
Abstract
Venereal syphilis, caused by Treponema pallidum, is a major global health problem. Untreated latent syphilis can progress to tertiary syphilis, often leading to severe complications such as cardiac involvement, particularly syphilitic aortitis, which may manifest decades after the initial infection. We present a case of a 46-year-old woman who developed an ascending aortic aneurysm and severe aortic valve insufficiency due to late-stage syphilis. She presented with bilateral lower limb edema, intermittent chest pain, decreased functional capacity, and dyspnea, ultimately requiring hospitalization for cardiogenic shock. Diagnostic imaging revealed significant aortic valve damage and aneurysmal dilation of the ascending aorta, while serological tests confirmed tertiary cardiovascular syphilis. Surgical intervention involved the reconstruction of the ascending aorta and replacement of the aortic valve with a bioprosthetic valve. Histopathological analysis indicated chronic endocarditis. Postoperative management included intensive care support and antibiotic treatment. The patient demonstrated satisfactory recovery, with no further complications reported at the 3-month follow-up.
Introduction
Venereal syphilis, caused by the bacterium Treponema pallidum (Tp), is a complex, multistage illness characterized by a range of clinical manifestations. 1 Syphilis stands as a significant global concern in the realm of sexually transmitted diseases. 1 In 2019, the global prevalence of syphilis reached 49.71 million cases, with Colombia reporting an incidence of approximately 196 cases per 100,000 individuals.2–4 Among patients with latent syphilis left untreated, 70% remain asymptomatic while 30% progress to tertiary syphilis.4–7 Within this group, 10% eventually experience cardiac complications, notably syphilitic aortitis, which typically manifests 20 to 30 years post-primary infection.1,4,5
Cardiovascular syphilis typically manifests in the fourth or fifth decade of life and presents various complications, such as uncomplicated syphilitic aortitis, syphilitic aortic aneurysm, syphilitic aortic valvulitis with regurgitation, and syphilitic coronary ostial stenosis.5–9 The low diagnostic frequency and suboptimal treatment may increase the incidence of associated cardiovascular complications.5,6 Observational studies describe that the most affected aortic segments are the ascending portion, the aortic arch, and the descending portion.8–10
This rare cardiovascular complication often presents with ascending aortic aneurysm and, less frequently, aortic insufficiency.1,6,10–12 Herein, we present a case study of a woman patient afflicted with an ascending aortic aneurysm and severe aortic valve insufficiency stemming from late-stage syphilis, necessitating reconstruction of the ascending aorta and replacement with a biological aortic valve.
Case report
A 46-year-old woman was admitted in October 2022 to Fundación Clínica Shaio. She presented to the emergency department with a spectrum of symptoms, including bilateral lower limb edema persisting for 50 days, intermittent self-resolving chest pain, decreased functional capacity even with minimal exertion, and episodes of paroxysmal nocturnal dyspnea. Her medical history revealed prior tobacco, marijuana, and cocaine use, which ceased 5 years prior, as well as a previous occupation as a sex worker, transitioning to a stylist over the last decade. Upon admission, she presented with hypotension, desaturation, and dyspnea. Clinical examination revealed a mesodiastolic grade IV/VI murmur at the aortic focus, jugular venous distension graded at 2, and lower limb edema.
Transthoracic and transesophageal echocardiograms unveiled significant aortic valve damage potentially stemming from previous endocarditis, along with aneurysmal dilation of the ascending aorta, valvular heart disease, and generalized hypokinesia, resulting in an ejection fraction of 41% (Figure 1). The right ventricle maintained normal size and preserved function, with a shortening fraction of 42%. Furthermore, contrast chest angiotomography demonstrated ectasia of the ascending aorta with a diameter of 56 mm, indicative of a fusiform aneurysm (Figure 2). Suspecting infective endocarditis, blood cultures were obtained, alongside serological testing for human immunodeficiency virus, hepatitis, and serial bacilloscopy, all of which returned negative results. However, venereal disease research laboratory and rapid plasma reagin tests yielded positive results for antibodies against Tp, with dilutions of 1:32 and 1:64, respectively, confirming a diagnosis of tertiary cardiovascular syphilis. A cerebrospinal fluid study ruled out neurosyphilis.
