
Abstract
Primary intestinal-type adenocarcinoma (ITAC) of the larynx is extremely rare and requires differentiation from metastatic intestinal adenocarcinoma due to their similar morphological and immunophenotypic features. This case report describes a man in his early 70s presenting with 3 months of hoarseness, with a history of well-controlled coronary heart disease and hypertension. Laryngoscopy revealed nodular masses in the anterior part of the left ventricular fold and epiglottic tubercle, while neck ultrasound demonstrated no significantly enlarged lymph nodes. The patient underwent extended resection of the mass via transoral CO2 laser microsurgery, with negative surgical margins. Postoperative pathology combined with immunohistochemistry (CK7 -, CK20 +, CDX2 +, SATB2 +, Villin +) confirmed the diagnosis. Gastrointestinal endoscopy ruled out metastatic lesions, and whole-body PET/CT showed no abnormal involvement. No tumor recurrence was observed during 12 months of follow up. This case emphasizes the importance of pathology, gastrointestinal endoscopy, and imaging in differentiating primary from metastatic lesions in laryngeal adenocarcinoma with intestinal differentiation. Surgical resection is the preferred treatment for early localized lesions, and additional long-term follow-up data are required to clarify the prognosis.
Keywords
Introduction
Laryngeal adenocarcinoma is a rare malignancy, accounting for approximately 1% of all laryngeal cancers. It mainly arises from the laryngeal salivary glands or serous glands; however, most cases are metastatic adenocarcinomas. 1 Laryngeal intestinal-type adenocarcinoma (ITAC) is an extremely rare subtype that exhibits morphological similarity to intestinal adenocarcinoma and shares an identical immunophenotype as colorectal cancer. Therefore, metastasis from gastrointestinal adenocarcinoma should be excluded before diagnosing primary laryngeal ITAC. Diana Bell et al. 2 first reported a case in 2014, and no other English-language literature reports have been identified. This study retrospectively analyzed the clinical data of a case of primary laryngeal ITAC and reviewed relevant literature to investigate its clinical manifestations, pathological features, treatment strategies, and prognosis.
Case presentation
A man in his early 70s presented to The Second Affiliated Hospital, School of Medicine, Zhejiang University (Hangzhou, China) in mid-2024 with a 3-month history of hoarseness. He had a history of coronary heart disease and hypertension, both of which were well-controlled. Laryngoscopy revealed nodular masses in the anterior part of the left ventricular fold and epiglottic tubercle, with normal mobility of the bilateral vocal cords (Figure 1(A)). Neck lymph node ultrasound revealed no significantly enlarged lymph nodes on either side of the neck. After excluding surgical contraindications, transoral laryngeal mass biopsy was performed under general anesthesia. Intraoperatively, nodular masses were observed in the epiglottic tubercle, anterior parts of the bilateral ventricular folds, and the inferior edge of the left ventricular fold, with a slightly rough and granular surface. Intraoperative frozen section suggested: (laryngeal mass) glandular tissue showing tubular and papillary patterns, with low-grade intraepithelial neoplasia and small foci of cribriform pattern, consistent with high-grade intraepithelial neoplasia. Therefore, with the patient's family's consent, extended mass resection was performed via transoral CO₂ laser microsurgery. The resection encompassed the anterior aspects of the bilateral ventricular folds, epiglottic tubercle, and tissue above the anterior commissure, with a 2mm safe margin (Figure 2(A)). Intraoperative frozen section analysis confirmed negative surgical margins.
