
Abstract
Primary adrenal extranodal natural killer (NK)/T-cell lymphoma (ENKTL) is exceptionally rare, and it remains unclear whether this subtype of ENKTL exhibits distinct clinicopathological features. This case report describes a later 30s female patient who presented with 6 months of back pain. 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) revealed a hypermetabolic left adrenal mass. Histopathology revealed diffuse atypical lymphocytes with necrosis and vascular invasion. Immunohistochemical analysis demonstrated tumor cell positivity for CD3, CD2, CD8, TIA-1, and granzyme B, while being negative for CD5, CD4, CD56, CD20, Pax-5, CD30 and keratin, with a Ki-67 proliferation index of approximately 80%. Chromogenic in situ hybridization showed strong and uniform nuclear positivity of Epstein–Barr virus-encoded RNA (EBER) in the neoplastic population. T-cell receptor rearrangement (TR-γ) was in germline configuration. The final diagnosis of primary adrenal CD56-negative extranodal NK/T-cell lymphoma was confirmed. Chemotherapy was initiated immediately. But she died within 4 months because of disease progression. Primary adrenal ENKTL appears to be exceedingly rare and might portend a particularly poor prognosis. CD56 negativity and advanced stage could potentially represent key prognostic determinants.
Introduction
Extranodal natural killer (NK)/T-cell lymphoma (ENKTL) is a subtype of mature NK/T-cell lymphoma that is prevalent in East Asia and Central and South America. ENKTL is associated with Epstein–Barr virus (EBV) infection. It occurs predominantly in midline structures, particularly the nasopharynx and upper airway region (nasal-type ENKTL). However, a similar disease can occur primarily in extranasal sites (e.g., skin, testis, intestine, muscle), or as a disseminated disease without any apparent nasal involvement. 1 Primary adrenal ENKTL is extremely rare, with only eight cases (including ours) reported in the English literature in the past two decades, and it is unclear whether this type of ENKTL has unique clinicopathological features.
Case report
A later 30s female patient was admitted to Gui Qian International Hospital in May 2022 for persistent 6 months of back pain. The patient had no significant past medical history, including any chronic inflammatory or infectious conditions. The laboratory data indicated a white blood cell count of 4.15 × 10⁹/L (62.4% neutrophils, 23.1% lymphocytes, and 7.7% monocytes), a hemoglobin level of 122 g/L, and a platelet count of 243 × 10⁹/L. At that time, serum cortisol level was 33.86 μg/dL at 8 AM, 18.48 μg/dL at 16 PM, and 5.96 μg/dL at 24 PM. 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) demonstrated a hypermetabolic left adrenal mass, without extra-adrenal lesions (Figure 1). Core biopsies showed diffuse proliferation of atypical lymphocytes (Figure 2(a)), with sheet-like necrosis and angiodestructive growth pattern (Figure 2(b)). The tumor cells varied in size, with clear cytoplasm, irregularly folded nuclei and small nucleoli (Figure 2(c)). Pathological mitotic figures were frequently observed (20 mitoses per 10 high-power field). Focal residual adrenal tissue was identified (Figure 2(d)). Immunohistochemistry (IHC) indicated that the tumor was positive for CD3 (Figure 3(a)), CD2, CD8 (Figure 3(b)), TIA-1 (Figure 3(c)), and granzyme B, while being negative for CD5, CD4, CD56 (Figure 3(d)), CD20, Pax-5, CD30, and keratin, with a Ki-67 proliferation index of approximately 80% (Figure 3(e)). Chromogenic in situ hybridization showed strong and uniform nuclear positivity of Epstein–Barr virus-encoded RNA (EBER) in the neoplastic population (Figure 3(f)). T-cell receptor-γ gene rearrangement (TR-γ) was germline. Based on pathological findings, the diagnosis of primary adrenal CD56-negative ENKTL was approved. The patient completed one cycle of chemotherapy at an external institution, but died 4 months later due to disease progression. Written informed consent was obtained from the patient's husband for publication. Our team had obtained the consent of patient’s husband for treatment. The patient's details have been de-identified. The reporting of this study conforms to CARE guidelines. 2

Radiological features of the case. There was a large mass in the left adrenal region with non-uniform density. The maximum cross-section was 68 mm × 79 mm. The boundary was unclear. There were no obviously enlarged nodules or nodules with increased FDG uptake in the head, neck, or chest.
