
Abstract
Objective
The purpose of this study is to further investigate the diagnostic value and precise localization of 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography (68Ga-PSMA PET/CT) for preoperative pelvic invasion in prostate cancer (PCa) patients in comparison with multiparametric MRI (mpMRI), in order to explore the better clinical diagnostic recommendations.
Patients and methods
The clinical data of 118 PCa patients who underwent 68Ga-PSMA PET/CT and mpMRI, including the patients with Pelvic invasion (n = 46) and No pelvic invasion (n = 72), was collected from May 2019 to June 2024. The correlation between the maximum standardized uptake value (SUVmax) of 68Ga-PSMA-11 PET/CT, Prostate Imaging Reporting and Data System (PI-RADS) of mpMRI and serum prostate-specific antigen (PSA) levels, and Gleason score was analyzed and explored. Thereafter, both modalities were directly compared for every patient and PCa lesion in the terms of pelvic invasion by all collected and analyzed data. In addition, the sensitivity and specificity of 68Ga-PSMA PET/CT and mpMRI were verified by postoperative hematoxylin-eosin staining and PSMA immunohistochemistry of intraoperative localized microcarcinoma.
Results
Analyzing the clinical and imaging data of PCa patients, it was found that the SUVmax of 68Ga-PSMA-11 PET/CT and PI-RADS of mpMRI had a positive correlation with the PCa patients’ serum PSA and Gleason score. In addition, SUVmax, PI-RADS and PSA, Gleason score of PCa patients with pelvic invasion were significantly higher than those without pelvic invasion. After further data analysis, 68Ga-PSMA-11 PET/CT presented the sensitivity and specificity of 95.56% and 95.89%, respectively. Moreover, mpMRI demonstrated the sensitivity and specificity of 93.18% and 93.24%, respectively. There was no significant statistical difference between them. Meanwhile, the comparison between 68Ga-PSMA PET/CT and mpMRI in the diagnosis of lymph node metastasis was similar.
Conclusions
Both 68Ga-PSMA PET/CT and mpMRI have high sensitivity and specificity in the detection of primary PCa lesions with pelvic invasion. Despite the excellent performance of 68Ga-PSMA PET/CT in the diagnosis of small PCa lesions, it cannot replace the diagnostic value of mpMRI in localization and staging of PCa.
Introduction
Prostate cancer (PCa), with the increasing morbidity and mortality worldwide, is the second most frequently diagnosed and fifth most aggressive tumor in men. 1 With an estimated one in 25 men undergoing prostate examination around the world is likely to be diagnosed with PCa within his lifetime.1,2 As in China, PCa is the seventh most diagnosed cancer and the tenth main cause of tumor mortality. 3 Therefore, the early detection of PCa plays a vital role in assessing the progress and treatment strategies of disease. Traditionally, the diagnosis of PCa has been mainly relied on digital rectal examination and prostate-specific antigen (PSA) testing with prostate biopsy guided by transrectal ultrasound.2–4 Although PSA is a valuable biomarker for the detection of PCa, it is organ-specific rather than cancer-specific. This lack of specificity might lead to over-diagnosis and over-treatment. 4 In this setting, there is a need for non-invasive and more accurate measures in the detection of PCa lesions.
