
Abstract
Objective
This study employed data derived from a nationally representative panel survey to investigate the impact of comorbidities on the health-related quality of life (HRQoL) of individuals living with diabetes mellitus.
Methods
A retrospective, cross-sectional, population-based analysis was conducted using data from 10,049 participants in the Korea Health Panel Survey (KHPS) in 2020. The participants were divided into three groups: individuals without diabetes, individuals with diabetes only, and individuals with diabetes and comorbidities. HRQoL was assessed using the European Quality of Life—5 Dimensions (EQ-5D) tool. Multiple regression analyses were performed to examine the contribution of comorbidities to HRQoL scores.
Results
Comorbidities were associated with lower scores in physiological, psychological, and overall HRQoL. A significant reduction in HRQoL was observed with comorbidities, and a negative association was established between the number of comorbidities and physiological and overall HRQoL (P < .001). Demographic factors such as age, education, and disability significantly influenced HRQoL. In addition, psychological factors such as high stress had a substantial impact on HRQoL, particularly in individuals with diabetes and comorbidities (P < .01).
Conclusion
Comorbidities considerably impair HRQoL among patients with diabetes. Health providers should consider the presence of comorbidities and diseases in diabetes when developing intervention methods to effectively manage diabetes and patients’ well-being.
Introduction
Diabetes mellitus (DM) is a chronic metabolic disease characterized by persistently elevated blood sugar levels, which, over time, lead to severe damage to the nerves, blood vessels, kidneys, eyes, and heart. The global spread of DM is increasing, and consequently, it is a major public health issue and a leading cause of death and disability. 1 In 2019, DM and its complications caused up to 4.2 million deaths, estimated to constitute approximately 11.3% of all deaths worldwide. 2 Additionally, DM has contributed substantially to the global disability burden, with 67.9 million disability-adjusted life years (DALYs) reported in 2017. 3 These statistics demonstrate the substantial and devastating impact of DM on global public health.
According to the 10th edition of the International Diabetes Federation (IDF) Diabetes Atlas (2021), approximately 1 in 11 adults (90 million people) in Southeast Asia are living with diabetes. 4 This figure is projected to rise to 113 million by 2030 and 151 million by 2045. In Korea and many other countries, DM has become a major public health concern, affecting a substantial portion of the population and significantly burdening the healthcare system. According to research, 16.7% of Korean adults (aged >30 years), or approximately 6.05 million individuals, were living with DM in 2020. 5 Patients with DM represented 13.8% of the adult Korean population (aged >30 years) in 2018, and 10.7% of the total population in 2017. 6 These figures demonstrate the significant and growing impact of diabetes in South Korea and emphasizes the need for efficient strategies to control and prevent this disease.
A clear understanding of how DM influences the quality of life within the Korean healthcare system is crucial to developing effective policies and interventions. Research on health-related quality of life (HRQoL) has gained prominence in healthcare, particularly in individuals with DM. HRQoL assessment is not limited to physical dimensions; it also evaluates patients’ psychological, social, and emotional well-being. 7 Previous research has found a significant relationship between diminished HRQoL and DM. For instance, individuals with DM exhibit lower HRQoL than those without the condition. 8 Another study reported a correlation between DM and lower HRQoL, particularly in physical functioning and mental well-being domains. 9 Moreover, research conducted in a specific population in Korea also confirmed that DM had a detrimental effect on HRQoL. 10 For individuals with chronic conditions such as DM, HRQoL metrics provide invaluable insights into the extent to which the disease and its management affect their daily lives and overall well-being.