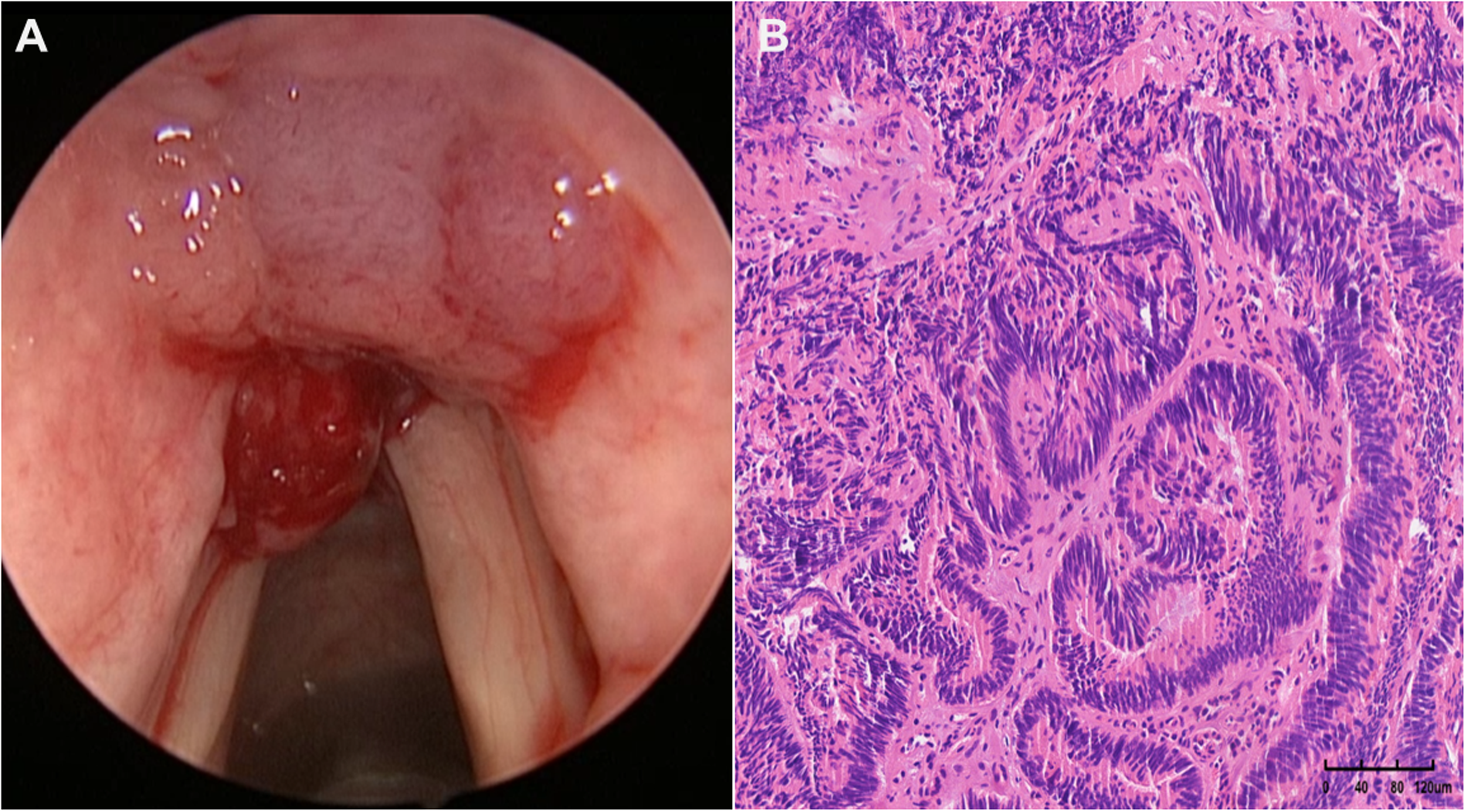
Laryngoscopy revealed nodular masses in the anterior part of the left ventricular fold and epiglottic tubercle (A). Postoperative routine pathology indicated low-grade intraepithelial neoplasia and well-differentiated adenocarcinoma (B).

Postoperative laryngoscopy at 20 days (A). At 12 months postoperatively, follow-up laryngoscopy (B) and MRI (C and D) revealed no obvious tumor recurrence. MRI: magnetic resonance imaging.
