CT reconstruction is essential to identify fractures and dislocations. It provides a precise characterization of fracture patterns and quantification of displacement, guiding surgical planning. For patients with coronoid fractures, systematic evaluation using three-dimensional reconstructed CT incorporating humeral subtraction views is recommended. This method allows for precise assessment of fracture line orientation (medially oblique, horizontal, or laterally oblique), fracture morphology (concave, flat, or convex), and fracture extent (whether it extends to ST). Additionally, careful review of all two-dimensional sequences (axial, sagittal, and coronal) is essential to identify subtle joint incongruity or subluxation. 31 In VPMRI, AMCF exhibits three characteristic imaging features: (1) an obliquely oriented medial fracture line, (2) a concave fracture morphology, and (3) extension of the fracture to the anterior cortex of ST (Figure 3). The presence of an associated avulsion fracture of the lateral epicondyle of the humerus serves as an indirect sign of LCL injury. For patients without evident dislocation on initial imaging, gravity varus stress CT may be performed to provoke and assess potential dynamic joint instability. 31 Regarding surgical decision-making, previous approaches often considered fracture fragment size or degree of displacement as key indicators. Case studies have shown that for nondisplaced or minimally displaced AMCF (especially ≤5 mm), favorable outcomes can be achieved with conservative treatment if the elbow joint remains stable.2,32–35 However, due to individual variations in coronoid cartilage thickness and the lack of standardized measurement methods, relying solely on size thresholds for decision-making is unreliable. Therefore, treatment strategies should primarily be based on a detailed analysis of fracture morphology, supplemented when necessary by stress imaging and examination under anesthesia with fluoroscopy. This comprehensive approach assesses both static and dynamic joint stability and congruity, rather than focusing solely on the degree of displacement.
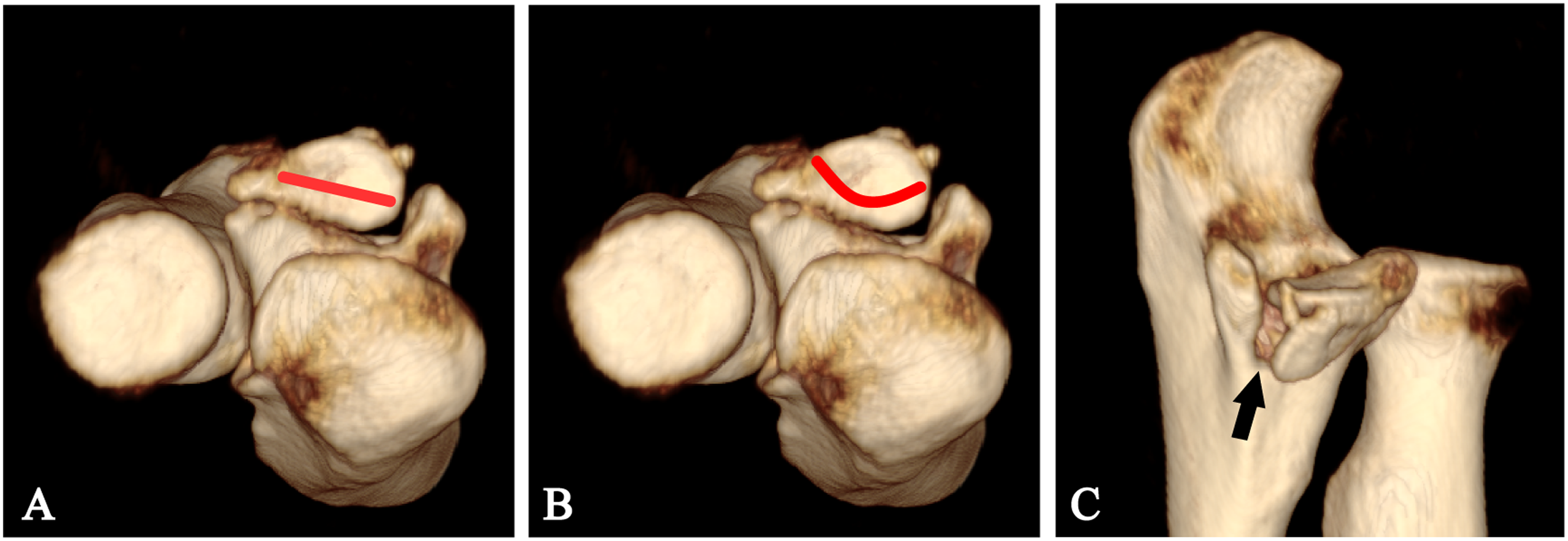
A man in his early 40 s with typical VPMRI. (a) An obliquely oriented medial fracture line. (b) A concave fracture morphology. (c) Extension of the fracture to the anterior cortex of ST.