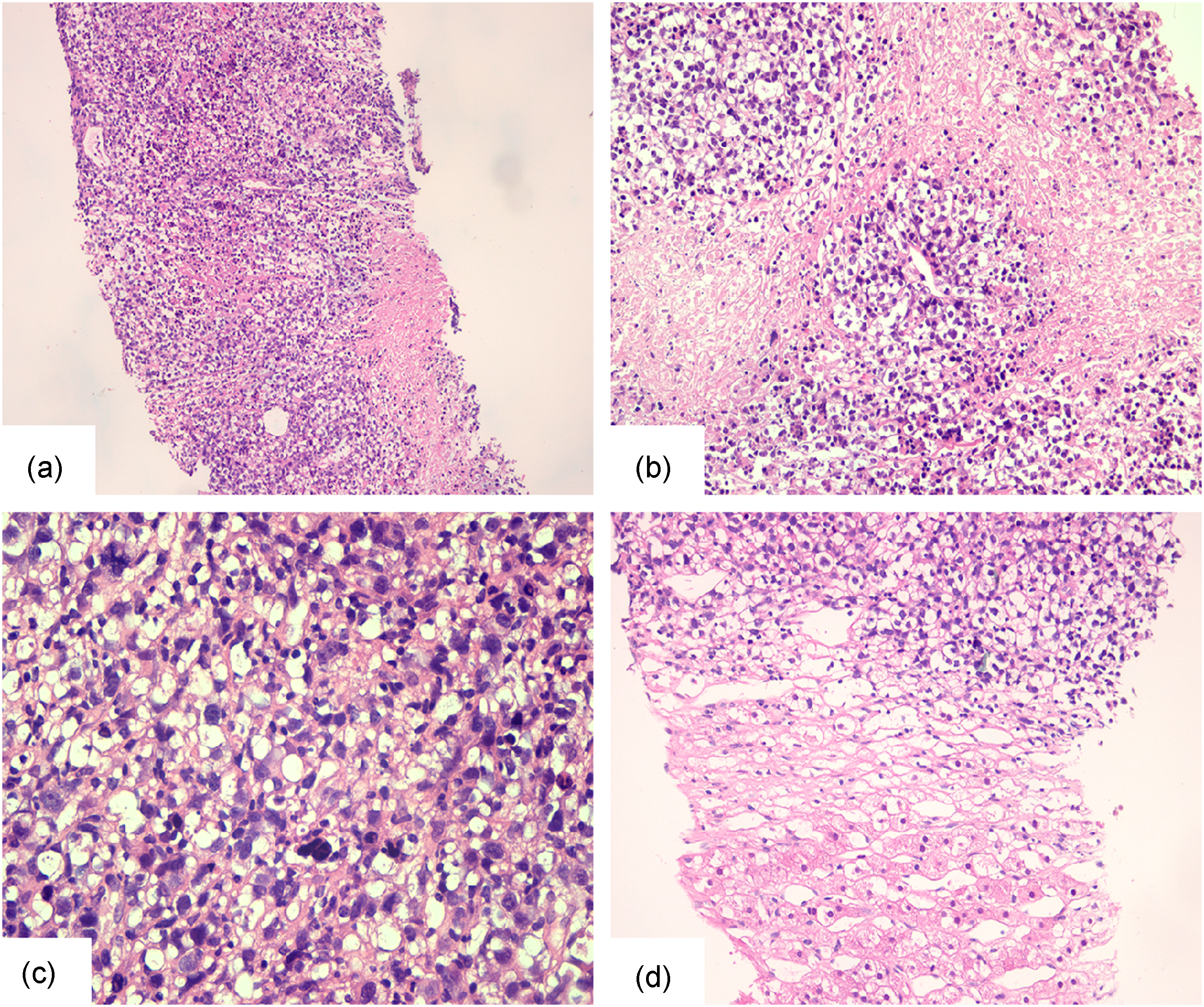
Histomorphological features of the needle biopsy specimen (hematoxylin and eosin stain). (a) Diffuse proliferation of atypical lymphocytes (×100 magnification). (b) Sheet necrosis and vascular invasion were noticeable (×200 magnification). (c) The tumor cells had obvious pleomorphism with clear cytoplasm, irregular nuclear contour, prominent nucleoli, and pathological mitotic figures (×400 magnification). (d) There was residual adrenal tissue in focal areas (×200 magnification).

Immunophenotype and in situ hybridization features. (a) CD3, (b) CD8, (c) TIA-1, (d) CD56, (e) Ki-67, and (f) EBER. All magnifications: ×400.