Postoperative routine pathology (Figure 1(B)) indicated: (epiglottic tubercle mass) glandular tissue showing tubular and papillary patterns, with low-grade intraepithelial neoplasia and well-differentiated adenocarcinoma, consistent with ITAC based on immunohistochemical findings. Immunohistochemistry results: CK7 (−), CK20 (+), CDX2 (+), SATB2 (+), Villin (+), p16 (−), TTF-1 (SPT24) (−). The immunohistochemical results have been reviewed by two pathologists. No lesions were detected on postoperative gastrointestinal endoscopy. Whole-body positron emission tomography/computed tomography (PET/CT) imaging showed: (1) clinically suspected postlaryngeal cancer surgery changes, with slightly increased glucose metabolism in the surgical area, consistent with postoperative alterations and (2) physiological radioactive uptake in the intestinal tract. Postoperative diagnosis: laryngeal cancer (ITAC, supraglottic type, T2N0M0). To date, the patient has been followed up for 12 months, and no obvious tumor recurrence has been identified on laryngoscopy and magnetic resonance imaging (MRI; Figure 2(B)–(D)).
All patient details have been de-identified. This study was reported in accordance with the CARE guidelines. 3
Discussion
Primary laryngeal adenocarcinoma is uncommon, accounting for approximately 1% of nonsquamous cell laryngeal malignancies, and generally originates from salivary glands or serous glands. 1 ITAC is an even rarer type of primary head and neck malignant tumor. Most literature reports document its occurrence in the nasal cavity and paranasal sinuses, with only a few cases reported in the tongue, base of the tongue, middle ear, and pharynx.4–7 For primary laryngeal ITAC, only one case reported by Diana Bell et al. 2 in 2014 was found in literature search. Due to the rarity of primary head and neck ITAC, current basic research is mostly based on sinonasal ITAC.
Microscopically, primary ITAC is characterized by columnar cells arranged in glandular or papillary structures similar to colorectal cancer, and some cases contain mucinous components, signet-ring cells, or poorly differentiated cancer components.2,6 ITAC not only has a microscopic structure similar to colorectal cancer histologically but also has similar characteristic immunohistochemical markers. Literature reports indicate that commonly used immunohistochemical indicators include CDX2, CK20, Villin, CK7, and SATB2,8,9 which assist in distinguishing ITAC from other primary laryngeal adenocarcinomas. CK7 is diffusely and strongly positive in intestinal adenocarcinoma but weakly expressed or absent in ITAC 10 ; compared with CDX2, CK20 shows specific positive expression in ITAC, and positive SATB-2 expression further supports the diagnosis of ITAC. 9 The patient in this case was negative for CK7, while CDX2, CK20, and SATB2 were positive, showing characteristics of intestinal-derived tumors. Although immunohistochemical studies indicate that ITAC and rectal adenocarcinoma are highly similar, significant differences exist in their molecular pathological mechanisms. 11 Activating mutations of KRAS and BRAF oncogenes in the epidermal growth factor receptor (EGFR) signaling pathway are common in rectal adenocarcinoma but much less frequent in ITAC. 12 In ITAC, MET (MET proto-oncogene, receptor tyrosine kinase) protein overexpression can be observed but without MET gene amplification, which is not common in rectal adenocarcinoma, providing a possible opportunity for targeted therapy. 13
Metastatic laryngeal malignant tumors are rare, accounting for approximately 0.09% to 0.40% of laryngeal tumors, mostly including cutaneous melanoma and renal cell carcinoma; among these metastatic laryngeal cancers, laryngeal metastasis from primary intestinal cancer accounts for approximately 6%.14,15 Although laryngeal metastasis from intestinal cancer is rare, gastrointestinal endoscopy must be performed to distinguish it from gastrointestinal malignant tumors metastases to the larynx. Gastrointestinal endoscopy is recommended for all cases where intestinal-type differentiation is detected in laryngeal cancer after simple mass resection or radical surgery. Primary laryngeal ITAC can be diagnosed after excluding metastasis from primary gastrointestinal lesions. Since gastrointestinal endoscopy is not a routine assessment method for the initial diagnosis of laryngeal cancer, the patient in this case underwent gastrointestinal endoscopy after the postoperative routine pathological examination suggested ITAC, excluding distant metastasis from gastrointestinal malignant tumors, and was subsequently diagnosed with primary laryngeal ITAC. For the confirmation of primary laryngeal ITAC, pathologically, immunohistochemical markers including CDX2, CK20, Villin, CK7, and SATB2 can be used to differentiate it from other primary laryngeal adenocarcinomas. Clinically, gastrointestinal endoscopy is required to rule out metastases from primary gastrointestinal lesions; to avoid missing subtle lesions, concurrent whole-body PET/CT can be performed.