Numerous articles and reviews have examined various aspects of DM, including epidemiology, complications, and treatment strategies; however, research specifically focusing on the impact of comorbidities in HRQoL is scarce. Moreover, no studies have assessed how comorbidities in individuals with diabetes affect HRQoL within a representative Korean population using an HRQoL instrument that has been validated and found reliable for use in Korea. Comorbidities, such as hypertension and ischemic heart disease, are prevalent among individuals with type 2 DM and have been associated with a decline in HRQoL. 11 Understanding the correlation between comorbidities and HRQoL is essential for developing tailored interventions that address the complex needs of patients with DM and multiple health conditions. Consequently, further research in this area is still needed. We used data from the Korean Health Panel Study (KHPS) to fill the evidence gap in this field. The KHPS incorporates varied demographics within the sample to facilitate the comparison and comprehensive analysis of subgroups, which aids in comprehending the complex, multifaceted factors that influence health and developing robust solutions supported by evidence. In addition, longitudinal panel data allows researchers to scrutinize changes over longer periods, circumventing the limitations of cross-sectional data. Therefore, this study investigated the impact of comorbidities on the HRQoL of individuals with DM, ultimately informing effective healthcare strategies.
Methods
Study design
This study employed a retrospective, cross-sectional, population-based analysis design based on secondary data from 10,049 participants in the Korea Health Panel Survey (KHPS).
Data source
The KHPS is a collaborative survey conducted by the Korea Institute of Health and Social Affairs and the National Health Insurance Service. The survey results are used in healthcare and health insurance policymaking, particularly in assessing medical expenditure and healthcare costs. The survey is conducted using computer-assisted personal interviewing (CAPI) in each region, and appointed surveyors receive training on the survey content and guidelines. Panel households must maintain a household health account book to record annual medical expenditures systematically, thus ensuring accuracy in reporting medical expenditures. 12
The KHPS primarily focuses on gathering data related to social characteristics, income and expenditure status, general medical expenses, medical service utilization, and the health insurance status of households and individual members. 13 Additionally, the survey includes information on chronic disease management, overall health status, medical accessibility, and household members’ lifestyles. The relevant institutional review board has ethically approved the survey process, and all participants provide their data and informed consent either verbally or in writing.
This study utilized baseline data from the KHPS in 2020, initially involving 14,844 respondents. Individuals under 19 years old, those with missing data, and individuals with a history of malignancy were excluded, as malignancies significantly impact quality of life. Consequently, 10,049 respondents (4412 men and 5637 women) were included and analyzed from the baseline data of 2020.
Description of variables
Independent variables
This study aimed to examine the impact of comorbidities on HRQoL. The longitudinal analysis utilized the International Classification of Diseases, 10th Revision (ICD-10), to identify the type of chronic disease among survey participants. From the KHPS dataset, respondents diagnosed with diabetes were selected according to ICD-10 codes E10–E14. 14 To ensure unbiased estimates of the impact of comorbidities on HRQoL outcomes, participants were divided into the following groups: individuals without DM, those with DM only, and those with DM with comorbidities. The comorbid diseases included hypertension, knee osteoarthritis, intervertebral disc disease (IVDD), cerebral infarction, angina pectoris, depression, myocardial infarction, hypothyroidism, asthma, rheumatoid arthritis, chronic hepatitis, dementia, hyperthyroidism, intracranial hemorrhage (ICH), chronic renal failure, chronic obstructive pulmonary disease (COPD), bronchiectasis, and emphysema. The 10,449 respondents were divided into 8581 respondents without diabetes, 460 respondents with DM only, and 1008 respondents with DM with comorbidities. Furthermore, participants with DM and comorbidities were further divided into subgroups according to the number of comorbidities: one comorbidity, two comorbidities, and more than or equal to three comorbidities.
