
Abstract
Objective
Simultaneous bilateral cochlear implantation has been shown to provide long-term benefits in children suffering from severe-to-profound hearing loss. However, very little research has been conducted on long-term benefits in Mandarin-speaking children. We aimed to (1) evaluate tone perception with simultaneous bilateral cochlear implants (CIs) compared to unilateral CIs; and (2) evaluate early auditory and speech skills.
Methods
The longitudinal study was comprised of 20 participants, 10 with unilateral and 10 with simultaneous bilateral CIs. Participants received a CI at a mean age of 1.3 (SD ± 0.2) years. The Mandarin Early Speech Perception test, auditory thresholds, and influence of environmental factors were measured pre-operatively and after 24 months. Categories of Auditory Performance (CAP), Speech Intelligibility Rating (SIR), and LittlEARS Auditory Questionnaire (LEAQ) were measured pre-operatively and after 6, 12, and 24 months.
Results
After 24 months of device use, tone perception scores tended to be higher in the bilateral CI group than in the unilateral group, although the difference did not reach statistical significance (p = 0.058). Over the 24-month follow-up period, CAP, SIR, and LEAQ scores showed significant improvements in both groups (all p < 0.05).
Conclusions
Tone perception and early auditory and speech skills in Mandarin-speaking children were better with simultaneous bilateral CI implantation compared to unilateral after 24 months of use.
Introduction
Treatment with a cochlear implant (CI) has become increasingly common in young children with severe-to-profound hearing loss, showing great benefits in both speech and language development. Recent studies have shown the vast improvements that children have gained after receiving simultaneous bilateral CIs.1–5 These include benefits to speech recognition in quiet and in noise, to sound localization, and to spoken language abilities.1–5 Moreover, with language development and hearing performance, the age at implantation is critically important.6,7 Our recent publication from Gao and colleagues demonstrated that in the short term (i.e. 12 months post-first fitting (FF)), bilateral implantation had profound significant improvements in both speech and hearing performance in Mandarin-speaking young children. 5
Mandarin is a tonal language that uses pitch cues to provide lexical meaning. 6 Therefore, it is critical to perceive tonal distinctions to understand spoken Mandarin. The tone information in Mandarin is widely distributed among various frequency components of syllables. The fundamental frequency (F0) and its harmonics carry the main tone information, and the perception of tones mainly relies on F0. Limited by the coarse spectral resolution of CIs, users cannot fully utilize F0 information, and as such usually have weaker tone discrimination ability.8–13 Previous studies have shown that the recognition rate of Mandarin tones among unilateral CI users ranges from 60% to 82%,8–13 with large individual differences in tone recognition performance. Tone information also plays an important role in speech understanding in noise and in music perception. It contributes to improved speech recognition in noisy environments,8,14 and is significantly correlated with the ability to appreciate music, in terms of tone recognition, melody perception, and instrument identification. 15 Therefore, many scholars are currently devoted to the study of tone perception in CI users.
In addition to the limitations of the CI itself, the perception of tones is influenced by other factors. Zhou and Xu conducted a study on tone perception and production abilities in 125 unilateral CI children (2.42–16.18 years old) and analyzed the effects of variables such as age at implantation, duration of CI use, family members and income, CI type and speech processing strategies, communication mode, and rehabilitation time on tone perception. 13 The results showed that age at implantation was the only factor that influenced Mandarin Chinese tone perception, with early cochlear implantation leading to better tone perception and production abilities. 13 However, Chen and Xi found that the average tone recognition score for 96 unilateral CI children (2.41–7.09 years old) was 77%, and there was a significant correlation between the duration of CI use and tone perception scores. 8 However, these results were only obtained from unilateral CI recipients, and limited research exists on tone perception abilities in bilateral CI children.
The purpose of this study is to explore the perception of Mandarin tones in a homogeneous group of early bilateral simultaneous CI patients (who were the same age at implantation and testing) and to compare them with unilateral cochlear-implanted children. Furthermore, we aim to analyze the factors (parent education level, living environment, residual hearing before implantation, pre-operative hearing aid use, post-operative rehabilitation, and only child status) that may affect the tone perception abilities of bilateral CI children under the conditions of consistent age at implantation and testing.
Methods
This study employed a prospective design to compare Mandarin tone perception between children with unilateral and simultaneous bilateral cochlear implantation, conducted from January 2017 to November 2019. The STROBE guidelines were followed when reporting this study.