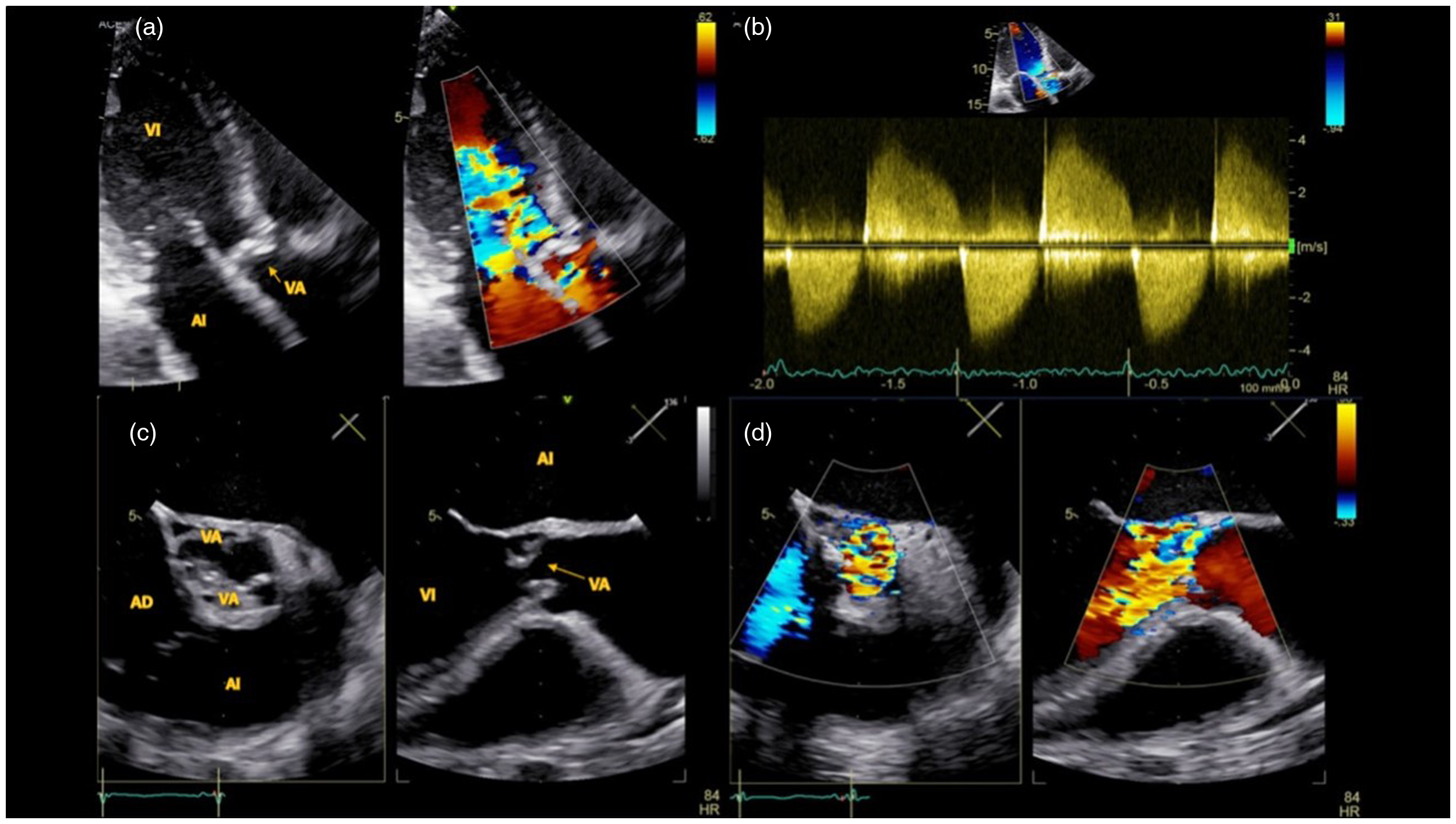
Transthoracic and transesophageal echocardiogram in diastole.

Three-dimensional reconstruction from tomography.
The patient was admitted to the intensive care unit due to cardiogenic shock that required vasopressor and inotropic support, and initial empirical antibiotic treatment of infective endocarditis was started with ampicillin combined with ceftriaxone. Once hemodynamic stabilization was achieved without the need for vasopressor support, a surgical replacement of the aortic valve and ascending aorta was performed. The procedure was carried out via median sternotomy using hypothermic cardiopulmonary bypass with cannulation through the femoral artery and central bicaval cannulation. During the surgery, an aneurysmal dilation from the sinotubular junction to the aortic isthmus was identified, along with severe aortic valve insufficiency attributable to scar-related endocarditis and a drained abscess with scarring beneath the non-coronary sinus. The surgical procedure involved the replacement of the aortic valve with a 28-mm Ultra Mosaic bioprosthetic valve and the aortic root. The ascending aorta was replaced using a 32-mm Gelweave graft. In addition, the supra-arch vessels were reconstructed during operation. This included careful reconnection to ensure adequate blood flow after surgery. Histopathological examination of the aortic aneurysm showed chronic inflammatory involvement of the adventitia, the media, the vasa vasorum, and the aortic valve, suggesting chronic endocarditis with scarring and acute components (Figure 3).
