
Abstract
Objective
Cognitive flexibility is the ability to transition between various tasks flexibly, which declines in aging. The purpose of this quasi-experimental study was to investigate the effect of a 12-week multicomponent exercise intervention on cognitive flexibility and attention, measured by color trail test (CTT)-1, CTT-2, and CTT 2-1 difference, in community-dwelling older adults. The relationship between cognitive flexibility and muscular fitness was also examined.
Methods
The participants were assigned to either the exercise group (n = 41, aged 70.6 ± 5.9 years) or the control group (n = 18, aged 67.9 ± 4.9 years). The exercise group participated in a 90-minute multicomponent exercise session, including endurance, resistance, and stretching training, twice a week for 12 weeks. Participants in the control group maintained their sedentary lifestyle. CTT and muscular fitness, including 30-second arm curl, 30-second chair stand, and 2-minute step tests, were measured before and after the intervention.
Results
A significant group×time interaction effect was found in CTT-2, CTT 2-1 difference, chair stand, and step test. After the intervention, the exercise group showed a significantly better cognitive flexibility, indicated by faster completion time in CTT-2 (before: 140.3 ± 60.1 seconds, after: 127.0 ± 60.6 seconds) and improved CTT 2-1 difference (before: 82.8 ± 49.5 seconds, after: 72.2 ± 49.0 seconds). The exercise group also improved the number of repetitions in chair stand (before: 18.5 ± 5.0, after: 22.8 ± 5.5) and step test (before: 108.9 ± 16.2, after: 126.2 ± 19.0). The cognitive and muscular performance remained unchanged in the control group. Moreover, better performance in the 30-second chair stand test was associated with faster completion time in CTT-1 at baseline (r = –0.296).
Conclusions
The amelioration in cognitive flexibility coincided with improvements in muscular fitness after a 12-week multicomponent exercise intervention in older adults. Better muscular strength was associated with higher cognitive flexibility at the baseline.
Introduction
The increasing number of older individuals globally is a significant demographic trend, with the World Health Organization projecting that by 2030, one in six people will be aged 60 or over. 1 As societies grapple with this demographic shift, the need to prioritize and sustain the health of the aging population becomes crucial to alleviate medical, economic, and social burden. Essential to this objective is the preservation of cognitive and physical abilities to enable individuals to carry out daily tasks and maintain their independence. 2
Advancing age is linked to a gradual reduction in various cognitive abilities, such as executive functioning, attention, processing speed, and memory. 3 These declines are thought to result, in part, from structural changes in the brain, with the frontal lobe being especially affected. 4 In light of the age-related decline in cognitive function, engaging in exercise emerges as a potent strategy to counteract these effects. An international consensus statement underscores the critical role of exercise in enhancing cognition, brain structure and function, perceptual and motor skills, and various physiological functions across musculoskeletal, metabolic, cardiovascular, and immune systems. 5
Recent longitudinal research has identified a link between reduced muscular fitness and a faster progression of cognitive decline. For instance, older Chinese adults with sarcopenia exhibited a greater prevalence of mild cognitive impairment compared to those without the condition. 6 Additionally, in a cohort of older Taiwanese men, greater muscular strength was positively associated with higher scores in global cognition, executive function, and attention over a 2-year follow-up period. 7 Several physiological factors that link both muscular and cognitive function have been identified.8,9 For example, decreasing testosterone levels are associated with risks for sarcopenia and dementia. 10
Cognitive flexibility, a crucial component of executive function, refers to the ability to transition flexibly between various tasks. 11 This proficiency becomes particularly crucial when managing multiple tasks simultaneously in daily life. It also enables individuals to rapidly and effectively generate diverse ideas, consider response alternatives, and modify behaviors to adeptly respond to changing circumstances. 12 The aging process is associated with a decline in cognitive flexibility, potentially through the decreased functional connectivity among various brain regions. 13 This decline may adversely affect daily functioning in older adults by impeding their ability to multitask and rapidly adapt to evolving situations prompted by new information and environmental demands. 14 Moreover, attention is a core cognitive ability in humans, essential for processing information and guiding behavior. It underlies nearly every facet of human activity, as most actions and decisions depend on effective attentional control and regulation. 15
To improve the overall quality of life for older adults, multicomponent exercise programs are commonly recommended, incorporating elements such as endurance, strength, flexibility, and balance training. 16 Evidence from research indicates that multicomponent exercise programs may be more effective in enhancing cognitive function in older adults than exercise interventions focused exclusively on either endurance or resistance training. 17 Muscular fitness, including strength and endurance can have a crucial role in preserving cognitive function in older adults. 18 However, whether multicomponent exercise can enhance cognitive flexibility and attention through improvements in muscular fitness remains uncertain. The purpose of this study was to investigate the effect of 12-week multicomponent exercise intervention on cognitive flexibility and attention, measured by the cultural-inclusive Color Trail Test (CTT), in healthy community-dwelling older Taiwanese adults. The association between these cognitive functions and muscular fitness was also examined. It is hypothesized that the exercise intervention can improve cognitive flexibility and muscular fitness. Additionally, the cognitive and muscular functions are positively related.