Subjects
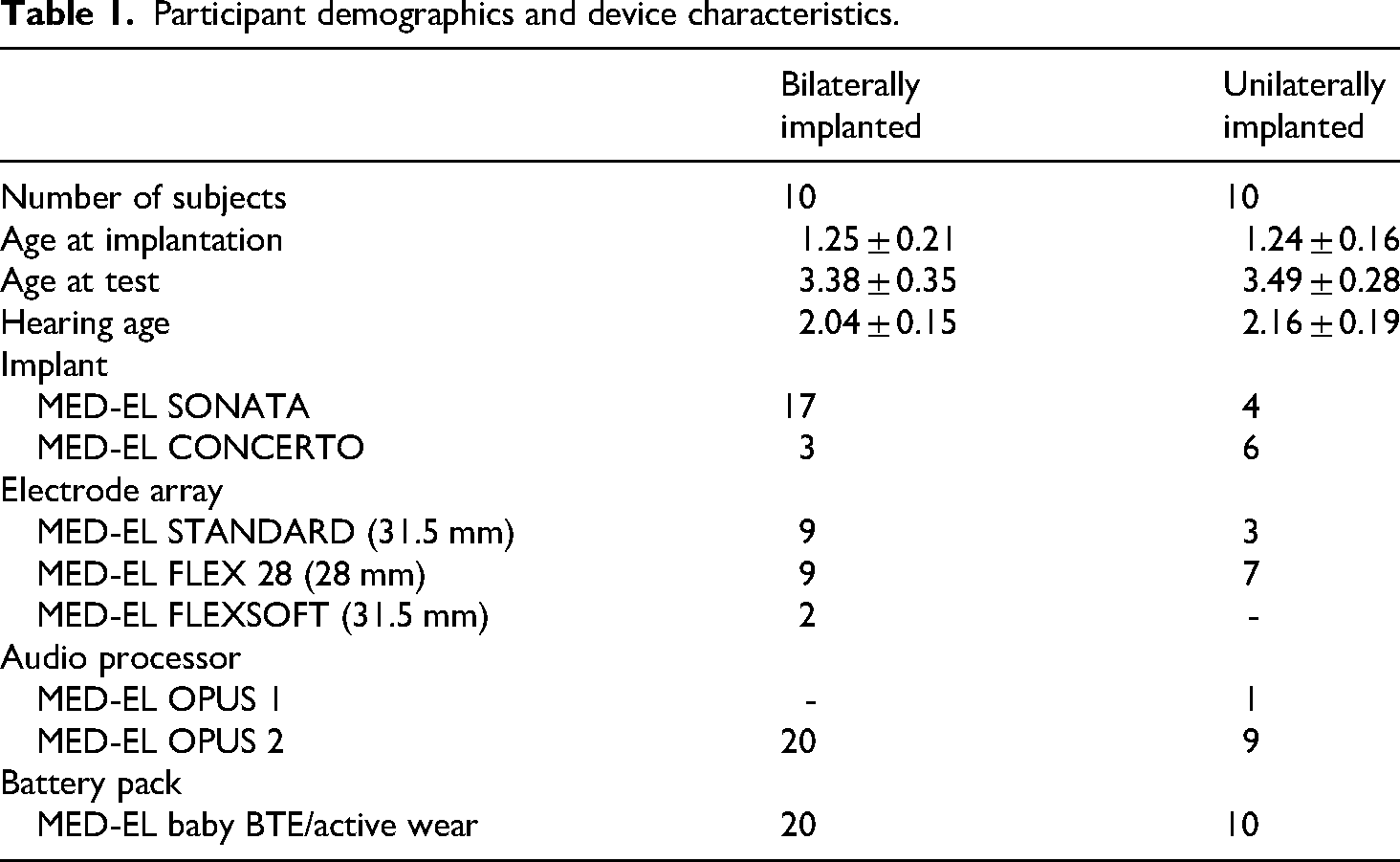
Twenty children with congenital bilateral severe-to-profound hearing loss were recruited at the Peking Union Medical College Hospital in Beijing, China. Ten participants were unilaterally implanted, and 10 participants were simultaneously bilaterally implanted. The unilateral group consisted of four males and six females with a mean age of 1.24 (±0.16) years at the time of implantation. The bilateral group consisted of four females and six males with a mean age of 1.25 (±0.21) years at the time of implantation. As per clinical norm, prior to CI provision, most participants did not use hearing aids. All participants received MED-EL implants and electrode arrays (MED-EL GmbH, Innsbruck, Austria; Table 1). All surgeries were performed via round window insertion and using soft surgical techniques. This study was completed in accordance with the Helsinki Declaration of 1975 as revised in 2024. The study protocol was approved by the Ethics Committee of Peking Union Medical College Hospital (ZS-1028; November 29, 2016), and written informed consent was obtained from the parents of all minor participants prior to study enrollment.