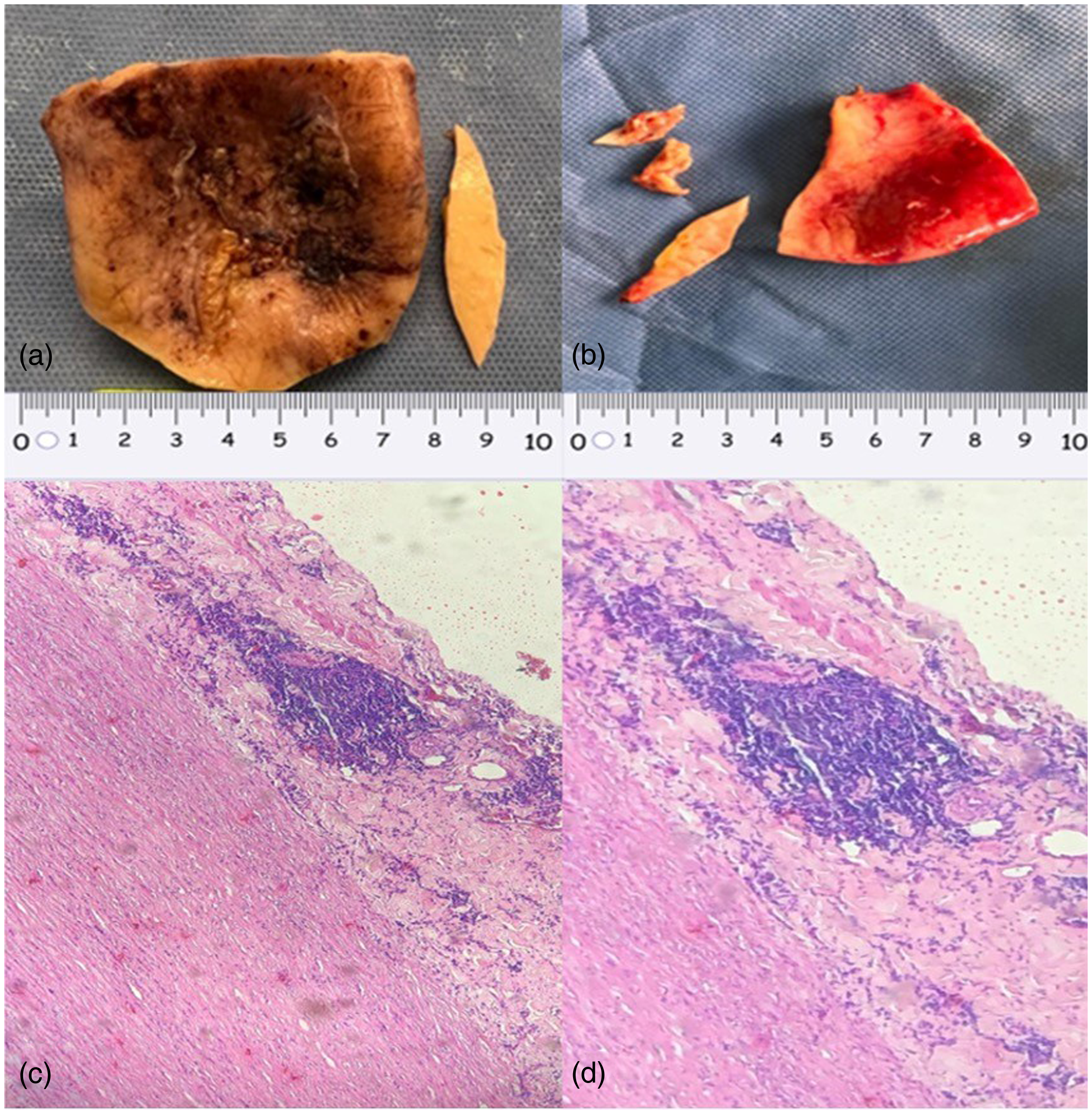
Macroscopic and microscopic vascular lesion.
