
Abstract
Lumbar transverse process injuries are rare in adolescent athletes, with very few documented cases related to sports activities, particularly involving the fifth lumbar region. This report aims to highlight the clinical presentation, diagnosis, and management of apophyseal injuries of the fifth lumbar transverse process in two adolescent athletes. Two adolescent athletes, a 14-year-old boy and a 15-year-old girl, presented with subacute onset of unilateral lower back pain (LBP) following repetitive athletic activities. Both patients had a history of spondylolysis that had previously healed. Initial clinical assessments, including physical examination and imaging studies (CT and MRI), were performed to diagnose the nature of their injuries. Conservative treatment, including rest and specific rehabilitation exercises, was employed. Both patients exhibited right-sided LBP exacerbated by specific movements, mimicking symptoms of lumbar spondylolysis. Imaging studies revealed no evidence of spondylolysis but indicated a slight widening of the growth plate and high-intensity signal changes in the right fifth lumbar transverse process apophysis. Both patients returned to their sports activities within a month of starting treatment, with no recurrence of symptoms reported during follow-ups. Apophyseal injuries of the fifth lumbar transverse process, though rare, should be considered in the differential diagnosis of adolescent athletes presenting with unilateral LBP, especially in the absence of acute trauma.
Introduction
Low back pain (LBP) is a common symptom among adolescent athletes, presenting a diagnostic challenge due to its multifactorial etiology. The prevalence of LBP in this population ranges approximately from 20% to 40% in prevalence, with variations depending on the type of sport. 1 Numerous conditions, including acute trauma, chronic overuse, repetitive trauma, and referred pain, can induce LBP in adolescent athletes. When treating LBP, it is crucial to diagnose specific LBP linked to specific medical treatments. Specific differential diagnoses included lumbar spondylolysis, discogenic LBP, lumbar disc herniations, ring apophysis fractures, facet joint disorders, and sacroiliac joint disorders. 2 Lumbar spondylolysis is the most crucial differential diagnosis in this population. 2 The optimal outcome for adolescents with lumbar stress fractures is bone union. Given the significant correlation between the stage of lumbar stress fracture and the likelihood of achieving bone union, as demonstrated in previous research, early identification of lumbar stress fractures is essential for achieving bone union through conservative management in adolescent athletes. 3 In adults, various physical examination tests and the identification of red flags are employed to diagnose serious pathologies such as fractures, infections, and malignancies associated with LBP4,5 However, especially in cases of overuse injuries, such as lumbar stress fractures in younger individuals, establishing a clear relationship between diagnosis and specific symptoms and physical findings often presents challenges.
Lumbar transverse process injuries may also present with LBP; however, sports-related cases, particularly in the fifth lumbar region, are extremely rare.6–10 Port-related transverse process fractures are typically associated with acute high-energy direct trauma or violent muscular contractions during American football,6,7 soccer, 8 skiing, and snowboarding. 9 However, there have been few reports of subacute-onset transverse process injuries, especially among younger populations. 10
Here, we present two cases of adolescent athletes with unilateral LBP attributed to an apophyseal injury of the fifth lumbar transverse process. We explored the clinical presentations, diagnostic imaging, and treatment approaches of this pathology (Graph 1).