Participant demographics and device characteristics.
Test batteries
Measurements for tone perception, pre-operative residual hearing, post-operative aided hearing thresholds, and the influence of environmental factors were completed pre-operatively and after 24 months post-FF. The Categories of Auditory Performance (CAP), Speech Intelligibility Rating (SIR), and LittlEARS Auditory Questionnaire (LEAQ) tests were completed pre-operatively and after 6-, 12-, and 24 months post-FF.
Tone perception assessed with the Mandarin Early Speech Perception test
Mandarin Early Speech Perception (MESP) test was used to assess early tone perception in Mandarin-speaking children with CIs. MESP is a closed set two alternative tone pair discrimination test based on the English Early Speech Perception test developed by Moog and colleagues. 16 This test consists of six categories of increasing difficulty, in which category six is used to test tone perception. Four tones make up six tone pairs of increasing difficulty. The first three categories are similar to the English version (category 1: speech detection; category 2: pattern perception; category 3: spondee perception). The last three categories focus on tonal differences that exist within the Mandarin language (category 4: vowel perception; category 5: consonant perception; category 6: tone perception). 17 The test items were presented at 65 dB (A) through loudspeakers from a computer and the participants pointed to pictures after hearing each recorded word. In the picture, there are two objects that sound the same but have different tones, and the child chooses one of the two objects based on what they had heard. A more comprehensive description of MESP methods is described by Zheng and colleagues (2010). 17
Influence of hearing level on tone perception
Pre-operative residual hearing was assessed using the response thresholds of tone-burst auditory brainstem response (500/1000/2000/4000 Hz) recorded by the Biologic Navigator Pro objective auditory test system (Natus Europe GmbH, München, Germany). The test was performed in an electromagnetically shielded soundproof booth with a background noise of <30 dB (A) sound pressure level.
Aided hearing thresholds were measured using a Madsen Conera audiometer (GN Otometrics A/S, Taastrup, Denmark) in a standard soundproof booth, where background noise was <30 dB (A). Warble tones (500/1000/2000/4000 Hz) were presented through a loudspeaker 1 m away at 0-degree azimuth in the sound field. Aided hearing thresholds for children at 24 months post-cochlear implantation can be obtained through play audiometry.
Influence of potential environmental factors on tone perception
We examined the potential effects of environmental variables such as parental education level, only child status, living conditions, unaided auditory thresholds before operation, history of hearing aid use before operation, and history of auditory rehabilitation after operation, on MESP tone perception. The family environment can have a substantial impact on a child's hearing and speech development after receiving a CI, as reviewed by Davenport and Holt. 18 In a separate analysis we calculated the averages of the MESP tone perception scores while factoring in the potential environmental variables. Information was gathered via questionnaires given to the child's parents/guardians.
Evaluation of the early auditory and speech skills in the implanted children
Categories of auditory performance
The CAP test is an index consisting of eight performance categories relating to auditory perception. 19 It is arranged in a hierarchy of skills that increase in difficulty from the ability to hear environmental sounds to the ability to use a telephone. The CAP is widely used for monitoring the progress of a child with a CI.
Speech intelligibility rating
The SIR test is used to document a child's speech intelligibility over time by allocating their ability to speak into categories between 1 and 5, whereby category 1 refers to having no intelligible speech, category 2 refers to the production of single words, and higher categories are assigned to increasing levels of speech intelligibility and connection of words. 20
LittlEARS auditory questionnaire
LEAQ is a questionnaire that evaluates age-appropriate auditory behavior in the pre-verbal development phase based on the parents/guardians’ observations of their child's reaction to acoustic stimuli. 21 This questionnaire consists of a series of yes/no questions and was validated for use in Mandarin. 21 It takes approximately 10 min for the parents/guardians to complete, and the results obtained can be compared to a set of expected values.