Due to the extreme rarity of primary laryngeal ITAC, literature reports are limited to case reports, and there is currently no standard treatment regimen. Diana Bell et al. 2 reported a case with a TNM (tumor, node, metastasis) stage of T3N2cM0 at diagnosis: the patient showed no significant response to four cycles of induction chemotherapy, then underwent total laryngectomy and bilateral neck dissection of levels II to IV, followed by postoperative radiotherapy (a total dose of 67.4 Gy delivered in 33 fractions); no recurrence or metastasis was observed during 6 months of follow up. In the present case, the tumor was staged as T2N0M0. Given the localized nature of the lesion, the patient underwent transoral endoscopic CO₂ laser tumor resection, with negative surgical margins. Postoperative PET/CT imaging indicated no involvement of cervical lymph nodes or other sites; no radiotherapy or chemotherapy was administered postoperatively, and no tumor recurrence or metastasis has been noted during 12 months of follow up to date. Compared with open or combined surgical approaches, transoral endoscopic CO₂ laser resection is more suitable for early-stage localized laryngeal ITAC, particularly demonstrating more distinct advantages in the preservation of vocal and swallowing functions.
Nonsquamous cell carcinoma of the larynx encompasses multiple pathological subtypes, and the radiosensitivity of these tumors and their response to systemic therapy are unpredictable. However, Andrea Iandelli et al. 16 demonstrated that the general surgical principles for laryngeal cancer remain applicable to this subtype. Surgical approaches should be tailored to tumor stage and patient conditions. 17 For patients with early-stage, localized lesions, surgery is the first choice, and minimally invasive methods are recommended to completely resect the tumor. During surgery, oncological principles should be followed to ensure negative margins. 16 Radiotherapy can be used as a treatment option for advanced tumors or patients ineligible for surgery due to lesion location and age. It can also be used as adjuvant postoperative treatment for patients with high-risk factors for recurrence (e.g. positive margins) and can be combined with platinum-based drugs for concurrent chemoradiation sensitization. 11 The role of chemotherapy alone in the treatment of laryngeal ITAC is currently uncertain. Most immunotherapies for ITAC remain theoretical, with no clinical data available.
Due to the rarity of nonsquamous cell carcinomas of the larynx, their prognosis has not been fully elucidated. 18 According to literature reports, laryngeal adenocarcinomas (e.g. laryngeal adenocarcinoma not otherwise specified, adenoid cystic carcinoma, and mucinous adenocarcinoma) have a poorer prognosis compared with laryngeal squamous cell carcinoma at the same stage.19,20 The patient in this case has only been followed up for 12 months, and additional long-term follow-up data are still needed to clarify the prognosis.
Conclusion
In conclusion, primary laryngeal ITAC is extremely rare. When postoperative pathology suggests ITAC, clinical differentiation from metastatic gastrointestinal adenocarcinoma is required using modalities such as gastrointestinal endoscopy and PET/CT. Individualized treatment should be emphasized, with surgical treatment as the primary modality for early-stage, localized lesions. The insufficient follow-up duration is a limitation of this prognostic analysis; therefore, additional long-term follow-up data are still required to elucidate the prognosis.
Footnotes
Acknowledgements
The authors thank all the members of Department of Otorhinolaryngology—Head and Neck Surgery, the Second Affiliated Hospital, School of Medicine, Zhejiang University, for their invaluable help.
Ethical considerations
The study was approved by the Ethics Committee of the Second Affiliated Hospital, School of Medicine, Zhejiang University (approval no.: 2025LSYD1113. 29 July 2025).
Author contributions/CRediT
MHN did resources, visualization, and writing—original draft and editing. LXX did conceptualization, resources, supervision, methodology, project administration, and editing. ZD and LZW did conceptualization, supervision, funding acquisition, writing-original draft, and writing—review and editing.
Statement of informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work is supported by the Medical Science and Technology Project of Zhejiang Province (number: 2023KY737) and the National Natural Science Foundation of China (number: 82401338).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.