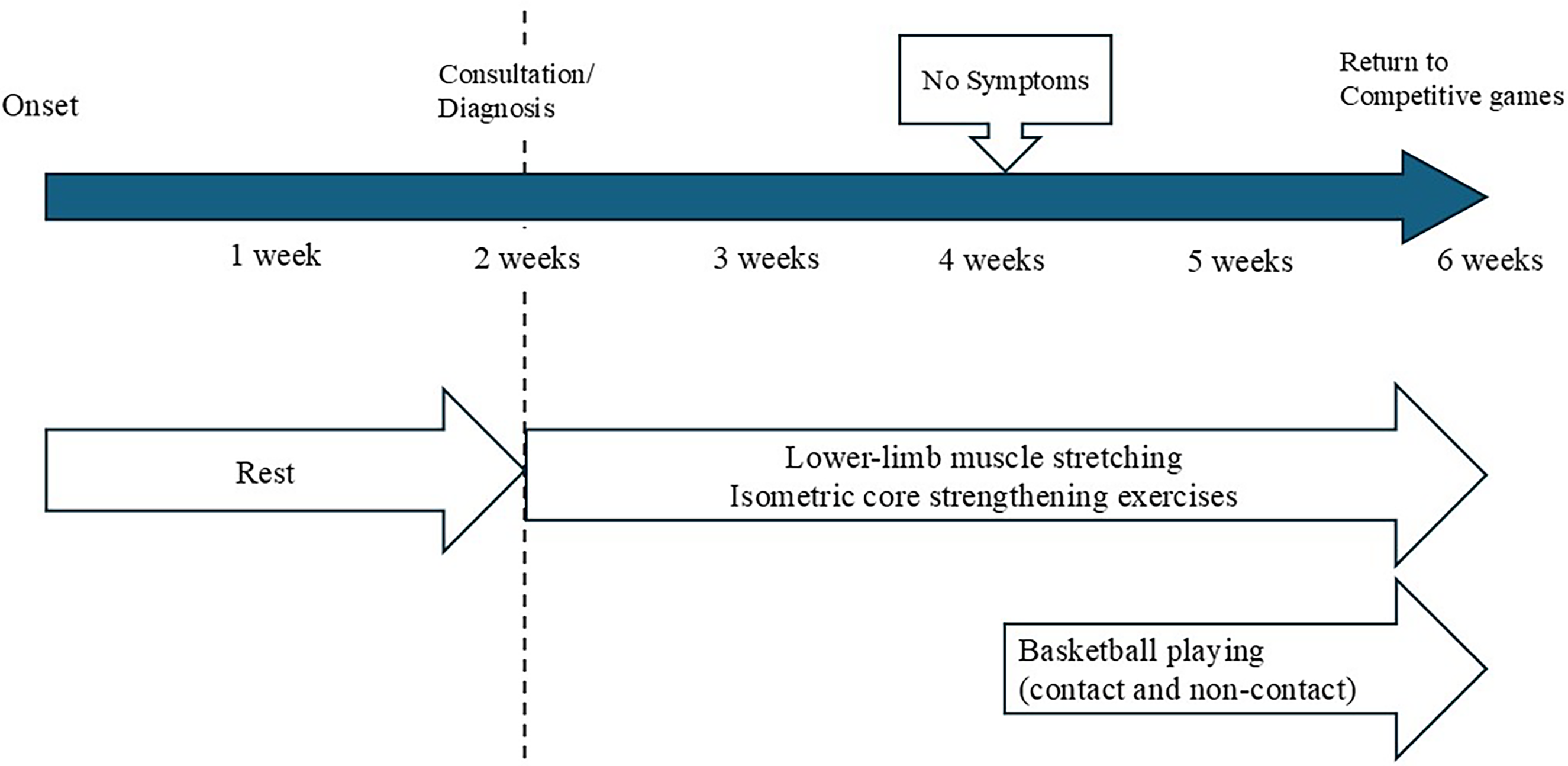
Treatment timeline for Case 1: from onset to return to play. The patient's target competitive games were scheduled to take place 4 weeks after the diagnosis.
Case presentation
The reporting of this study conforms to CARE guidelines. 11 At our institution, case reports do not require approval from an ethics review committee. All patients described in this paper, along with their parents, provided written informed consent for publication.
Case 1
Chief complaint and present history
The patient, a 14-year-old boy with a height of 163 cm and weight of 54 kg, was right-handed and played competitively on a basketball team. He developed subacute onset of right-sided LBP after repeated running and jumping activities, for which he sought treatment at a chiropractic clinic. Despite 2 weeks of rest, his symptoms persisted, and he was referred to our institution.
Past medical history
He had a previous history of spondylolysis of the right fourth (L4) and the left fifth (L5) lumbar vertebrae, which occurred 1 year prior to the consultation and had healed with conservative treatment, with confirmation by magnetic resonance imaging (MRI) (Graph 2).

Treatment timeline for Case 2: from onset to return to play.
Physical examination
Upon initial assessment at our clinic, he reported right-sided LBP exacerbated by backward and left lateral bending. There was no tenderness over the spinous processes or facet joints, and both the Kemp sign and straight leg raising (SLR) test were negative. Both sensation and muscle strength in the lower limbs were found to be normal.