Health-related quality of life (HRQoL)
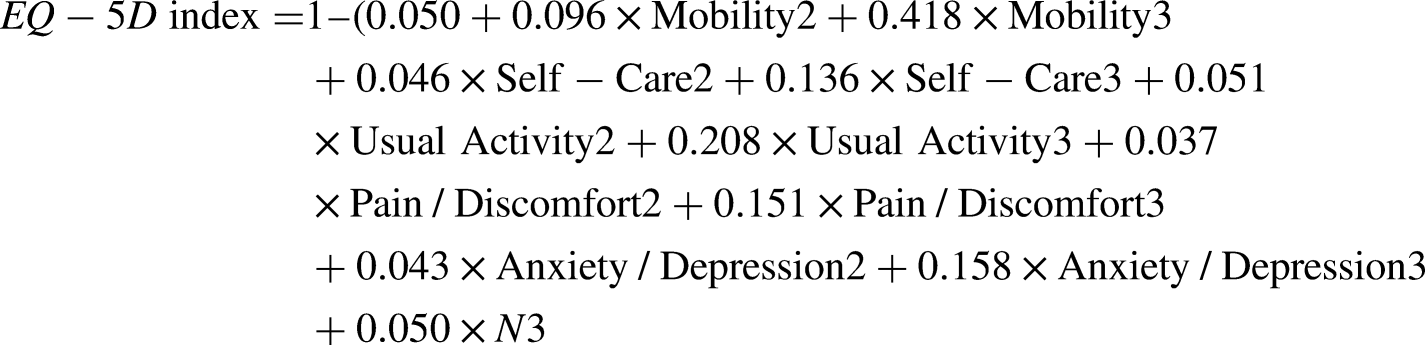
The self-reported European Quality of Life scale with five dimensions (EQ-5D) was used to measure HRQoL. This instrument measures five dimensions of HRQoL, including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is measured using a three-point scale of severity: level 1—no problem, level 2—some or moderate problems, and level 3—serious problems.
15
The overall HRQoL score in this survey was calculated using a formula developed by the Korea Centers for Disease Control and Prevention, according to which a minimum score of −0.171 indicates poor health and a score close to 1 indicates minimal health-related issues across the five dimensions.
16
The formula is as follows:
Covariates
All regression models accounted for and adjusted potential confounding factors affecting HRQoL. After reviewing the literature comprehensively, the following covariates were selected: socio-demographic characteristics, encompassing various aspects of demographic status (gender, age, education, economic status, and family composition), functional status (disability status and regular exercise), physical status (BMI), health behavior (smoking and drinking), mental health (stress about disease, thought of suicide), and health perception (subjective health status).10,17,18 These variables could potentially influence EQ-5D and were thus adjusted for in all regression models to minimize bias and better estimate the relationship between comorbidities and HRQoL across all regression models.
Participants aged between 20 and 101 years were grouped into two categories: <50 years and >50 years. Initially measured on a 6-point Likert scale, education level was categorized into two groups: high school or lower and college or higher. Similarly, economic status, initially assessed on a 7-point Likert scale, was simplified into employed and unemployed categories. Family composition was categorized as “living alone” and “living with others” according to the responses to the question regarding household cohabitation. Disability status was dichotomized into disabled and non-disabled. Regular exercise was determined by responses to the question about self-reported engagement in regular exercising routine over the past year, categorized as “yes” or “no.”
The body mass index (BMI) was calculated using height and weight measurements. Participants with a BMI of >25 were categorized as obese, according to the Korean Society for Obesity Studies. 19 Smoking status was identified through responses to inquiries about current smoking habits; participants were categorized as “ex/current smoker” or “never smoked.” Alcohol consumption was assessed via drinking frequency in the past year; participants were categorized as “never drinking” or “drinking.” Stress levels were gauged using the questions regarding the stress level experienced in daily life, with responses indicating high stress categorized as “yes” and those indicating low stress as “no.” Finally, subjective health status was categorized as “poor” or “fair/good” according to participants’ self-assessed general health.
Data analysis
This study used IBM SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA). A p-value of <0.05 indicated statistical significance. To analyze the DM group's general characteristics, lifestyle habits, and mental health status, categorical variables were presented as frequencies and percentages, and the Chi-squared test was used to compare the baseline characteristics of DM only and DM with comorbidities groups. Regression estimates and 95% CIs were reported to analyze the effects of the number of comorbidities on HRQoL, representing the average difference in HRQoL for each additional comorbidity in the DM-with-comorbidities group compared with the DM-only group as the reference. Multivariate analysis using multiple linear regression was used to estimate the influence of DM only and DM with comorbidities on HRQoL before and after adjustment for covariates and determine the predictive factors that independently influenced HRQoL.