Methods
Study design
This was a quasi-experimental study with a pretest–posttest design, in which participants were non-randomly assigned to either an exercise or a control group. The study spanned 14 weeks, beginning with pre-intervention CTT and muscular fitness assessments in the first week, followed by a 12-week intervention period, and concluding with post-intervention CTT and muscular fitness assessments in the 14th week. The multicomponent exercise program was designed in accordance with the exercise guidelines for older adults issued by the American College of Sports Medicine and the American Heart Association. 16 Initial feedback on the exercise program was sought from five experts specializing in exercise for older adults. Subsequent adjustments were made based on their comments, and the revised intervention program received approval from the experts. The study protocol was approved by Research Ethics Committee, China Medical University Hospital, Taichung, Taiwan (CMUH111-REC2-090) on Aug 5, 2022. The reporting of this study conforms to STROBE guidelines. 19 This study was conducted according to the Helsinki Declaration of 1975 as revised in 2024. All participant details were de-identified to ensure that no individual could be identified in any way.
Participants
Community-dwelling participants were recruited from Chia-Yi County, Taiwan. Eligibility criteria included individuals aged 60 years or older who were literate, capable of free movement, able to communicate clearly through speaking and writing, and free from cognitive impairment, severe cancer, cardiovascular disease, diabetes, hypertension, or arthritis, and who had not engaged in regular physical activity during the past 12 months. Recruitment was conducted from August to September 2022 through social media, poster announcements, and word-of-mouth referrals.
A total of 70 participants passed the screening process conducted with the Physical Activity Readiness Questionnaire 20 and were then assigned to the exercise group (50 participants) and the control group (20 participants). All participants gave the written informed consent to the research and to publication of the results. Only exercise group participants with an attendance rate exceeding 80% were included in the final analysis, yielding 41 individuals. In the control group, two participants were lost during follow-up, resulting in a final sample of 18 individuals.
Interventions
The intervention was implemented between September and December 2022. The exercise program was designed according to recommendations from the American College of Sports Medicine and the American Heart Association. 16 Participants in the exercise group attended 90-minute group-based classes twice weekly over a period of 12 weeks. Each session was led by certified fitness instructors who followed a standardized progression protocol. The session structure included a 10–15-minute warm-up, 40–45 minute of aerobic endurance exercises, 10–15 minute of resistance exercises, and 15–20 minute of stretching.
The aerobic endurance component was designed to progressively challenge participants. The routine began with basic aerobic dance movements and evolved to incorporate more complex choreographic elements and increased movement velocity. Instructors continuously regulated exercise intensity to maintain a perceived exertion between 5 and 6 on the 10-point Borg scale, with increased complexity and movement velocity occurring every 2 to 3 weeks. Instructors also regularly checked with participants during exercise to ensure that perceived exertion remained within the targeted range and adjusted intensity accordingly.
The resistance training component targeted major muscle groups in the upper and lower body. Movements such as leg press, knee extension, knee flexion, hip abduction, bicep curl, and tricep extension were performed using elastic bands. This protocol was based on the principle of progressive overload. Participants started with 8 repetitions per movement, and the regimen was structured to advance to 10 repetitions as the program progressed. Instructors adjusted the resistance provided by the elastic bands and numbers of repetitions according to individual performance and to maintain a perceived exertion between 5 and 6 on the 10-point Borg scale, ensuring that the workload promoted strength gains while maintaining safety.
The stretching component featured simple yoga-based movements aimed at improving flexibility and targeting major joints including the arms, legs, neck, and back. Although the stretching exercises remained relatively consistent throughout the program, instructors offered individualized modifications to address evolving flexibility and recovery needs. For instance, instructors implemented yoga movements such as downward-facing dog, child's pose, cobra pose, seated forward bend, and cat-cow stretch to facilitate comprehensive joint mobilization and muscle relaxation.