Investigations
His bone growth stage was assessed Risser grade 4/5. High-intensity signal changes only on the right side of the L5 transverse process apophysis were observed on short-tau inversion recovery (STIR) sequences on MRI, with corresponding pinpoint tenderness on palpation (Figure 1(a)). In addition, computed tomography (CT)-simulated sequences revealed a slight widening of the growth plate of the right L5 transverse process apophysis (Figure 1(b)).
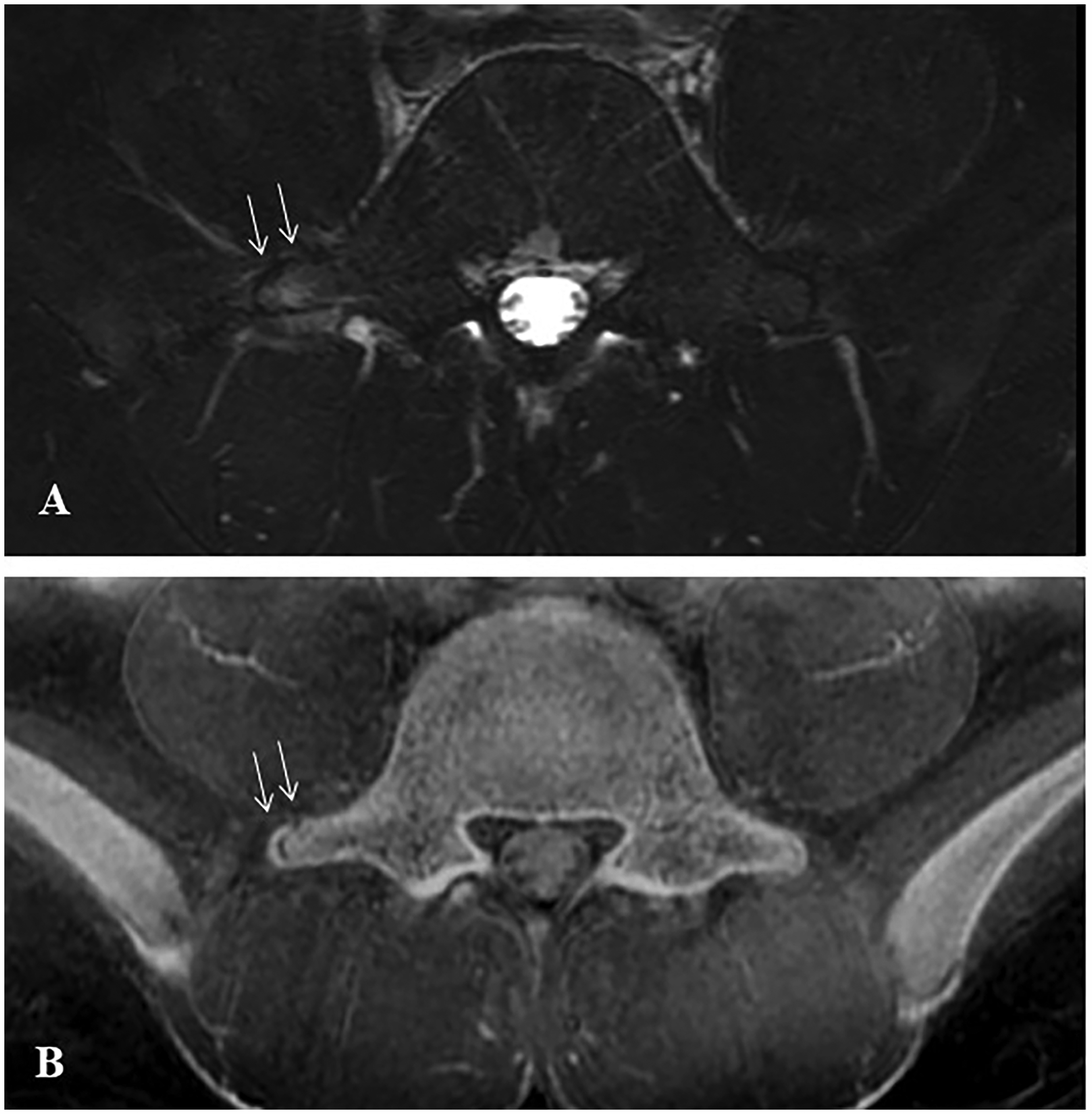
High-intensity signal changes were observed only on the right side of the L5 transverse process apophysis (arrows) in the axial view of the short-tau inversion recovery sequences on MRI (A). The axial view of the computed tomography-simulated sequences revealed a slight widening of the growth plate of the right L5 transverse process apophysis (arrows) (B).