Imaging examination plays an extremely important role in the diagnosis and staging of PCa. 5 Multiparametric MRI (mpMRI) is a kind of non-invasive imaging examination that has shown the considerable promise in the staging and detection of PCa.4,6 In recent years, mpMRI has increased the diagnostic accuracy of PCa with the use of prostate imaging reporting and data system (PI-RADS). Nowadays, it suggested that 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography (68Ga-PSMA PET/CT) has emerged as a viable staging tool which was first described in 2012. 7 PSMA is a type 2 transmembrane glycoprotein that is highly overexpressed in PCa, which can be targeted by ligands for imaging and treatment purposes. 8 68Ga-PSMA PET/CT has higher sensitivity and specificity, compared to conventional imaging examination such as bone scintigraphy and computerized tomography. 9 68Ga-PSMA PET/CT is especially beneficial in the setting of biochemical recurrence of PCa after local treatment. This is mainly because of its superior detection rate compared with conventional imaging and with previously established radiotracers such as radiolabeled choline.10–12
In this study, pelvic invasion included seminal vesicle invasion, lymph nodes invasion, skeletal metastases, rectum, or bladder invasion. 13 To our knowledge, considering the differences in the diagnosis of PCa between 68Ga-PSMA PET/CT and mpMRI is existed, and the potential benefit and comparison of 68Ga-PSMA PET/CT and mpMRI for the staging in PCa patients with pelvic invasion have not yet been investigated. Therefore, the purpose of this study is to further compare the diagnostic value and precise localization of 68Ga-PSMA PET/CT for preoperative pelvic invasion in PCa patients in comparison with mpMRI, in order to explore the better clinical diagnostic recommendations.
Patients and methods
Patient characteristics
From May 2019 to June 2024, a total of 118 patients diagnosed with PCa, who underwent 68Ga-PSMA PET/CT and mpMRI at the same period, including pelvic invasion (n = 46) and no pelvic invasion (n = 72), were included in this study by all collected and analyzed clinical data. Laparoscopic radical prostatectomy (RP) with or without lymph node dissection was performed 4–6 weeks after prostate biopsy. The time interval between imaging examination (68Ga-PSMA PET/CT and mpMRI) and RP was no more than 40 days in this study. Para-aortic and pararectal nodes were removed only if positive sentinel lymph node was found. The tissue specimen was prospectively mapped and labeled separately according to the anatomic regions just listed and sent for histopathologic examination. Therefore, it is to compare the diagnostic value of 68Ga-PSMA PET/CT and mpMRI for preoperative pelvic invasion in PCa patients.
Study exclusion criteria were as follows: (1) have taken a 5α-reductase inhibitor in the past month; (2) have had prostate-related surgery and treated; (3) combine with other types of tumor; and (4) lack of clinical data. The study protocol was reviewed and approved by the Ethics Committee of Nanjing First Hospital, Nanjing Medical University (YW20190124-07). Written informed consent was obtained from all participants prior to their enrollment. This study was conducted in full conformity with the ethical standards of the Declaration Helsinki (1975, revised 2024). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 14
The clinical characteristics of all PCa patients are summarized in

Patient flowchart.
Clinical characteristics of the patients included in this study (n = 118).

Continuous data are reported as median (range). SUVmax: maximum standardized uptake value; PI-RADS: Prostate Imaging Reporting and Data System; PSA: prostate-specific antigen; RP: radical prostatectomy; RP + ePLND: radical prostatectomy + pelvic lymph node dissection.
All patients diagnosed with PCa by prostate biopsy have undergone 68Ga-PSMA PET/CT and mpMRI prior to the surgery. Maximum standardized uptake value (SUVmax), as the uptake value of 68Ga-PSMA-11 in the performance of PCa, reflected the size and range of PCa positive lesions. The mean SUVmax was 19.94 ± 15.67 MBq (4.36–89.6 MBq) in this study. In addition, PI-RADS was based on the comprehensive scores of prostate T2-weighted imaging (T2WI), diffusion-weighted imaging (DWI), and dynamic contrast-enhanced imaging, which gave a score for the possibility of clinically significant PCa. The PI-RADS of all PCa patients ranged from 2 to 5, including 5 (4.2%) with PI-RADS score=2, 28 (23.7%) with PI-RADS score=3, 50 (42.4%) with PI-RADS score=4, 35 (29.7%) with PI-RADS score=5. In terms of initial stage, T2 was 88 (74.6%), and 30 (25.4%) of initial stage were T3. After excluding surgical contraindications, all patients underwent surgical treatment, 86 patients underwent laparoscopic RP, and 32 patients underwent laparoscopic radical prostatectomy + pelvic lymph node dissection (RP + ePLND).