Statistical methods
All analyses were performed using IBM SPSS Statistics 24 (IBM, Armonk, NY). All figures were created using Office Excel (Microsoft, Redmond, WA). Data are presented as the means with standard deviations (±SD) and/or the medians with ranges (minimum and maximum values). Qualitative data are presented as absolute and relative frequencies, and are used to describe participant characteristics (e.g. age, gender, etc.) and characteristics of the examined study outcomes. Data normality was confirmed using the Shapiro–Wilk tests. For data followed a normal distribution, we used the analysis of variance (ANOVA) and paired t-tests. For data that did not follow a normal distribution, we used the Friedman test and Wilcoxon rank test. All multiple pairwise comparisons were corrected using the Bonferroni method, to avoid any type I errors. Degrees of freedom are reported as F (between groups, within groups) followed by the F-value. Statistical significance was set to p < 0.05.
Tone perception assessed with MESP test
Mann–Whitney U tests were used to examine differences between bilateral and unilateral CI groups for each given tone at 24 months post-FF (tone average, tone 1, tone 2, tone 3, and tone 4).
We used a Friedman test to assess the differences of the four tones (tones 1 to 4), independently within each bilateral and unilateral CI group.
Influence of hearing level on tone perception
To examine if pre-operative residual hearing versus post-FF aided hearing thresholds influenced tone perception, we used a univariate ANOVA with degrees of freedom expressed as F. Univariate ANOVA analyses took place between hearing thresholds and tone perception in both bilateral and unilateral groups at pre-operation and 24 months post-FF.
Influence of environmental factors on tone perception
A repeated measures ANOVA was used to assess the effect of variables such as education level of parents, only child status, living environment, pre-operation unaided auditory threshold, pre-operation history of hearing aid use, and history of auditory rehabilitation post-FF, on tone perception.
Evaluation of the early auditory and speech skills with the CAP, the SIR, and the LEAQ
A Friedman test was used to determine if there was any improvement over time at 6-month intervals (from pre-operative testing up to 24 months post), separately within the bilateral and unilateral CI groups for each test. Pairwise comparisons with the Wilcoxon signed-rank test were performed to assess differences between the individual post-FF test results.
Results
Tone perception assessed with the MESP test
Tone perception assessed with the MESP scores are presented in Figure 1. We found that, although not significant, the average tone score was better in the bilateral CI group compared to the unilateral CI group (u = 25.000, p = 0.058). Similarly, for the recognition scores of tones 1 to 4, the bilateral CI group also showed higher results than the unilateral CI group, though again, without statistical significance (tone 1: u = 28.000, p = 0.083; tone 2: u = 37.000, p = 0.319; tone 3: u = 43.000, p = 0.588; tone 4: u = 25.000, p = 0.053). Overall, we did not find any significant differences between the four Mandarin tones, either in the bilateral group or in the unilateral group (Friedman test: bilateral group: χ2 = 6.209, p = 0.102; unilateral group: χ2 = 6.253, p = 0.100).

Tone perception results (tone average, tones 1 to 4) assessed with the Mandarin Early Speech Perception (MESP) test at 24 months post-operatively are shown for the bilateral and unilateral group (%). The black squares indicate the mean, the horizontal lines the median. The asterisks depict outliers, the circles extreme outliers.
Influence of hearing level on tone perception
The influences of hearing level on tone perception are presented in Tables 2 and 3. No significant effects of pre-operative residual hearing or 24 months post-operative hearing thresholds on tone perception were found for either bilateral or unilateral implanted children (Tables 2 and 3).
Hearing level in both bilateral and unilateral groups pre-operatively and 24 months post-first-fitting.

Pre, pre-operatively; 24m: 24 months post-first fitting. ; nHL: normalized Hearing Level.
Residual hearing: the average hearing level from 500 to 4000 Hz (if no response was obtained at a frequency, a value of 130 dB nHL was applied in the calculation 22 ). Aided hearing threshold: the average hearing threshold from 500 to 4000 Hz.
Influence of hearing level on tone perception.

24m post-FF: 24 months post-first-fitting.
Statistical values are reported as degrees of freedom (df), F-values, and p-values.
Influence of environmental factors on tone perception
The influence of potential factors on tone perception is presented in Table 4. No significant effects on tone perception were found for any of the evaluated variables.
Influence of potential environmental factors on tone perception 24 months post-first fitting.

MESP: Mandarin Early Speech Perception; 24m: 24 months.
Statistical values are reported as degrees of freedom (df), F-values, and p-values.