MRI
Assessing ligament injuries via physical examination in acute elbow trauma is challenging. Reluctance to actively move the joint may indicate severe soft tissue or bony injury. MRI provides critical evaluation of soft tissues, particularly for diagnosing ligamentous and tendinous injuries obscured by patient guarding (Figure 4).

A man in his mid-40 s with AMCF, LCL injury and a pMCL tear. (a) Coronary PD fat sat MRI showing a tear in the pMCL (arrow). (b) Showing injury to the origin of the LCL (arrow). (c) Sagittal PD fat sat MRI showing significant posterior displacement of the proximal ulna relative to the distal humerus, accompanied by widening of the humeroulnar joint (star).
Ultrasound examination
Ultrasound examination is widely used in orthopedics. This technique benefits from dynamic real-time imaging, allowing visualization of ligament, flexor tendon, and extensor injuries. Examinations can target symptomatic areas precisely. Ultrasound helps identify tendon retraction, ligamentous laxity, and pathological joint space widening associated with injuries. 36
Treatment
The goal of VPMRI treatment is to restore elbow stability and function. However, current management lacks consensus on conservative treatment indications, surgical approaches and fixation methods for coronoid fractures, and the necessity of ligament repair.
Nonsurgical treatment
In contrast to historical skepticism regarding nonsurgical treatment,7,37 contemporary anatomical studies and clinical evidence have demonstrated that conservative treatment can yield favorable outcomes in select cases.32–34 Pollock's cadaveric study indicated that AMCF fragment size significantly affects elbow stability. Both AMCF fragment dimensions and the severity of concomitant ligament damage may critically determine the need for open reduction and internal fixation. These findings support conservative management for Type I fractures with fragments <2.5 mm and intact MCL, even those with LCL involvement. 18 Chan et al. 32 adopted a nonsurgical regimen focused on early rehabilitation for 10 patients with AMCF. This protocol involved short-term immobilization using a posterior elbow splint after injury, followed by supervised, progressive functional exercises initiated early (typically within 10–14 days post-injury). After a mean follow-up of 50 months, all patients achieved satisfactory elbow range of motion and Mayo Elbow Performance Scores, with bony union of the fractures and no complications such as joint instability or post-traumatic arthritis. Foruria et al. 34 studied 28 acute isolated coronoid fracture patients, reporting that conservative treatment achieved good outcomes in 90% of cases. Regardless of coronoid fragment position or soft tissue injury severity, conservative treatment could be applied when fracture height was <50% and ST remained intact. Previous studies have suggested that for subtype 2 of the O'Driscoll anteromedial facet type fracture, nonsurgical treatment may be considered if the elbow joint can maintain concentric reduction and the fracture displacement is minimal (≤3 mm). 32 The latest treatment principles further emphasize that clinical decisions should be based on a precise assessment of the instability pattern. Specifically, if an AMCF assessed via three-dimensional CT (particularly with humeral subtraction views) does not simultaneously meet all three characteristic imaging features (Figure 3), lacks factors affecting fracture healing such as soft tissue interposition, and can maintain joint congruity, it can achieve favorable outcomes through standardized nonsurgical treatment. 31
Surgical treatment
Surgical approach
The choice of surgical approach must balance adequate exposure for fracture management against minimizing iatrogenic neurovascular injury. RING 37 noted that a single posterior median approach provides extensive elbow joint access with high safety. Current anatomical understanding provides diverse surgical approach options, including anterior, posterior, medial, and lateral directions, for comprehensive elbow management. The AMCF is typically addressed via the medial approaches, 38 most commonly the “over-the-top” (Hotchkiss) approach and flexor carpi ulnaris (FCU) split approach. Since VPMRI is occasionally accompanied by MCL injury, surgical planning must ensure exposure permits both fracture fixation and the exploration and repair of MCL. Comparative studies38,39 demonstrate the “over-the-top” approach better exposes coronoid tips in shear fractures, while the FCU-split approach provides superior visualization of ST and aMCL. For fractures requiring plate fixation, the choice of surgical approach depends on the exposure needed to address the specific structures involved, ensuring accurate and stable placement of the plate. For O'Driscoll type I/II fractures, which primarily involve the coronoid tip and AMF, the “over-the-top” approach can be employed. This approach provides adequate exposure of AMCF and allows for subperiosteal dissection to prepare the bone bed for an anteromedial buttress plate. In contrast, type III fractures involve ST, where a more direct and extensive exposure of the entire medial coronoid surface is critical for precise plate placement. Therefore, these fractures are better addressed via the “FCU-splitting” approach, which also facilitates assessment and repair of MCL. In VPMRI, LCL is frequently avulsed from the lateral humeral epicondyle. The Kocher approach is commonly employed for LCL exploration and repair. The lateral approach may be optimal only when coronoid fractures involve small fragments with concomitant radial head fractures. For isolated coronoid fractures, this approach provides limited exposure that often precludes precise fracture fixation. When MCL repair is unnecessary, the lateral approach offers a minimally invasive option for managing both LCL injuries and coronoid fractures through dorsal K-wire fixation. However, achieving optimal fixation without clear anatomical landmarks under restricted visualization requires substantial technical expertise and tactile proficiency, typically attainable only by experienced surgeons.