Participants in the control group were instructed to maintain their sedentary lifestyle. These individuals had not engaged in regular physical activity during the 12 months prior to the study.
Anthropometric measurement
Body height and weight was measured with an electronic scale. Waist and hip circumference was measured with stretch-resistant tapes by a trained personnel. Waist circumference was measured at the midpoint between the lower margin of the last palpable rib and the top of the iliac crest. Hip circumference was measured at the widest portion of the buttocks. 21
Color trail test
The CTT is a cultural-inclusive alternative to the Trail Making Test (TMT), a widely used neuropsychological assessment in clinical settings. 22 The CTT replaces the English alphabets in the TMT with numbers. 23 This study used the Chinese version of the CTT following Kuo and Hua's procedure. 24 In CTT-1, participants connected encircled numbers (1–25) sequentially, while in CTT-2, they alternated between pink and yellow numbered circles. Errors were corrected during the test, and completion times for CTT-1 and CTT-2 were recorded. The difference between CTT-2 and CTT-1 (CTT 2-1 difference) was also calculated.
CTT-1 assesses sustained and divided attention, visual scanning, and processing speed while CTT-2 evaluates cognitive flexibility and working memory.11,25 The CTT 2-1 difference provides information on cognitive flexibility independent of motor and visual scanning ability. 23 The test–retest reliability for CTT-1 and CTT-2 was 0.618 and 0.833, respectively. 24
Muscular fitness test
Muscular strength and endurance were evaluated before and after the intervention according to Rikli and Jones, 26 which are relevant to daily activities and maintain autonomy in older adults.
Upper body strength was assessed using a 30-second arm curl test, where participants performed bicep curls with an 8-lb dumbbell for men or a 5-lb dumbbell for women. The total number of repetitions completed in 30 seconds was recorded.
Lower body strength was measured with a 30-second chair stand test. Participants stood up and sat down from a chair with arms crossed, and the total number of stands completed in 30 seconds was recorded.
Lower body endurance was assessed using a 2-minute step test. Participants stepped in place, raising each knee to a marked height between the iliac crest and patella. The number of times the right knee reached the target height in 2 minutes was recorded, with pauses allowed if form was compromised.
Statistical analysis
Data are presented as means ± standard deviations. Baseline anthropometric data between the exercise and control groups were compared using t-test. Body weight and waist and hip circumference before and after the intervention within each group were compared with paired t-test. For CTT and muscular fitness data, a repeated-measures analysis of variance was conducted, with time considered as the within-subject factor and group as the between-subject factor. In the presence of a significant group × time interaction effect, Bonferroni post hoc analysis was used to identify differences before and after the intervention in each group. The effect sizes of repeated-measures ANOVA are expressed as partial η2 values. Effect size in the differences between conditions was assessed using Cohen's d. The criteria for interpreting effect sizes are as follows: partial η2 values of small (≥0.01), medium (≥0.06), and large (≥0.14); Cohen's d values of small (≥0.2), medium (≥0.5), and large (≥0.8). The correlation between variables was analyzed by Pearson's correlation coefficient. Statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, USA). A significance level was set at p < 0.05.
Results
Table 1 presents basic characteristics at the baseline and after the 12-week intervention in the exercise and control group. The age range was 62–85 years in the exercise group and 61–82 years in the control group. Anthropometric parameters were similar at the baseline between the two groups. Participants in the exercise group significantly reduced waist (p < 0.001, d = 0.425) and hip circumference (p = 0.008, d = 0.182) while maintaining body weight (p = 0.061, d = 0.047) after the intervention.
Basic characteristics before and after the 12-week intervention in the exercise and control group (mean ± standard deviation).