Evaluation of the early auditory and speech skills in the implanted children
Categories of auditory performance
Mean CAP scores improved significantly from the pre-operative testing up to 24 months post-FF for both groups (Friedman test: statistic: bilateral group: χ2 = 28.2, p < 0.001; unilateral group: χ2 = 12.6, p = 0.006). When separately comparing all the post-FF time intervals, we found significant results within the bilateral group at all time interval comparisons, however not within the unilateral group (Tables 5 and 6).
Early auditory and speech performance scores of the implanted children assessed with the CAP, SIR, and LEAQ questionnaires.

CAP: Categories of Auditory Performance; SIR: Speech Intelligibility Rating; LEAQ: LittlEARS Auditory Questionnaire; 6m: 6 months; 12m: 12 months; 24m: 24 months.
Statistical comparison of early auditory and speech skill scores across time points in implanted children.

CAP: Categories of Auditory Performance; SIR: Speech Intelligibility Rating; LEAQ: LittlEARS Auditory Questionnaire; 6m: 6 months; 12m: 12 months; 24m: 24 months.
p value threshold is 0.05/3 = 0.017 (Bonferroni corrected).
Speech intelligibility rating
Mean SIR scores improved significantly from pre-operative testing up to 24 months post-FF for both groups (Friedman test: statistic: bilateral group: χ2 = 29.2, p < 0.001; unilateral group: χ2 = 13.9, p = 0.006). When separately comparing all the post-FF time intervals, we found significant results within the bilateral group at all intervals comparisons except 24 months versus 12 months, however not within the unilateral group (Tables 5 and 6).
LittlEARS auditory questionnaire
The mean LEAQ score was significantly increased from pre-operative testing up to 24 months post-FF for both groups (Friedman test: statistic: bilateral group: χ2 = 28.2, p < 0.001; unilateral group: χ2 = 14, p = 0.003). When separately comparing all the post-FF time intervals, we found a significant result within the bilateral group at all time intervals except 24 months versus 12 months. No significant differences were found when comparing the post-FF time intervals within the unilateral group (Tables 5 and 6).
Discussion
The main findings of this investigation were that: (1) the overall tone perception ability in Mandarin-speaking children was better, albeit not significantly, with simultaneous bilateral CI compared to unilateral CI after 24 months post-FF; (2) the potential environmental variables had no effect on tone perception scores after 24 months post-FF; and (3) when the two groups were analyzed separately, we found that the CAP, SIR, and LEAQ scores were significantly increased at all time intervals (except for 24 months vs. 12 months) in the bilateral group but not in the unilateral group.
In this study, the average recognition rate of tone perception in bilateral CI recipients was 89% (Figure 1), which was higher compared to unilateral CI recipients (81%) and previous studies.8–13 This may be due to several reasons. First, the subjects in this study had a young age at implantation (1.25 ± 0.21 years) and high homogeneity. The age at implantation may be an important factor influencing tone perception in CI children. Han et al. 9 conducted a study on tone perception in 20 prelingually deaf children (1.5–13.5 years old) who received CIs and found a correlation between early implantation and better tone perception. Moreover, a study from Zhou and Xu showed that the age at implantation was the only influential factor on tone perception and production abilities in 125 Mandarin-speaking unilateral CI children (2.42–16.18 years old). 13 Both bilateral and unilateral CI children in this study were younger at the time of implantation compared to these previous studies, which may have contributed to higher tone perception scores found here. Second, binaural listening provides redundant information in terms of temporal and intensity cues, enhancing the perception of the target signal. In the perception of Mandarin tones, the perception and extraction of F0 is crucial. When F0 is present, other acoustic cues such as duration and intensity play a secondary role. However, when F0 extraction is difficult, duration and intensity may serve as important cues for tone perception. Because of limited F0 cues, CI users may rely on duration and amplitude envelope cues to recognize Mandarin tones.23,24 Bilateral CI recipients can obtain more redundant information in terms of duration and intensity, which may contribute more to the perception of speech and tones.