68Ga-PSMA-11 PET/CT examination and analysis
The 68Ga-PSMA-11 was prepared with an ITG semi-automated module (Munich, Germany). 68Ga-PSMA-11 was stable and had high radiochemical purity after 2 h of radiolabeling in vitro, which tested by analytical reverse phase high-performance liquid chromatography. All the patients were treated with proper hydration on the day of the study. Each patient was administered an intravenous injection of 68Ga-PSMA-11 (median, 131.72 MBq, range 130.6–177.6 MBq) and rested for 60 min. The patient then underwent PET/CT in a uMI 780 PET/CT scanner (United Imaging Healthcare (UIH), Shanghai, China). All patients were scanned from the vertex through the proximal legs. CT acquisition was performed on a spiral CT scanner, with a slice thickness of 5 mm and a pitch of 1. When CT scan was finished, 3D-PET images required the patient to assume four bed positions with 2 min per bed position for the same landmarks. Images were reconstructed using an iterative reconstruction algorithm (two iterations, 21 subsets). The UIH WorkStation software was used to calculate the SUVmax and the uptake of 68Ga-PSMA-11 was quantified SUVmax.
mpMRI examination and analysis
For these patients undergoing mpMRI, 3 Tesla (T) MR scanner (Erlangen, Germany) with a specific imaging protocol for the prostate was used. The protocol consisted of an initial T2-weighted (T2 W) single-slab 3D TSE sequence with slab selective, variable excitation pulse which was reconstructed in an additional coronal and sagittal plane, followed by a further T2 W sequence with a focus to the prostatic fossa. Two separately performed sequences with DWI (p-values 0, 500, 1000, 2000) and apparent diffusion coefficient (ADC) were both focused on the whole pelvis and again the prostatic fossa. T1-weighted (T1 W) axial VIBE sequences were included before and after contrast medium administration. During contrast injection, T1 W VIBE perfusion imaging was performed.
Histologic examination
The pathologist received the tissue specimens, including the prostate gland and the lymph nodes, which was fixed in buffered formalin, embedded in paraffin, and sectioned in 4 mm slices. The slices were both stained with hematoxylin-eosin (H&E). Two experienced pathologists who were blind to the imaging determined the TNM stage, according to the TNM classification. Pathologic stage at laparoscopic RP was used as the reference standard for extracapsular extension and seminal vesicle invasion. Histologic findings in all cases were reevaluated by two experienced genitourinary pathologists unblinded to clinical information and blinded to all imaging results, using a standard protocol. After the completion of the PET acquisition and mpMRI examination, the images were assessed clinically by two experienced nuclear medicine physicians and radiologists who were blinded to the clinical findings and structural imaging. The final decision would reach a consensus. For immunohistochemical analysis of PSMA binding, the slices were incubated with the PSMA at 37 °C for 2 h. Then, after three washes with PBS, sections were incubated with horseradish peroxidase-labeled secondary antibody for 1 h at room temperature. The bound antibody complexes were detected by a diaminobenzidine detection system, and the immunostained images were observed with microscope.
Statistical analysis
Analyze the 68Ga-PSMA PET/CT and mpMRI in diagnosis of primary PCa and pelvic invasion lesions, including seminal vesicle invasion, lymph nodes invasion, skeletal metastases, rectum or bladder invasion. The correlation between SUVmax, PI-RADS and serum PSA levels, and Gleason score was calculated by Spearman. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for primary PCa, pelvic invasion and lymph node status of 68Ga-PSMA-11 PET/CT and mpMRI were calculated, respectively. Descriptive data were presented as Mean and standard deviation (SD) for normally distributed variables. Paired student's t-test was used to evaluate differences among normally and non-normally distributed variables. Statistical analysis was carried out with SPSS 22.0 and GraphPad Prism5; and p < 0.05 was considered significant.