Ethical statements
This study was conducted in accordance with the Declaration of Helsinki and adhered to ethical standards for studies involving human subjects. The Korea Health Panel Survey data used in this study are statistical data designated by the government under Article 18 of the Statistics Act. 20 Since the Korea Health Panel Survey data are openly published 12 ; hence, ethical approval was not required for this study. This study did not require informed consent from the participants, as their information was fully anonymized and unidentified before analysis. In addition, personal information cannot be used to identify individuals and is fully protected in compliance with Articles 33 and 34 of the Statistics Act. Before participating in the KHPS, respondents were provided with a detailed explanation of the study's purpose and methodology and were also asked to read and sign an agreement form, providing consent to use their data in future scientific research. All participants in this study received sufficient explanation about how to use the questionnaire, provided written consent, and then completed the questionnaire. This study did not include minors.
Results
Background characteristics of study participants
Of the 10,049 respondents, mostly were female, aged >50 years, and had a level of education below a college degree. In addition, the members of each group generally lived with other people and were employed. In contrast to patients with diabetes and comorbidities, only a small number of the DM-only group had a disability (P = .025). The DM-only group exercised more than individuals with DM and comorbidities (58.9 vs. 47.0%); however, in the group without DM, the proportion of those who exercised regularly and those who did not exercise regularly was approximately equal (50.4% vs. 49.6%).
Across all groups, most participants were not obese according to their BMI category. Data regarding smoking status also showed that participants generally did not smoke. Nevertheless, the proportion of participants who drank alcohol was higher in the DM-with-comorbidities and DM-only groups compared with the group without DM. The variables reflecting the mental state of the respondents showed that they generally did not experience high levels of stress and exhibited few symptoms of depression, anxiety, or suicidal thoughts (all P < .05) (Table 1).
The demographic and other characteristics of participants at baseline (n = 10,049

The P-value is the chi-square test result. BMI, body mass index.
Influence of comorbidities on HRQoL
The impact of comorbidities on the HRQoL dimension scores of individuals with diabetes, before and after adjustment, is presented in Table 2. Subjects with DM only and DM with comorbidities reported lower unadjusted HRQoL than subjects without DM, with score reductions of −0.04 and −0.12 points, respectively. After adjusting for known determinants of HRQoL, the effect sizes of DM only and DM and comorbidities on HRQoL were −0.01 and −0.08, respectively. The impact was statistically significant for DM only, which impaired mobility, usual activities, and pain/discomfort. On the other hand, diabetes with comorbidities impaired mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (Table 2).
Effects of eq-5D scales by disease groups.

The analysis was conducted to explore statistically different from the group with or without DM (P < .05) based on a 95% confidence interval for the difference between groups.
Multiple linear regression, adjusted for the influence of gender, age, education, economic status, family composition, disability status, and regular exercise. BMI, smoking, drinking, high stress, thoughts of suicide, and subjective health status. SD, standard deviation. DM, diabetes mellitus. BMI, body mass index.
*p < .05.
**p < .01.
***p < .001.
Linear regression analysis of the impact of total comorbidities on each HRQoL dimension showed a significant difference between the DM-only group and the group with diabetes with one comorbidity. However, the group with diabetes with two comorbidities had a significantly reduced HRQoL (−0.04 (95% CI: −0.09, −0.01)) compared with the DM-only group. These patients also exhibited significantly lower scores on self-care (−0.05 (95% CI: −0.08, 0.02)), pain/discomfort (0.07 (95% CI: −0.04, 0.03)), and anxiety/depression (−0.02 (95% CI: −0.03, 0.01)) dimensions compared with the DM-only group. Furthermore, the DM group with three or more comorbidities also experienced the greatest reduction in HRQoL (−0.10 (95% CI: −0.12, −0.00)) compared with the DM-only group. This decrease was statistically and clinically significant and clinically important, signifying the profound effect of multiple comorbidities on overall well-being. All five dimensions of HRQoL were also substantially impacted by comorbidities (Table 3).