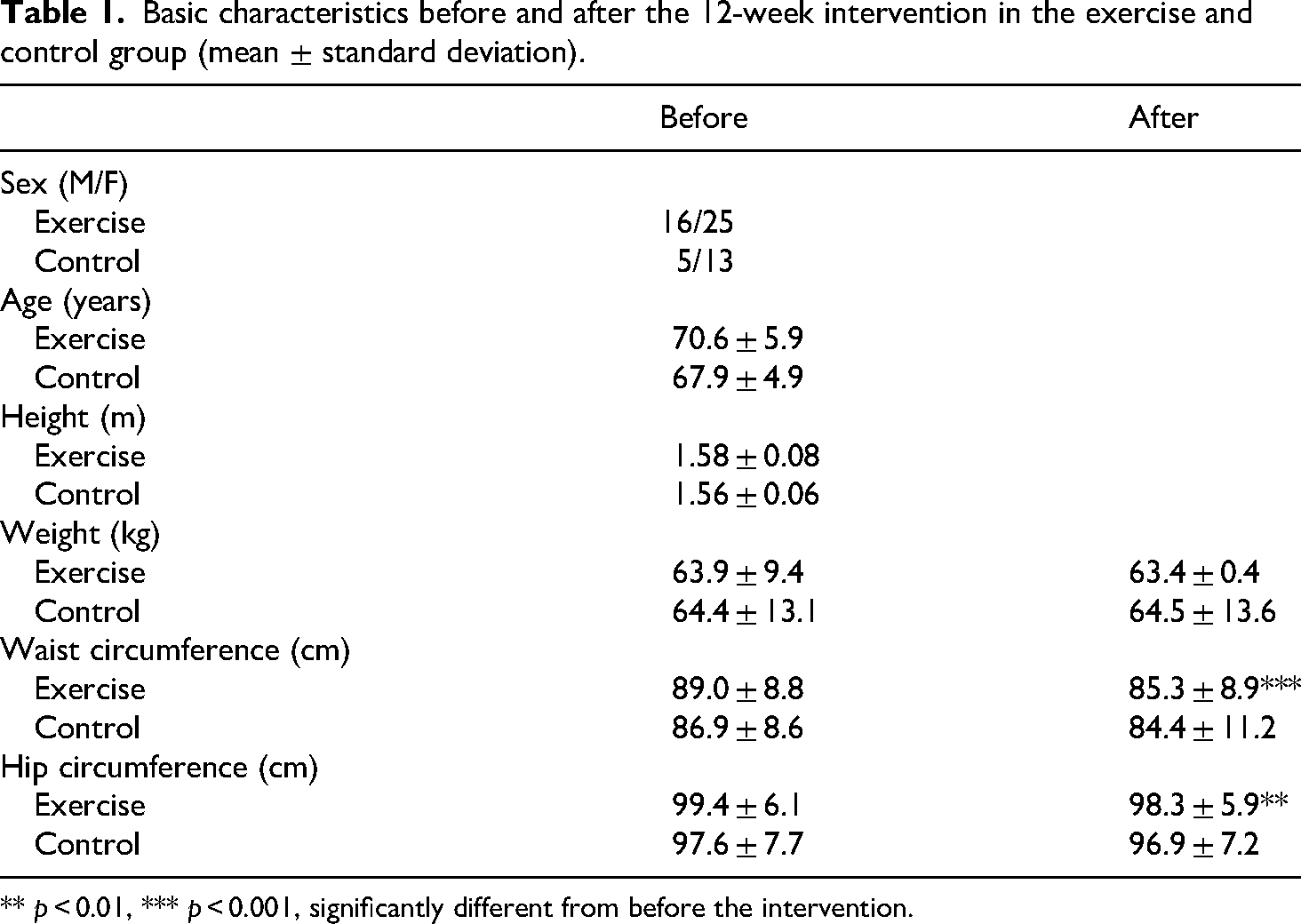
** p < 0.01, *** p < 0.001, significantly different from before the intervention.
The performance in CTT-1, CTT-2, and CTT 2-1 difference are presented in Table 2. A significant group × time interaction effect was observed in CTT-2 (p = 0.003, η2p = 0.147) and CTT 2-1 difference (p = 0.020, η2p = 0.091). Post hoc analysis revealed that the exercise group had a significantly faster completion time in CTT-2 (p = 0.001, d = 0.220) while no significant change was observed in the control group. Moreover, the exercise group exhibited an improved CTT 2-1 difference after the intervention (p = 0.018, d = 0.214). Participants in the exercise group significantly improved the performance in arm curl (p < 0.001, d = 0.723), 30-second chair stand (p < 0.001, d = 0.822), and 2-minute step test (p < 0.001, d = 0.982) after the intervention (Table 3). Conversely, the muscular fitness for participants in the control group remained unchanged after the intervention period. In addition, better performance in 30-second chair stand test is associated with faster time in CTT-1 (r = -0.296, p = 0.023, Figure 1).

The correlation between color trail test-1 test time and 30-second chair stand test performance at the baseline in all participants.
Performance in color trail test (CTT) before and after the 12-week intervention in the exercise and control group (mean ± standard deviation).

* p < 0.05, ** p < 0.01, significantly different from before the intervention in the exercise group.