Results
Correlation analysis of SUVmax and clinical performance
In order to study the correlation between the total serum PSA, Gleason score, SUVmax, and PI-RADS of all PCa patients, the results found that, with the increasing of SUVmax of PCa patients, serum PSA or Gleason score or PI-RADS score of PCa also increased in these patients (
Patient characteristics according to SUVmax and clinical performance.

SUVmax: maximum standardized uptake value; PI-RADS: Prostate Imaging Reporting and Data System; PSA: prostate-specific antigen.
Difference analysis of pelvic invasion or not in PCa patients
According to the pathological results, all patients were divided into two groups: pelvic invasion group and non-invasion group, of which 46 cases (38.98%) were in the invasion group and 72 cases (61.02%) were in the non-invasion group. The patient characteristics stratified by the pelvic status are summarized in
Patient characteristics stratified by the pelvic status.

Continuous data are reported as median (range). Bold values indicate statistical significance.
ASA: Anesthesiologists Society of America; SUVmax: maximum standardized uptake value; PI-RADS: Prostate Imaging Reporting and Data System; PSA: prostate-specific antigen.
The serum PSA level of the PCa patients with or without pelvic invasion was 30.98 ng/ml (range 5.65–176.5) and 12.66 ng/ml (range 4.68–288.0), respectively (p = 0.005). Gleason score also had significant difference between with or without pelvic invasion (p = 0.001). The SUVmax (p = 0.001) and PI-RADS (p = 0.001) of the patients with pelvic invasion were both significantly higher than those without pelvic invasion. The above results also indicated that these patients with pelvic invasion of PCa have higher malignant potential, compared with those without pelvic invasion.
Comparison of the diagnostic value of 68Ga-PSMA PET/CT and mpMRI in PCa patients with pelvic invasion
Diagnostic performances of 68Ga-PSMA PET/CT and mpMRI for the pelvic invasion: per-patient analysis (n = 118).

NPV: negative predictive value; PPV: positive predictive value; 68Ga-PSMA PET/CT: 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography; mpMRI: multiparametric MRI.
After further data analysis, 68Ga-PSMA-11 PET/CT presented the sensitivity, specificity, PPV and NPV of 95.56%, 95.89%, 93.48% and 97.22%, respectively. Moreover, mpMRI demonstrated the sensitivity, specificity, PPV and NPV of 93.18%, 93.24%, 89.13%, and 95.83%, respectively. These results indicated that both 68Ga-PSMA PET/CT and mpMRI had a certain diagnostic value in the detection of PCa with pelvic invasion, and no significant statistical difference was found.
Detection analysis of pelvic lesion with 68Ga-PSMA PET/CT and mpMRI
Among the 118 PCa patients included in this study, the postoperative pathology results of 46 patients indicated the presence of pelvic invasion. Subsequently, these patients were grouped according to the specific location of pelvic invasion, including seminal vesicle invasion, lymph nodes invasion, skeletal metastases, bladder, or rectum invasion. 43 cases were detected the presence of pelvic invasion by 68Ga-PSMA PET/CT, including 28 patients with seminal vesicle invasion, 32 patients with lymph nodes invasion, 18 patients with skeletal metastases, 5 patients with rectum or bladder invasion. In addition, 41 patients were detected pelvic invasion the presence of pelvic invasion by mpMRI, and 21, 26, 14, and 4 patients with invasion of seminal vesicle, lymph nodes invasion, skeletal metastases, and bladder or rectum invasion, respectively (
Comparison between 68Ga-PSMA PET/CT and mpMRI in the patients with prostate cancer (n = 118).

Ga-PSMA PET/CT: 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography; mpMRI: multiparametric MRI.
Analysis of 68Ga-PSMA PET/CT and mpMRI in the diagnosis of metastatic lymph nodes of PCa
Among 46 PCa patients with pelvic invasion, 32 patients were diagnosed with lymph nodes invasion.