The impacts of total number of comorbidities on diabetes with comorbidities and HRQoL dimension (n = 1468).

Data are presented as mean difference (95% CI). The reported β-coefficients of each category of comorbidity status represent average difference in HRQoL scores of each diabetes with comorbidities compared with the reference (DM only). Regression were adjusted by gender, age, education, economic status, family composition, disability status, regular exercise, BMI, smoking, drinking, high stress, thought of suicide and subjective health status. HRQoL: health-related quality of life.
p < .05.
p < .01.
p < .001.
Descriptive of HRQoL dimensions and prevalence of comorbidities
The descriptive analysis of each HRQoL dimension revealed that both the diabetes-only group and the group without diabetes generally reported no issues with mobility, self-care, usual activities, pain/discomfort, or anxiety/depression. The diabetes-with-comorbidities group exhibited comparable results, except for the pain/discomfort dimension, for which a higher proportion reported experiencing problems. Specifically, 53.3% of respondents reported some problems, and 3.9% reported severe pain in this dimension, with an average score of 0.69 ± 0.28. The most frequent comorbid conditions prevalent among participants were hypertension (38.27%), knee osteoarthritis (18.79%), intervertebral disc disease (18.71%), and depression/bipolar disorder (3.24%). Emphysema was the least common comorbidity among patients with diabetes, impacting only 0.13% of patients with diabetes (Figures 1 and 2).
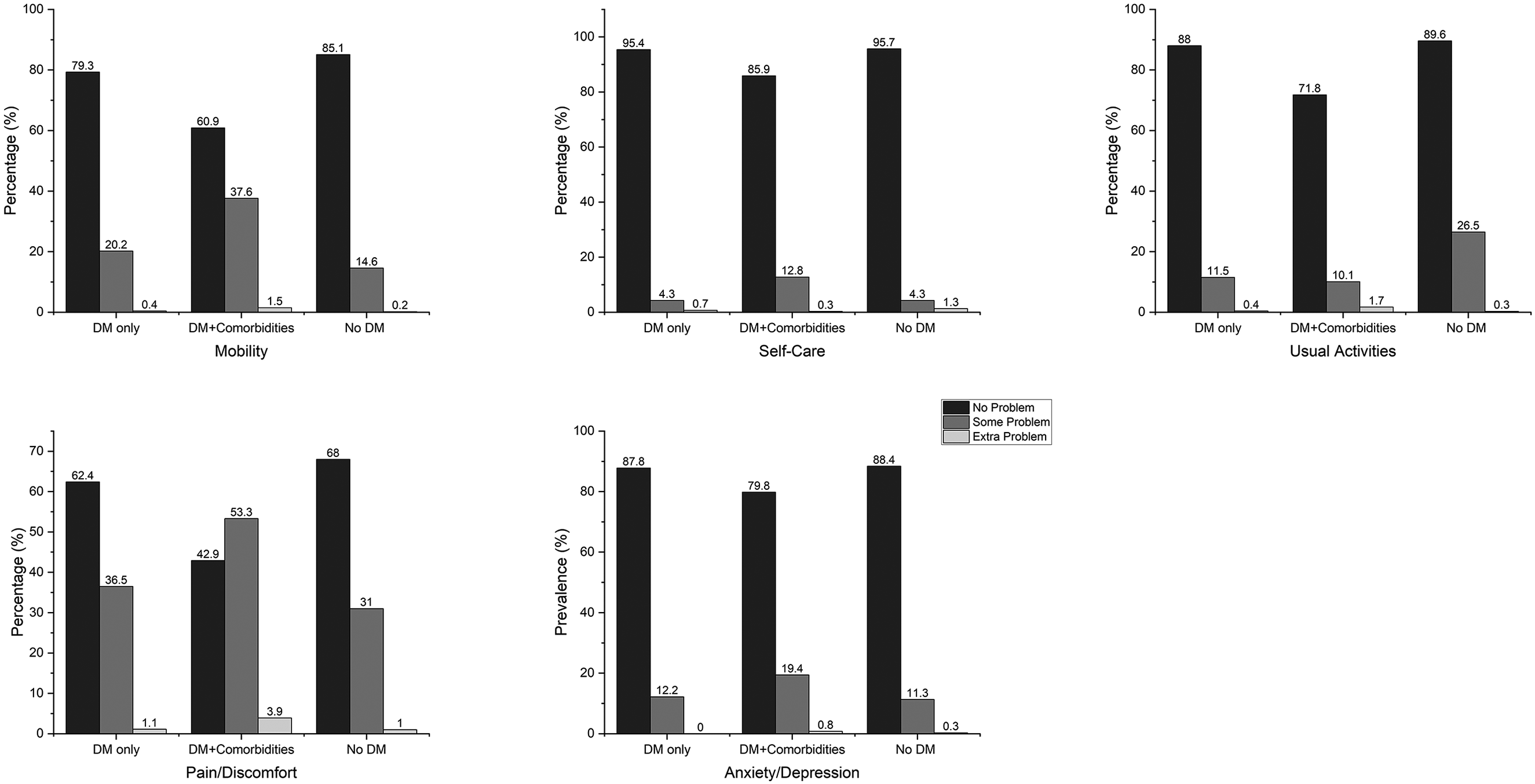
Distribution of perceived problem levels in each of the dimensions of the eq-5D.

Prevalence of comorbidities.
Factors influencing HRQoL