Previous studies have focused on the influence of the age at implantation and the duration of CI use on tone perception. However, there are also other potential factors that may influence speech tone recognition in these children, including family support, socioeconomic status, maternal influence, family structure, and so on. Families from higher socioeconomic backgrounds are more likely to have access to early cochlear implantation and post-operative rehabilitation, which positively impacts later auditory and speech abilities. Zhou and Xu conducted a study on tone perception and production abilities in 125 unilateral CI children and analyzed the effects of variables such as age at implantation, duration of CI use, family members and income, CI type and speech processing strategies, communication mode, and rehabilitation time on tone perception. 13 The results from this study showed that the age at implantation was the sole factor influencing Mandarin tone perception. 13 However, in contradiction, Chen and Xi conducted a study on 96 unilateral CI children and analyzed the effects of variables such as the age at implantation, the duration of CI use, previous hearing aid use, maternal education level, and pre-operative hearing level on Chinese tone and sentence perception. 8 The study demonstrated that only the duration of CI use could predict tone perception ability in quiet environments. 8 Long et al. found that having caregivers with higher education levels was positively correlated with early development of pre-lingual auditory skills in CI children. 25 Further, children with better pre-operative hearing thresholds had better pre-lingual auditory skills after surgery. 25 Because the subjects in this study had high homogeneity in terms of the age at implantation and the duration of CI use, attempts were made to analyze whether factors such as parents’ education level, living environment, residual hearing before implantation, pre-operative hearing aid use, post-operative rehabilitation, and whether the child is the only child may have an influence on early speech and tone perception. The results showed no significant correlations between tone perception and these factors. The results of this study, including previous research, are not entirely consistent, and one possible reason is the relatively small sample size in the studies. More studies are needed using a homogeneous population with a larger sample size.
The current investigation used CAP, SIR, and LEAQ questionnaires to evaluate the children's early auditory and speech skills after implantation, and both the combined and separate differences between bilateral and unilateral CI groups. We found that, when separating the bilateral and unilateral groups, the bilateral group had significantly higher scores in the CAP, SIR, and LEAQ at all time intervals, which has been similarly demonstrated in previous studies. Indeed, an investigation from Long et al. showed that bilateral implantation resulted in a significant improvement in the Mandarin version of the LEAQ compared to unilateral implantation, with the improvements lasting 24 months post-FF. 25 As previously mentioned in the Methods, the LEAQ evaluates age-appropriate auditory behavior in the pre-verbal development phase which is based on the parents/guardians’ observations of their child's reaction to acoustic stimuli. 21 This evaluation is not necessarily an objective measure of a child's speech and hearing performance, but rather a subjective observation. Gao et al. speculated that a major reason for the lack of difference between bilateral and unilateral implantations was due to the short timeframe at which the children were tested after receiving the CI. 5 Indeed, based on previous investigations, it is quite clear that long-term bilateral CI use offers much greater significant benefits in both speech and hearing performance compared to just short-term CI use.26–30 Ultimately, these findings demonstrate that, within Mandarin-speaking children, CI use improves the scores of the CAP, SIR, and LEAQ over the long term.
This study has several limitations. First, the sample size of this study was relatively small. Future studies with larger cohorts are necessary to validate our preliminary findings, enhance the generalizability of the results, and allow for more sophisticated sub-group analyses. Second, our follow-up period was relatively short. As the children grow older and their ability to cooperate improves, future studies should incorporate more assessments of tone perception, language, and cognitive skills. This may reveal more pronounced differences in auditory and speech development between unilaterally and bilaterally implanted children.
Conclusion
This investigation found that Mandarin-speaking children had a better, albeit not-significant, tone perception ability at 24 months post-FF when implanted with simultaneous bilateral CI compared to only being implanted unilaterally. Moreover, simultaneous bilateral CI demonstrated significantly higher scores in the CAP, SIR, and LEAQ up to 24 months post-FF compared to being implanted unilaterally. The use of simultaneous bilateral CI implantation in Mandarin-speaking children can offer improvements that are not seen when the child is unilaterally implanted. We would recommend bilateral implantation for further clinical practice in Mandarin-speaking children suffering from severe-to-profound bilateral hearing loss.
Footnotes
Abbreviations
Ethical considerations and consent to participate
The study was approved by the Ethics Review Committee of Beijing Union Medical College Hospital (Protocol ZS-1028). For all minor participants, written informed consent was provided by their parents before enrollment.
Author contributions
Conceptualization, Zhiqiang Gao; methodology, Zhiqiang Gao, Hua Yang, Yingying Shang, Bin Wang, and Xu Tian; data curation, Suju Wang, Bingya Guo, Jiayan Yang, Wen Sun, Jianglan Zuo, and Yanan Lan; writing—original draft preparation, Suju Wang; writing—review and editing, Suju Wang and Zhiqiang Gao; supervision, Zhiqiang Gao and Xu Tian; and funding acquisition, Zhiqiang Gao. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China, National High Level Hospital Clinical Research Funding (grant numbers 2022YFC2402701, 2019YFB311801, and 2022-PUMCH-B-095).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors on request.