Differential diagnosis
Considering his history and symptoms, the initial differential diagnoses included lumbar spondylolysis and myofascial LBP. However, the imaging findings and clinical correlation led to a diagnosis of a right L5 transverse process apophysis injury at the iliolumbar ligament attachment site.
Treatment
The patient's target competitive games were scheduled to take place 4 weeks later. With the consent of the patient and his family, conservative management without the application of a lumbar orthosis was initiated, and only lower-limb muscle stretching and isometric core strengthening exercises were permitted for 2 weeks. At the 2-week follow-up, the patient reported no pain during backward or lateral bending and palpation, showing a full range of motion in the lumbar spine. Furthermore, improvement in lower limb tightness was noted, leading to clearance for athletic training and sports participation (both non-contact and contact playing). Six weeks after onset (4 weeks after the initiation of treatment), he returned to competitive games without declining performance levels or any recurrence of symptoms (graphic timeline 1). He had no symptom recurrence during the 1-year follow-up. The patient and his parents were informed that additional imaging evaluations were recommended to be performed at the final follow-up. However, the patients and their parents did not opt for additional imaging evaluations, as the patient's symptoms had completely resolved clinically, and the course remained favorable.
Case 2
Chief complaint and present history
The patient was a 15-year-old girl who engaged in track and field, particularly in the long jump, standing at 159 cm, and weighing 53 kg. Her dominant (takeoff) foot was the left. During winter training, the patient experienced right-sided LBP following repeated jumping and sprinting exercises, excluding actual long jumps. Despite a week of rest, her symptoms persisted, leading to referral to our institution.
Past medical history
At the age of 12, she was diagnosed with bilateral L4 spondylolysis, which resolved with conservative treatment. Bone healing was confirmed using CT and MRI.
Physical examination
Initial assessment at our institution revealed right-sided LBP exacerbated by forward, backward, and left lateral bending, with tenderness noted over the distal aspect (tip) of the right L5 transverse process. Both the Kemp sign and the SLR test yielded negative results. There was no tenderness in the sacroiliac joint or restriction of the hip joint range of motion. Both sensation and muscle strength in the lower limbs were found to be normal.
Investigations
Her bone growth was assessed as Risser grade 4/5. Trunk CT revealed slight widening of the growth plate of the right L5 transverse process apophysis (Figure 2(a)). MRI imaging showed high-intensity signal changes on the right side of the L5 transverse process apophysis and perimuscular high-intensity signal anterior to the transverse process in STIR sequences (Figure 2(b)).

A slight widening of the growth plate of the right L5 transverse process apophysis (arrows) was observed on the axial view of the CT image (A). High-intensity signal changes on the right side of the L5 transverse process apophysis (arrows) and perimuscular high-signal spread (arrowheads) anterior to the transverse process were observed in the axial view of STIR sequences on MRI (B). At 3 months post-injury, MRI showed no high-intensity signal changes around the apophysis or surrounding perimuscular on the STIR sequence (arrows and arrowheads) (C).
Differential diagnosis
Given her medical history and symptoms, the initial differential diagnosis included lumbar spondylolysis, myofascial LBP, and sacral stress fractures. However, imaging findings and clinical correlation confirmed the diagnosis of right L5 transverse process apophysis injury at the iliolumbar ligament attachment site.
Treatment
Conservative management was initiated with the consent of the patient and her family without the use of a lumbar orthosis. After a week of rest, isometric spinal muscles and squat exercises were introduced. With an improvement in LBP noted after another week, light jumping movements, such as jogging and rope skipping, were permitted. At the 4-week follow-up examination, the patient reported no pain when bending the trunk in any direction with a full range of motion of the lumbar spine. She was gradually able to resume athletic training (graphic timeline 2) and has remained symptom-free since then. Three months after onset, MRI showed that the high-signal changes observed in the STIR sequences had disappeared, and there was no expansion of the growth plate (Figure 2(c)). Six months after onset, she achieved a personal record of a long jump at a competition, with no recurrence of symptoms during the 1-year follow-up.