Table 4 presents the findings of a multivariate regression analysis that identifies key factors associated with HRQoL among individuals with diabetes mellitus and comorbidities in Korea. The analysis revealed that higher education levels, the absence of disabilities, and low stress levels were positively correlated with both physiological and psychological well-being, leading to an overall enhancement in quality of life. Conversely, individuals aged 50 years or older exhibited a negative association with both physiological (Coefficient = −3.42; 95% CI: −11.71, −4.54, P < .01) and psychological scores (Coefficient = −4.06; 95% CI: −8.26, −4.10, P < .01), resulting in poorer overall quality of life (Coefficient = −4.10; 95% CI: −10.42, −3.76, P < .01). Additionally, the analysis indicated no significant relationship between HRQoL outcomes and poor subjective health status, suicidal ideation, or obesity. Table 4 further illustrates that individuals with diabetes who did not have comorbidities reported significantly better quality of life than those with one or more comorbid conditions. This trend underscores the detrimental impact of comorbidities on physiological, psychological, and overall quality of life metrics. These findings align with the existing literature that emphasizes the negative correlation between comorbid conditions and HRQoL among patients with diabetes, suggesting that as the number of comorbidities increases, physical and mental health scores significantly decline (Table 4).
Factors associated with HRQoL among diabetic patients with comorbidities.

b = Standardized regression coefficients. MO, mobility; SC, self-care; UA, usual activities; PD, pain/discomfort; AD, anxiety/depression; CI, confidence interval; BMI, body mass index.
p < .05.
p < .01.
p < .001.
Discussion
Our findings show that DM significantly impacts HRQoL in the Korean population. The results of this study also demonstrate that individuals with DM with comorbidities have lower HRQoL than those with DM without comorbidities. An age of ≥50 years, higher education levels, the absence of disability, high-stress levels, and the presence of comorbidities were significantly associated with the overall quality of life.