Discussion
Primary adrenal lymphoma or lymphoma involving mainly the adrenal gland without the regional lymph node involvement is very rare. All cases in our report presented with predominant adrenal involvement at initial diagnosis, without evidence of midline structure (e.g., nasopharyngeal) involvement (Table 1). To our knowledge, this is the best comprehensive collection of clinicopathological features of this rare tumor entity.
Reported cases of primary adrenal NK/T cell lymphoma.

Abbreviations: NK: natural killer; M: male; F: female; NM: not mentioned; ND: not done; TR-γ: T-cell receptor-γ gene rearrangement; EBER: Epstein–Barr virus-encoded small RNA:
Among the eight analyzed patients (five males and three females), with a median age at onset of 36 years (ranging from 17 to 79 years). Seven patients were of Asian descent. Imaging studies revealed bilateral adrenal lesions in five cases. All patients presented with abdominal or back pain, and three had concurrent fever. Adrenal hemorrhage, infection, or cortical and medullary tumors or metastases were initially considered clinically, but the definitive diagnosis depended on pathological biopsy. The morphological characteristics of primary adrenal ENKTL were similar to those observed in other anatomical sites. Peripheral T-cell lymphoma not otherwise specified (PTCL-NOS) was the most important differential diagnosis. Although CD56-negative, this tumor was characterized by angiocentric growth, prominent coagulative necrosis, cytotoxic phenotype, and association with EBV. These findings supported the diagnosis of ENKTL rather than PTCL-NOS. Among the eight reported cases (including the current case), two exhibited absent CD56 expression. Both cases exhibited fulminant disease progression and markedly reduced survival times of 33 days and 2 months, respectively, in sharp contrast to CD56-positive cases, which showed a mean survival time of 247 days. Experimental studies have suggested that CD56-negative ENKTL might represent a distinct clinicopathological subtype, as emerging clinical evidence indicates a significantly improved 5-year survival rate in patients with high CD56 expression compared to their CD56-negative counterparts. 10 The underlying mechanism may involve CD56 deficiency-induced impairment of NK cell migratory capacity and subsequent tumor microenvironment alteration. 11
In our series, primary adrenal ENKTL had a poor prognosis, with a median overall survival (median OS) of only 3 months, which was much shorter than that reported for the nasal ENKTL cohort by the International Peripheral T-cell Lymphoma Project (19.2 months). 12 One of the reasons for this may be the frequent presentation of primary adrenal ENKTL at advanced stages.
The data revealed that patients with neoplasms confined to the adrenal gland (n = 2) had favorable outcomes, with survival durations exceeding 12 and 26 months, respectively. Conversely, cases exhibiting multi-organ involvement were associated with dismal outcomes, showing 100% mortality within the observation period. Despite the absence of extra-adrenal spread at diagnosis in our case, survival duration was markedly shorter, potentially related to the CD56-negative phenotype.
The treatment of ENKTL includes radiotherapy, chemotherapy, and autologous stem cell transplantation. However, there is currently no effective treatment plan for this solid tumor. Cyclophosphamide, hydroxydaunorubicin (doxorubicin), oncovin (vincristine), and prednisolone (CHOP) is the most common chemotherapy for non-Hodgkin lymphoma. Despite not being a preferred regimen in the National Comprehensive Cancer Network (NCCN) guidelines for ENKTL therapy, Hu et al.7 reported favorable overall survival with this approach in their case. Furthermore, other therapeutic approaches, including immunotherapy (PD1/PDL1 inhibitor) and EBV-targeted therapies, are being progressively implemented in clinical practice. 13
Conclusion
Primary adrenal ENKTL appears to be exceedingly rare and might portend a particularly poor prognosis. CD56 negativity and advanced stage could potentially represent key prognostic determinants. Owing to the small cohort size in this preliminary study, we plan to prospectively enroll more cases in subsequent research to comprehensively characterize the clinicopathological features of this rare pathological entity.
Footnotes
Ethical approval
This study was approved by the ethics committee of Guiqian International Hospital on 1 April 2024. Approval number: GQGJ202404010321. Our institution approved the publication of the case details.
Consent to participate
Written informed consent was obtained from the patient's husband for this study.
Consent for publication
For this study, photos, and writing of our manuscript, the patient's husband has given their written informed consent.
Authors’ contributions
Chen Ying and Deyu Guo conceived and designed the case report. Dapin Zhong provided the clinical data. Xin He made the pathological diagnosis. Lina Wang contributed to the data analysis, and Yujuan Xu rechecked it. All authors contributed to the writing of the manuscript and approved the final version for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this presented case are included within this article.