The results of 68Ga-PSMA PET/CT and mpMRI in the detection of lymph nodes metastasis in the patients with pelvic invasion (n = 46).

Ga-PSMA PET/CT: 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography; mpMRI: multiparametric MRI.
The diagnostic value of 68Ga-PSMA PET/CT and mpMRI in clinical staging and surgical approaches of patients with pelvic invasion of prostate cancer

The performance of mpMRI and 68Ga-PSMA PET/CT in the PCa patient with seminal vesicle invasion. (A) T2WI sequence of mpMRI; (B) DWI sequence of mpMRI; (C) CT; (D) 68Ga-PSMA PET/CT; (E) H&E staining; (F) PSMA immunohistochemistry. 68Ga-PSMA PET/CT: 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography; PCa: prostate cancer; mpMRI: multiparametric MRI; T2WI: T2-weighted imaging; DWI: diffusion-weighted imaging; H&E: hematoxylin-eosin.
The T2WI sequence (
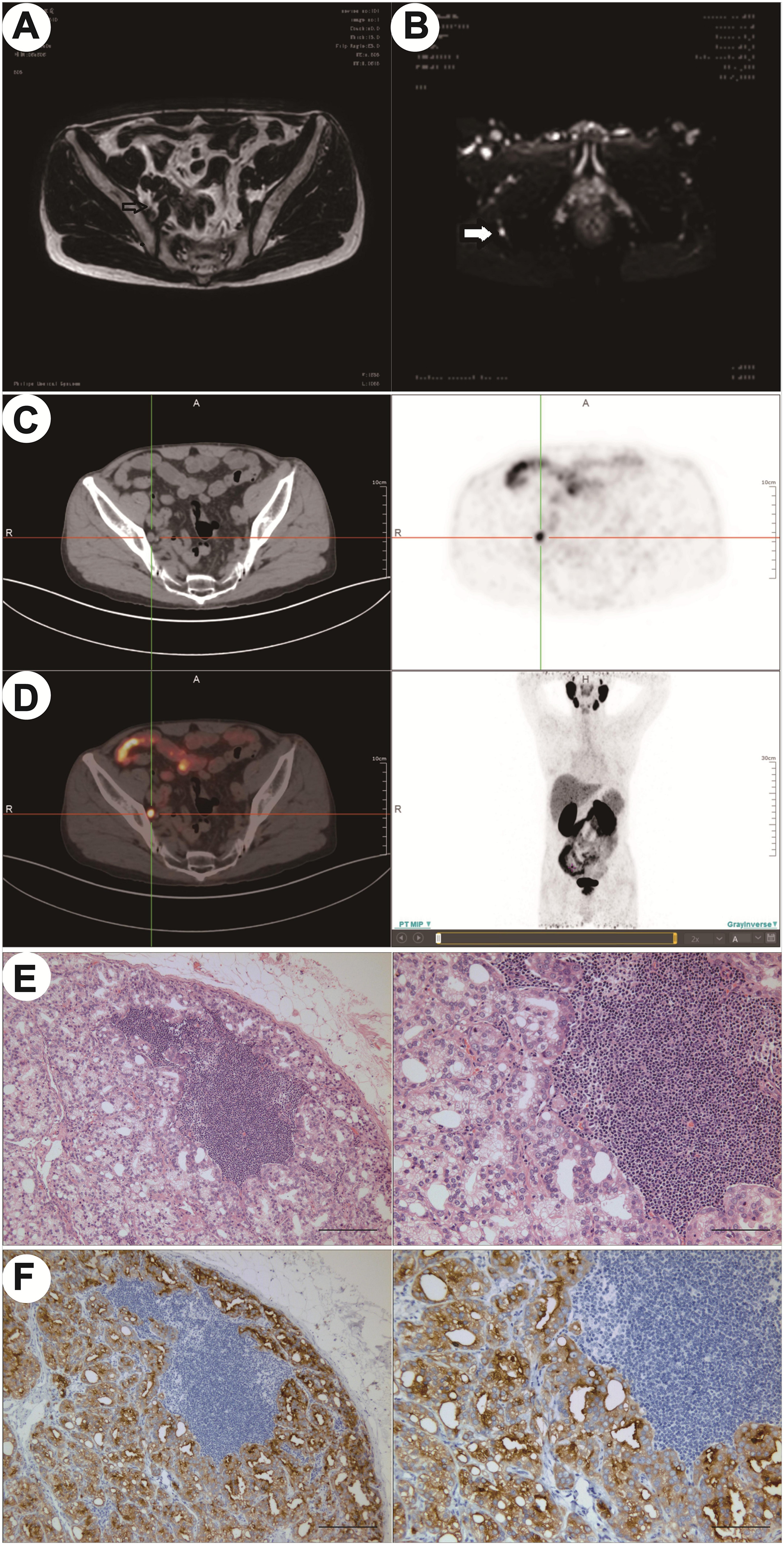
The performance of mpMRI and 68Ga-PSMA PET/CT in the PCa patient with lymph node metastases. (A) T2WI sequence of mpMRI; (B) DWI sequence of mpMRI; (C) CT; (D) 68Ga-PSMA PET/CT; (E) H&E staining; (F) PSMA immunohistochemistry. 68Ga-PSMA PET/CT: 68Gallium prostate-specific membrane antigen positron emission tomography/computed tomography; PCa: prostate cancer; mpMRI: multiparametric MRI; T2WI: T2-weighted imaging; DWI: diffusion-weighted imaging; H&E: hematoxylin-eosin.
Discussion
The accurate diagnosis and staging of PCa is of paramount importance and guides clinical decision-making in the choice between local treatment with systemic therapy, curative intent in palliative management or metastatic disease.2–4 68Ga-PSMA PET/CT and mpMRI, as non-invasive imaging