Coronoid fractures
Coronoid fracture treatment is guided primarily by O'Driscoll classification and fragment characteristics. Current fixation options include plates, screws, K-wires, tension bands, suture lasso techniques, coronoid reconstruction, and arthroscopy.40–44 Plates and screws remain the most common methods, demonstrating satisfactory outcomes in most cases12,40–42,45,46

A man in his early 40 s with VPMRI. (a) 3D CT reconstruction showing fractures of the AMF, ALF and ST (arrows). (b) Anteroposterior and (c) Lateral elbow radiographs showing surgical fixation of the coronoid fractures using plate.

A man in his late 20 s with VPMRI A 3D CT reconstruction showing the AMCF (arrow). (b) Sagittal CT showing significant displacement of the coronoid fractures (arrow). (c) Anteroposterior and (d) lateral elbow radiographs showing surgical fixation of the coronoid fracture with screw.
Previous literature emphasized surgical intervention when the coronoid fragment height exceeded 2.5 mm or accounted for more than 15% of the total coronoid height. 35 However, recent studies highlight that for isolated coronoid fractures involving AMF, the clear indication for surgery should be based on evaluation using three-dimensional reconstructed CT incorporating humeral subtraction views. If the AMCF simultaneously exhibits all three imaging features (Figure 3), surgical treatment is recommended. This should be further confirmed by fluoroscopic examination under anesthesia to verify elbow instability, thereby determining the specific repair strategy.31 This updated criterion shifts the surgical indication from simple fragment measurement to an assessment of the underlying injury mechanism and stability, thus providing a more precise basis for clinical decision-making.
Ligament repair
One characteristic feature of VPMRI injuries is associated damage to the LCL. However, it is essential to distinguish between a simple AMCF and a VPMRI pattern as a distinct clinical-pathological entity, as not all AMCF stem from a VPMRI mechanism. 31 This distinction is crucial when discussing the necessity for ligament repair, as the management principles differ between the two. Masouros et al. 12 proposed that for O ‘Driscoll type I coronoid fractures, stability can be achieved solely through LCL repair. For O'Driscoll type II/III coronoid fractures, LCL repair is often necessary alongside coronoid fixation to restore elbow stability.2,18,50 Recent studies also suggest LCL repair may not always be required.51,52 After rigid coronoid fixation, a hanging arm test can assess humeroradial or humeroulnar joint dislocation; LCL repair can then be decided based on the findings. 52 However, in the surgical management of true VPMRI, repair of the lateral collateral ligament is generally advocated to address the underlying rotatory instability. All favorable clinical outcomes reported are derived from surgical protocols in which LCL repair constitutes a core component.21,31 Although prospective studies are currently lacking to confirm whether equally excellent efficacy and stability can be achieved without ligament repair in true VPMRI, under the current level of evidence, performing ligament repair for confirmed VPMRI remains a literature-supported standard surgical principle. Additionally, MCL injuries may be overlooked during treatment because MCL primarily resists valgus stress, which is opposite to the injury mechanism of VPMRI. 4 Some evidence indicates that failing to repair the injured pMCL may cause persistent instability. 25 If instability persists after coronoid fixation and LCL repair, MCL repair should be considered. 3 Ligament therapy primarily includes repair and reconstruction techniques. Repair techniques encompass direct repair, drilling repair, and suture anchor repair. 53 Currently, the main reconstruction techniques are the modified “Jobe” technique and the “docking” technique. 54 Through a systematic review, Spears concluded that suture-reinforced repair and reconstruction of the ulnar collateral ligament of the elbow are biomechanically equivalent and demonstrate good clinical results. 55 Almigdad performed anchor-based direct repair of the LUCL in all 15 patients. At a mean follow-up time of 26 months, 12 patients had excellent results, while 3 had good results. All patients achieved functional range of motion, with a mean loss of 11.3° in terminal extension and 5° in terminal flexion. 56
Hinged external fixator
The purpose of a hinged external fixator is to maintain concentric alignment of the humeroulnar joint during elbow motion while protecting bony structures and ligaments. 57 When fractures are too small or comminuted for stable fixation, or when ligament repair is challenging, external fixation becomes necessary. Unlike plaster casts, which restrict motion and risk stiffness, this device provides stability while permitting early mobilization. Critical to its success is precise placement of the rotational axis pin, which must align exactly with the capitellum-trochlear axis. Malpositioning elevates articular stress during movement. Ma et al. 58 addressed this challenge using 3D-printed guides to position the axis pin, achieving optimal alignment with subsequent improvements in elbow range of motion and functional outcomes.