The prevalence of smoking was less in the DM-with-comorbidities group than in the other groups. When examining the relationship between smoking, alcohol drinking, and DM, it is crucial to consider the significant impact of these behaviors on the management and complications of DM. Prior research has identified smoking as a significant risk factor for the emergence of type 2 DM and the exacerbation of microvascular and macrovascular complications. 21 Similarly, alcohol consumption has been linked to poorer adherence to DM care regimens and an increased risk of chronic inflammation of the pancreas, which can impair insulin secretion and elevate the risk of DM. 22 Moreover, individuals with comorbid conditions, such as DM and cardiovascular disease, may have a heightened awareness of the detrimental effects of smoking and drinking on their health. 23 This increased awareness could contribute to a more proactive approach to modifying these behaviors, resulting in lower prevalence rates within this population.
While analyzing the dimensions of HRQoL using the EQ-5D, we found that diabetes with comorbidities impacted all aspects of quality of life. Contrastingly, individuals with diabetes without comorbidities experienced a similar effect, except in the self-care dimension. This is consistent with a previous systematic review and meta-analysis, which found that comorbidities were associated with a higher burden of disease and a negative impact on various domains of HRQoL, including physical health, psychological well-being, and social relationships. 24 The DM-with-comorbidities group also exhibited greater levels of pain and discomfort. Chronic pain is a common comorbid condition that can be particularly troublesome for patients with DM, given its symptomatic nature. 25 Chronic issues, such as diabetic neuropathy and non-neuropathic pain, rheumatic manifestations, and mental health comorbidities have been associated with greater pain intensity, increased complications, and reduced quality of life in patients with type 2 DM. 26
Numerous factors may have an impact on the HRQoL of a patient with DM. We found that age, a high level of education, the absence of disability, high-stress conditions, and the presence of comorbidities were consistently significant factors influencing physiological and psychological aspects of health-related quality of life. Age was among the most significant predictors of demographic factors, lifestyle choices, and comorbidities (P < .001). Similar results have been observed in European and Asian studies, which have shown an inverse correlation between HRQoL and age. 27 This is particularly relevant because older adults often experience multiple chronic conditions, which can lead to cognitive issues and the need for various medications—factors that significantly deteriorate their physical and mental well-being. 28
This study highlights the impact of educational attainment on HRQoL among individuals with diabetes, showing that those with higher education levels generally report better HRQoL. However, the research findings on this relationship remain inconsistent. For example, a study in Serbia found no significant correlation between education and HRQoL. 29 By contrast, research from the United Kingdom supports the current findings, showing that individuals with over 12 years of education experience improved HRQoL in managing type 2 DM. 30 Higher education levels may provide diabetic patients with better social support, increased self-esteem, and a deeper understanding of disease management, which can promote treatment adherence and ultimately enhance both health outcomes and quality of life. 17
Our results also indicated that disability significantly impacts HRQoL because of the multifaceted barriers that individuals face in their daily lives. People with disabilities often experience limitations in physical functioning, which can lead to decreased participation in social and recreational activities, ultimately affecting their mental and emotional well-being. Individuals with disabilities are more susceptible to chronic diseases and report poorer health outcomes than their non-disabled counterparts, largely because of increased sedentary behavior and physical inactivity.
31
The presence of comorbidities further exacerbates these challenges, as individuals may struggle with the management of multiple health conditions simultaneously, leading to a compounded negative effect on the physical and mental dimensions of HRQoL.
32
These findings underscore the critical importance of addressing these factors when developing strategies to enhance HRQoL among diabetic individuals
In contrast to prior studies, our study showed that gender variables did not significantly affect HRQoL except in the DM with comorbidities group. Several studies have investigated the impact of gender on HRQoL in patients with DM.33,34 Some have found that women with DM experience worse HRQoL, particularly regarding mental well-being, as compared to men. Likewise, other studies have reported that gender does not have a significant effect on changes in HRQoL. 35 Similarly, a systematic review of factors predictive of HRQoL among adults with type 2 DM found that gender did not consistently predict HRQoL. 36 The influence of gender on HRQoL in patients with DM appears to be multifaceted and may vary across different populations and study settings. A complex interplay of biological, psychological, social, and cultural factors may contribute to the varying impact of gender on HRQoL observed in patients with DM.