modalities, are both well-established imaging examination for the investigation of PCa. 13 Pelvic invasion including seminal vesicle invasion, lymph nodes invasion, and so on, which needed more accuracy modalities for accurate diagnosis and treatment of PCa. Furthermore, new treatment paradigms such as PSMA-ligand endoradiotherapy, or image-guided radiotherapy place further demands on imaging modalities. 16 A study suggested that 68Ga-PSMA PET/CT-targeted biopsy demonstrated good accuracy in the diagnosis of clinically significant PCa, which was not inferior to mpMRI-targeted biopsy, improving the detection rate for cancer in systematic biopsy. 17 Another study showed that 68Ga-PSMA PET/CT with a SUVmax cut-off of 8 demonstrated a good accuracy in the diagnosis of clinically significant PCa showing a good cost-benefit ratio as a single procedure for the diagnosis and staging of high-risk PCa. 18 However, although highly promising of imaging technology and the hybrid PET/CT scanners become more widely available, the question of which modality and the false-negative rate should be performed and when remains urgent. With this point in view, there is a shortage of comparisons between 68Ga-PSMA PET/CT and mpMRI for the detection of pelvic invasion in the patients with PCa, with truly objective comparison obstructed by the heterogeneity of tracers, patient populations and protocols. The purpose of this study therefore is to further compare the diagnostic value and precise localization of 68Ga-PSMA PET/CT for preoperative pelvic invasion in PCa patients in comparison with mpMRI, to explore the better clinical diagnostic recommendations.