Discussion
Recent studies indicate growing interest in VPMRI among surgeons. The condition's low diagnosis and treatment rates primarily stem from two factors. First and foremost, its complex injury mechanism and distinctive imaging features result in insufficient clinician recognition. Specifically, an isolated coronoid fracture without radial head involvement should raise suspicion for VPMRI. However, it must be clarified that not all AMCF constitute a VPMRI pattern. True VPMRI specifically refers to a distinct injury pattern caused by a varus-posteromedial rotational mechanism, characterized by objective instability. Its diagnosis should be based on dual criteria: first, the identification of three characteristic AMCF features consistent with the VPMRI mechanism through three-dimensional CT (particularly with humeral subtraction views); second, the confirmation of pathological varus and posteromedial rotational instability of the elbow joint through dynamic stress examination under anesthesia. This distinction is crucial to avoid overtreatment of stable AMCF while ensuring proactive intervention for VPMRI.
In addition, the decision between conservative and surgical management has historically focused on fracture fragment size and displacement. However, as noted previously, anatomical variations and the absence of a uniform measurement standard make decisions based purely on fracture size thresholds unreliable. Recent approaches emphasize a precise assessment of the instability pattern. Using three-dimensional reconstructed CT incorporating humeral subtraction views, the fracture is evaluated against the three definitive radiographic features of true VPMRI: (1) a medially oblique fracture line, (2) a concave fracture morphology, and (3) extension of the fracture to the anterior cortex of ST. 31 If all three features are present, surgical intervention is indicated. 31 The standard surgical protocol, confirmed by instability under fluoroscopic examination with anesthesia (including varus and valgus stress tests, hyperpronation and hypersupination tests, and gravity varus stress views), typically involves open reduction and internal fixation of the coronoid + LCL repair ± pMCL repair. If the fracture does not meet all three criteria, the key decision-making factor shifts to the ability to maintain joint congruity. 31 If congruity can be preserved, and there are no soft-tissue interposition or other factors impairing fracture healing, nonsurgical management may be appropriate. This requires a thorough discussion of potential risks with the patient. The initial immobilization and early rehabilitation protocol described by Badre for non-operative treatment can be applied. 31 During the conservative treatment period, joint alignment must be closely monitored through regular clinical assessments and serial radiographs. Any signs of joint incongruity or dynamic instability warrant immediate re-evaluation and consideration for surgical intervention. For surgical treatment, the optimal fixation method and surgical approach remain debated. We reviewed surgical approaches, coronoid fixation strategies, and ligament management. However, current evidence relies heavily on case reports lacking high-level support and often addresses isolated injuries rather than systematic VPMRI management. Despite these limitations, we maintain that for coronoid fractures constituting true VPMRI, plate-screw fixation via a medial approach is often beneficial. Secondly, based on current evidence in the literature, repair of LCL is necessary. Finally, the decision to repair the pMCL should be determined based on the intraoperative assessment of stability.
Conclusions
Overall, despite the diagnostic and therapeutic challenges in managing VPMRI, Future studies should focus on two key areas: Firstly, conducting multicenter prospective studies with larger cohorts is necessary to establish optimal VPMRI treatment protocols. Secondly, the diversity of coronoid fracture patterns highlights the need to investigate injury mechanisms and assess whether current classifications adequately correlate fracture morphology with injury patterns in VPMRI. Such evidence will advance our understanding of pathomechanics and guide precision treatment, ultimately improving VPMRI management outcomes.
Footnotes
Acknowledgments
We express our gratitude to all participants for their valuable insights and helpful discussions.
Consent for publication
The imaging data in this article were obtained from the Affiliated Hospital of Shandong University of Traditional Chinese Medicine, and consent for publication has been obtained.
Author contributions
All authors contributed to the study conception and design. SKH conducted the literature review and was the primary contributor to the manuscript writing and figure generation. PYD provided the relevant materials, and JRZ and YDL conducted the literature review. BY and YXY were the main contributor in reviewing the manuscript. All authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Shandong Province, Shandong University of Traditional Chinese Medicine Graduate Program Quality Improvement and Innovation Project, the Clinical Medical Science and Technology Innovation Program of the Jinan Science and Technology Bureau, Science and Technology Co-construction Project of the National Integrated Reform Demonstration Zone for Traditional Chinese Medicine, (grant number ZR2022MH021, YJSTZCX2025163, 202430051, NO.GZY-KGS-SD-2024-086).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.