Muscular fitness test results before and after the 12-week intervention in the exercise and control group (mean ± standard deviation).
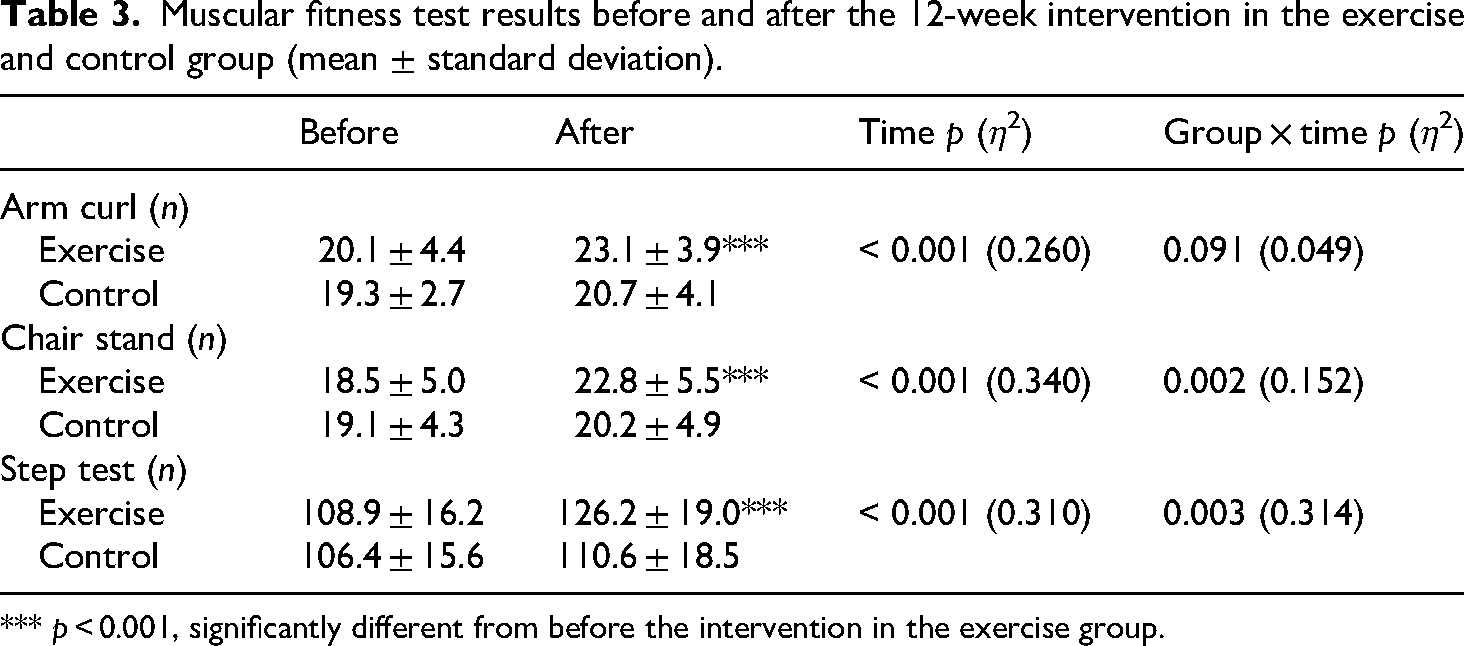
*** p < 0.001, significantly different from before the intervention in the exercise group.
Discussion
This study revealed that a 12-week multicomponent exercise improved cognitive flexibility measured by CTT-2 and CTT 2-1 difference in community-dwelling older adults aged 62 to 85 years. The amelioration in cognitive flexibility coincided with significant improvements in muscular strength and endurance. Furthermore, better cognitive flexibility was significantly associated with higher muscular endurance at the baseline.