Discussion
Here, we present two rare adolescent cases of unilateral LBP attributed to apophyseal injury of the fifth lumbar transverse process caused by sports. The patients presented with notable clinical features. First, its clinical presentation resembles that of lumbar spondylolysis. Second, both cases involved the L5 region. Third, both patients had a history of spondylolysis.
An apophyseal injury in the L5 transverse process may mimic the presentation and physical findings of lumbar spondylolysis. Lumbar spondylolysis is the most common cause of LBP in adolescent athletes aged ≥10 years and is often induced by repetitive lumbar extension movements. 3 Additionally, pain during lumbar lateral flexion has been reported to aid in the diagnosis of early-stage lumbar spondylolysis. 12 In the present cases, both athletes in their teens experienced symptoms with repetitive movements, and LBP was induced by lumbar extension and lateral flexion, initially raising the suspicion of recurrent spondylolysis. However, subsequent CT and MRI (especially STIR sequences) examinations ruled out spondylolysis, leading to a diagnosis of an apophyseal injury of the L5 transverse process. Discogenic LBP, lumbar disc herniations, ring apophysis fractures, facet joint disorders, and sacroiliac joint disorders were excluded, based on clinical findings and imaging studies. Differentiating between lumbar spondylolysis and apophyseal injury in the L5 transverse process poses a challenge because of overlapping physical findings; thus, imaging studies may be instrumental. Although ultrasonography was not performed in the present cases, it may serve as a simple and noninvasive modality for visualizing the lumbar transverse processes and may have potential in the diagnosis of this condition. 13 In addition, contralateral LBP with lateral bending may also be observed in myofascial LBP of the quadratus lumborum. 14 Palpation may be useful in differentiating between myofascial LBP of the quadratus lumborum and L5 transverse process apophyseal injuries. However, further case analyses are needed.
Apophyseal injury of the L5 transverse process in adolescent athletes may occur due to the repetitive traction force on the iliolumbar ligament attached to the L5 transverse process. Although L5 transverse process fractures are generally considered to result from acute high-energy trauma, there have also been reports of stress fractures at the base of the transverse process caused by repetitive trunk rotation during sports activities.15,16 However, in the present case, neither patient had any history of acute trauma, including pelvic injury, suggesting the possibility of overuse. While the typical age range for apophyseal injuries varies depending on the anatomical site, it is generally considered to be between 10 and 18 years. During this growth period, secondary ossification centers at the apophyses are structurally weaker than adjacent musculotendinous units, making them more susceptible to traction injuries due to repetitive mechanical stress, particularly in adolescent athletes. 17 The L5 transverse process is attached to the iliolumbar ligament, and traction on this ligament may lead to apophyseal avulsion injury. 18 The iliolumbar ligament contributes to the stability of the sacroiliac joint, 18 particularly influencing the stability of lumbar flexion and lateral bending at L5-S1. 19 It has also been reported that the iliolumbar ligament contains a rich supply of free nerve endings, suggesting that ligament injuries may induce pain. 20 These injuries are likely to occur in athletes who frequently perform jumping activities in which forced lumbar extension and lateral bending occur during landing. Further, some reports indicate that repetitive traction forces applied to the middle layer of the lumbar fascia comprising the transversus abdominis, iliopsoas, and quadratus lumborum muscles during lateral bending and increased intra-abdominal pressure can result in transverse process fractures of L1–L4, particularly L3, suggesting a possible contribution to the present cases.21,22 Therefore, such injuries should be considered when diagnosing LBP in adolescent athletes. The differences in pain-eliciting trunk movement between the two cases may reflect differences in injury severity and time from onset to initial consultation. On MRI, Case 1 showed signal changes limited to the bone, while Case 2 showed additional changes in the surrounding soft tissues, suggesting a more extensive injury and possibly inducing pain in many directions (Pain of Case 2 was exacerbated by forward, backward, and left lateral bending). In addition, Case 1 was assessed after 2 weeks of rest (2–3 weeks after onset), whereas Case 2 was evaluated after only 1 week of rest after onset. This discrepancy in timing may have allowed for some resolution of inflammation and stabilization of the fracture in Case 1, potentially influencing the clinical presentation and pain responses during physical examination (Pain in Case 1 was exacerbated by only backward and left lateral bending). Specifically, the pain experienced by the patient in Case 1 during left lateral flexion, which stresses the iliolumbar ligament, could allow localized stress responses in the ligament. Regarding pain during extension, anatomical variations in the iliolumbar ligament should be considered. 23 In Case 1, this ligament may have been subjected to increased stress during extension rather than flexion, contributing to symptomatic presentation. Further investigative studies are warranted to elucidate these observations and better understand the biomechanical implications of such injuries on the iliolumbar ligament and associated structures.