Lastly, factors such as high-stress levels emerged as a significant determinant of HRQoL through various physiological and psychological mechanisms, as evidenced by numerous studies and systematic reviews. Meta-analyses have indicated that chronic stress adversely impacts multiple domains of HRQoL, including physical, mental, and social well-being. 37 Chronic stress activates the hypothalamic–pituitary–adrenal (HPA) axis, leading to increased cortisol production, which can result in cognitive impairments and mood disorders such as anxiety and depression. 38 These psychological conditions are negatively correlated with HRQoL scores, demonstrating that individuals experiencing high stress report lower quality of life across various measures. Furthermore, stressful life events not only exacerbate existing health issues but also contribute to the development of new ones, such as cardiovascular diseases and metabolic syndromes, further reducing HRQoL. 39
This study has several limitations. First, DM status in the KHPS was determined via a self-reported questionnaire, potentially introducing recall bias and impacting the reliability of the data. Therefore, future studies should use other standardized objective measurements (for example, HBA1C values and fasting blood sugar) to accurately diagnose DM within the sample. Second, not all diabetic complications were assessed because of limitations in the survey used, which may have prevented a comprehensive understanding of the impact of DM with comorbidities on HRQoL. Additionally, the study was conducted at a single time point and may have thus overlooked fluctuations in HRQoL over time. As a cross-sectional study, the observed associations do not imply causation. This study also has several strengths. First, it utilized data from a nationwide population with a high response rate, offering representative insights into the Korean population. In addition, the study controlled for other comorbidities by categorizing participants into distinct groups comprising individuals with DM only, those with DM with comorbidities, and those without DM to offer clear insights into HRQoL levels according to diabetes status. This approach enhances the study's credibility and relevance by providing comprehensive information regarding public health strategies and informing interventions targeting the impact of DM on the quality of life in South Korea.
Conclusion
In conclusion, the study's findings reveal that comorbidities in DM are significantly associated with worse HRQoL. The analysis of EQ-5D scores by dimension indicated that individuals with DM and comorbidities experienced more issues in the pain/discomfort dimension. Additionally, demographic variables, such as age, education, disability, and high stress levels, were significant risk factors for HRQoL. Our findings suggest that interventions targeting psychological well-being and promoting healthy lifestyle behaviors could benefit individuals with DM with comorbidities by improving their HRQoL. These results emphasize the importance of comprehensive care that addresses both physical and psychological aspects to enhance the overall well-being of individuals with DM and related comorbidities. Finally, a comprehensive, patient-centered approach to diabetes care that incorporates both medical and psychological assistance is critical for enhancing the overall well-being of this group.
Footnotes
List of abbreviations
Author contributions
K-SH designed research projects and methodologies, reviewed, and revised the final version of the manuscript. DP performed data analysis, interpreted the data, and drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The data presented in this study is provided at the request of the author and is not disclosed for privacy purposes, available at ![]() (accessed March 24, 2024. When publishing research results to use Korean Health Panel Survey data, researchers clearly explain the data management organization, name, and version of the data and adhere to the conditions that the data will only be used for research purposes and will not be lent or transferred to others. The data was provided by the Korean Medical Panel data manager after sending an email (khp@kihasa.re.kr) with a data use consent form with the requirement of complying with established regulations.
(accessed March 24, 2024. When publishing research results to use Korean Health Panel Survey data, researchers clearly explain the data management organization, name, and version of the data and adhere to the conditions that the data will only be used for research purposes and will not be lent or transferred to others. The data was provided by the Korean Medical Panel data manager after sending an email (khp@kihasa.re.kr) with a data use consent form with the requirement of complying with established regulations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The Korea Health Panel Survey (KHPS) data was published openly. Therefore, ethical approval was not required for this study. This study did not require informed consent from the participants, as their information was fully anonymized and unidentified before analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.