A total of 118 patients diagnosed with PCa, who underwent 68Ga-PSMA PET/CT and mpMRI at the same period, were included in this study by all collected and analyzed clinical data, from May 2019 to June 2024. Among them, the postoperative pathology of 46 patients, who underwent 68Ga-PSMA PET/CT and mpMRI before RP or RP + ePLND, showed the presence of pelvic invasion. In a retrospective study, Zhang et al. compared 68Ga-PSMA-11 PET/CT with mpMRI for preoperative lymph node staging in the patients with intermediate to high-risk PCa, noting both 68Ga-PSMA-11 PET/CT and mpMRI performed great value for the staging of lymph node. 19 Frumer M et al. suggested that 68Ga-PSMA PET/CT versus mpMRI for excluding regional metastases prior to RP also found that 68Ga-PSMA PET/CT and mpMRI had the similar performance in excluding pelvic LNI with NPV of approximately 90%. 20 The detection of 68Ga-PSMA PET/CT and mpMRI in each group was evaluated based on the lesion site of pelvic invasion, including seminal invasion, lymph node metastasis, and so on. A total of 46 PCa patients with pelvic invasion were studied separately and grouped. The results found that both 68Ga-PSMA PET/CT and mpMRI have high specificity and sensitivity in the detection of primary PCa with pelvic invasion, and it is in agreement with several previous studies.19,20
Lymph node staging is a vital element to determine first-rank management. 21 Therefore, preoperative accurate assessment of lymph node metastases is very important in the diagnosis of PCa. Conventional imaging, including CT or MRI, are commonly used for the evaluation of preoperative lymph node status. However, the lymph node status is largely underestimated with these traditional techniques. To date, PLND is considered the most accurate for assessment of lymph nodes metastases, as it provides fresh tissue for pathologic nodal analysis.22,23 However, this technique is invasive, which might result in the increased lymphocele/lymphedema rates and venous thromboembolism rates. 24 Previous studies found that Patients with percent positive cores>50% and Gleason grade 4–5 disease will benefit the most from PSMA PET/CT and also will benefit from therapeutic intensification strategies, which suggested that PSMA PET/CT is a suitable replacement for conventional imaging, providing superior accuracy, to the combined findings of CT and bone scanning in the staging of high-risk PCa, leading to a change in the therapeutic strategy in 10% of the cases.25–27 Therefore, the novel accurate and no invasive imaging techniques might be very important in selecting patients that were suitable for PLND with intermediate to high-risk PCa. Interestingly, our statistical analysis revealed that compared with mpMRI, 68Ga-PSMA PET/CT has more advantages in detecting micro-lymph node metastatic lesions with PCa, which might provide a new perspective for urologists to diagnose PCa.
There are limitations associated with this study. Firstly, this study is a retrospective study with a short period and geographical limitations, so the credibility of the research results needs to be further confirmed. Secondly, all the patients were diagnosed with PCa, the probability of pelvic invasion was high, and there was a certain selection bias, which might overestimate the diagnostic value of 68Ga-PSMA PET/CT and mpMRI. In addition, all the operations and reports of 68Ga-PSMA PET/CT and mpMRI were performed by experienced nuclear medicine and imaging doctors, and the results might not be directly applied to clinical application. Since 68Ga-PSMA PET/CT has introduced, only a few patients have undergone PET/CT and mpMRI examination in our hospital. Therefore, the large-scaled multi-center prospective clinical studies should be paid attention to performing to confirm these results.
Conclusion
In conclusion, the results in this study indicated that both 68Ga-PSMA PET/CT and mpMRI had high sensitivity and specificity for the diagnosis of pelvic invasion in patients with PCa. Despite the excellent performance of 68Ga-PSMA PET/CT in the diagnosis of small PCa lesions, it cannot replace the diagnostic value of mpMRI in localization and staging of PCa. However, further studies are needed to investigate the possible contribution of 68Ga-PSMA PET/CT for the detection of microcarcinoma and micrometastatic lesions of PCa patients.
Footnotes
List of abbreviations
Ethics,consent and permissions
The study was conducted in our hospital after approving by the institutional ethical committee of the Nanjing First Hospital, Nanjing Medical University. All patients included in the study signed an informed consent.
Author's contributions
JRP and QZQ contribute to Protocol/project development; PGJ and HW contributed to data collection or management; QZQ, XLW, and PGJ contributed to data analysis; QZQ, XLW, and HW contributed to manuscript writing/editing. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jiangsu Provincial Social Development Project (grant number BE2023661).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.