Risk factors for lumbar spondylolysis and L5 transverse process apophyseal injuries may overlap. Risk factors for lumbar spondylolysis include being male and participation in sports involving repetitive lumbar extension and rotational movements (e.g., baseball, soccer, hockey for males and gymnastics, softball, and lacrosse for females). 24 Both patients had a history of lumbar spondylolysis (both achieved bony fusion and were returning to sports) and shared similarities with athletes who required repetitive lumbar extension and rotational movements. However, the specific movements or postures that place distinct mechanical stress on the iliolumbar ligament remain unclear and warrant further investigation.
The early-to mid-term prognosis for apophyseal injury to the L5 transverse process may be relatively favorable. The union rate of unilateral spondylolysis has been reported to be 98.2% in the very early stages, 96.0% in the early stages, and 64.3% in the progressive stages. 25 The recurrence rate has been reported to be approximately 26.1%. 26 Treatment for spondylolysis typically involves wearing an orthosis combined with rest and gradual reintroduction to athletic activities. To ensure bone union, which is the ultimate goal of treatment, prolonged treatment duration may be necessary, typically for 1–6 months, even if the pain disappears.25–27 In contrast, in our cases involving apophyseal injury to the L5 transverse process, symptom improvement was achieved with approximately 4 weeks of rest without the application of lumbar orthosis. Both patients were able to return to sports activities early without experiencing any recurrence of symptoms or decline in performance. In Case 2, MRI was performed, and the findings at 3 months post-injury were favorable. The precise duration required to achieve bone healing in apophyseal injuries to the L5 transverse process and long-term outcomes remain uncertain owing to the limited number of cases; thus, further accumulation and analysis are essential. Moreover, there have been reports linking core muscle activity to LBP in athletes performing jumping movements, 28 suggesting that early rehabilitation targeting core muscle activation may have contributed to early symptom improvement in both cases.
Conclusion
We presented two cases of adolescent athletes with unilateral LBP due to L5 transverse process apophyseal injuries. Attachment of the iliolumbar ligament to the L5 transverse process is presumed to have caused apophyseal injury due to traction on the ligament. A differential diagnosis from spondylolysis and L5 transverse process apophyseal injuries is crucial for identifying the cause of LBP in adolescent athletes. The two conditions share many similarities in physical findings, making differentiation challenging; therefore, imaging studies, such as CT and MRI, are useful for diagnosis. Apophyseal injury in the L5 transverse process may have a relatively favorable prognosis in the early to mid-term, and patients could return to sports earlier than those with lumbar spondylolysis do.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504251344840 - Supplemental material for Apophyseal injury of the fifth lumbar transverse process in adolescent athletes: A report of two cases
Supplemental material, sj-pdf-1-sci-10.1177_00368504251344840 for Apophyseal injury of the fifth lumbar transverse process in adolescent athletes: A report of two cases by Yuya Fukuda, Kinshi Kato, Kenichi Otoshi, Takuya Nikaido, Michiyuki Hakozaki, Yoichi Kaneuchi and Yoshihiro Matsumoto in Science Progress
Footnotes
Abbreviations
Author contributions
Conceptualization, K.K. and Y.F.; investigation, K.K.; writing—original draft preparation, K.K. and Y.F.; writing—review and editing, K.O., T.N., M.H., Y.K., and Y.M.; supervision, K.K. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Data availability statement
Data sharing does not apply to this study because no datasets were generated or analyzed in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.