CTT performance declines with age, as older adults exhibit longer completion time than their younger counterparts in both Western27,28 and Taiwanese populations. 29 In agreement to our results, previous studies have revealed that multicomponent exercise programs improved performance in CTT-2 or TMT-B in older adults. For instance, 3-month exercise program with stationary bicycles significantly improved performance in CTT-2 in older participants. 30 Programs including aerobic, resistance, flexibility, and balance exercise also resulted in faster time to completion in CTT-2 and TMT-B in older adults.31,32 An aerobic or resistance exercise program alone can produce a comparable magnitude of improvement in TMT-A and TMT-B performance. 33 Additionally, other forms of exercise, such as Tai Chi 34 and dual-task training that combined physical activity with cognitive tasks, 35 have also been shown to enhance performance on both the CTT and TMT. Notably, a single bout of 20-minute moderate intensity aerobic exercise is effective in improving cognitive flexibility in older adults. 36
To the best of our knowledge, the present study is the first to examine the effect of exercise on the CTT 2–1 difference, an indicator of cognitive flexibility, in older adults. Our findings suggested that participation in a multicomponent exercise program led to significant improvement in the CTT 2–1 difference, suggesting enhanced cognitive flexibility. This result aligns with previous studies that have reported positive effects of exercise on a similar cognitive measure, the TMT-B–A difference.37,38 It is plausible that the observed improvement in cognitive flexibility may be mediated by exercise-induced increases in brain-derived neurotrophic factor (BDNF). Supporting this hypothesis, prior research has shown that a single-nucleotide polymorphism in the BDNF gene can influence the extent to which exercise affects the TMT-B–A difference. 37 BDNF, a member of the neurotrophin family of growth factors, plays a critical role in supporting neuronal survival and maintenance, promoting synaptic plasticity, and facilitating memory formation in older adults. 39
The decline in cognitive function associated with aging results from deteriorations in brain function and structure, processes that can be mitigated through exercise. An in vivo study found that alternations in frontoparietal functional connectivity and striatal dopamine synthesis were associated with the decline in cognitive flexibility during aging. 40 Acute exercise has been shown to improve various execution functions, including cognitive flexibility, by increasing oxygenation in the prefrontal cortex. 41 Furthermore, a 12-week exercise program increased gray matter volume in specific areas of the frontal cortex and hippocampus in older adults. This increase was correlated with improved cognitive function. 42 A recent meta-analysis also reported a significant improvement in white matter integrity in the brains of older adults who exercised regularly. 43 This evidence highlights the benefits of exercise in enhancing brain structure, which may help mitigate cognitive decline in older adults.
Our findings indicated significant improvements in cognitive flexibility and muscular strength and endurance among participants in the exercise group. In addition, better muscular strength at the baseline was associated with superior CTT-1 performance. Recent longitudinal studies have revealed a crucial role of muscle mass and muscular fitness in preserving cognitive function in older adults. A systematic review and meta-analysis concluded that muscular strength at the baseline had a protective effect against cognitive decline. 18 Severe sarcopenia in Taiwanese older women was associated with a higher likelihood of global cognitive impairment over a 2-year span compared to those without sarcopenia. Similarly, greater muscular strength was associated with a lower risk of cognitive decline in older American adults during a 20-year follow-up period. 44 Meta-analyses have reported that peripheral blood BDNF concentrations increased significantly following exercise training in older adults.45,46 Given that exercise training is effective in enhancing muscle mass and strength, BDNF may act as a key mediator linking muscular fitness to cognitive function in older adults. Additional mechanisms potentially underlying the association between muscle mass, muscular fitness, and cognitive function include chronic inflammation, mitochondrial dysfunction and oxidative stress, as well as neuroendocrine factors such as testosterone, insulin, and other growth-related hormones. 8
This study has several limitations. Firstly, variables such as diet, dietary supplements, and medications, which could potentially impact cognitive function and muscular fitness, were not controlled. Secondly, despite participants being generally free from severe chronic diseases, some individuals might have undisclosed clinical conditions that could influence cognitive function and muscular fitness. Thirdly, external physical activity beyond the designated program was not monitored or controlled. Lastly, the unequal sample sizes between the exercise and control groups may have reduced the statistical power of the study.
Conclusion
This study revealed that a 12-week multicomponent exercise program may improve cognitive flexibility and muscular fitness in Taiwanese older adults between the ages of 62 and 85 years. Incorporating multicomponent exercise into health promotion programs for older adults may be crucial for preventing declines in cognitive and physical functions. Future research could use functional magnetic resonance imaging to elucidate the impact of multicomponent exercise on brain functions during cognitive flexibility tasks. Moreover, the mechanisms linking muscular fitness and cognitive functions, such as myokines, inflammation, and mitochondrial function, warrant further investigation.
Footnotes
Acknowledgments
The authors thank all participants for their time and effort.
Author contributions
Yi-Ling Chen performed conceptualization, methodology, and writing—original draft. Ching-Hsiang Chen did methodology, investigation, and writing—original draft. Ruey-Rong Huang did methodology and investigation. Chien-Hsing Tseng did conceptualization, writing—original draft, and writing—review and editing. Hsueh-Chin Chao did investigation, analysis, writing—review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.