Postoperatively, the patient required cardiovascular intensive care unit management, including vasopressor and mechanical ventilation support for 7 days, followed by an uncomplicated hospitalization and a 3-week course of benzathine penicillin G 6000000 IU per day intravenously based on current guidelines and literature.13–15 A telephone follow-up at 3 months post-discharge indicated satisfactory progress with no additional hospitalizations required. Additionally, we were unable to obtain further information or follow-up imaging studies, as the patient did not attend her scheduled infectious disease follow-up appointments. Finally, informed consent has been obtained from the patient for publication of the case report and accompanying images (Supplementary File). Ethical approval by a research ethics committee was not required. The reporting of this study conforms to CARE guidelines (Supplementary File). 16
Discussion
In our case, we described a 46-year-old woman with a history of substance use and a previous occupation as a sex worker, presenting symptoms suggestive of cardiovascular disease. Diagnostic testing revealed significant aortic valve damage, aneurysmal dilation of the ascending aorta, and positive serologic testing for syphilis, confirming the diagnosis of tertiary cardiovascular syphilis. Surgical intervention, including replacement of the aortic valve and ascending aorta, was necessary. Postoperatively, she required intensive care but ultimately showed satisfactory progress with no further hospitalizations at a 3-month follow-up.
Before the advent of antibiotic treatments prior to 1940, syphilitic aortitis accounted for a significant portion of heart disease cases in individuals aged over 50.17–19 The incidence of syphilitic aortitis during this period varied between 5% and 30%, with fluctuations attributed to economic, racial, and geographical factors.5–7 Presently, syphilitic aortitis is a rare cardiovascular complication capable of causing aneurysms in the ascending aorta and aortic insufficiency. In the case presented, syphilis infection was confirmed as the cause of aortitis through serological and histological findings, along with a favorable clinical response to medical and surgical treatment.6,7,18
Infectious aortitis, previously termed as a mycotic aneurysm, refers to the inflammatory involvement of any segment of the aorta.12,18,20 The mechanisms of infection can occur through contiguous spread, septic embolism, or hematogenous dissemination to the aortic wall via a vulnerable plaque or preexisting aneurysm.1,2,5 The primary agents identified include Staphylococcus aureus, Pneumococcus, Escherichia coli, and Salmonella.7,8 However, the resurgence of sexually transmitted infections underscores syphilis as a potential differential diagnosis, even in the absence of immunosuppression. 9 The natural progression of treated and untreated syphilis is unpredictable. Following initial infection, Tp proliferates in the aortic wall and then spreads into the lymphatic vessels, particularly abundant in the thoracic aorta, explaining the bacterium's affinity for this segment. In cases of untreated chronic infection, plasmacytes and lymphocytes induced by the immune response cause diffuse thickening of the intima.10,20
In the contemporary medical landscape, diagnosing syphilitic aortitis can present significant challenges.3,6,7 Unlike some medical conditions with distinctive symptoms, syphilitic aortitis lacks pathognomonic signs, complicating identification solely based on clinical presentation. Moreover, its echocardiographic findings may mimic those of other cardiac conditions, such as rheumatic valve disease or atherosclerotic disease, potentially leading to misdiagnosis. Presentations may range from asymptomatic to acute. 11 Acute aortic syndrome constitutes a medical emergency characterized by compromised integrity of the aortic wall and an increased risk of rupture.8,10,11 In the described case, transesophageal echocardiography and computed tomography were utilized to document severe aortic insufficiency, eccentric left ventricular hypertrophy, and aneurysms of the proximal, ascending, and aortic arch.
A case series of autopsies conducted between 1950 and 1960 on 100 patients with aortitis described chronically inflamed mesoaortitis with patchy destruction of musculoelastic medial tissue and replacement by connective tissue, accompanied by evidence of endarteritis obliterans of the vasa vasorum. 12 Moreover, among patients with syphilitic aortitis, 50% of aortic aneurysms developed in the ascending aorta, 35% in the aortic arch, and 15% in the descending aorta. 12 In our patient, the principal involvement was aortic insufficiency and the ascending aorta, with histological findings confirming syphilitic aortitis and chronic endocarditis on the aortic valve, along with an acute superimposed component, suggesting chronic syphilitic injury potentially predisposing to a coinfection not identified by blood or tissue cultures.6,7,12,17–20
We delineate several risk factors implicated in the resurgence of syphilis in a transgender woman with low socioeconomic status, psychoactive substance use, and engagement in sex work.3,5,6 Despite the availability of diagnostic tests and the efficacy of long-acting penicillin treatment, the incidence has surged by over 150% in the past decade, with an estimated 6.3 million cases annually worldwide, posing a significant public health challenge.8–11 This infection predominantly affects men in 82% of cases, with identified risk factors including sexual relations with same-sex partners and coinfection with human immunodeficiency virus in 41%.2,7
The medical management of infectious aortitis entails antibiotic therapy. In most scenarios, blood cultures and cultures of surgical specimens yield negative results, necessitating the choice and duration of treatment to be guided by the clinical context. For suspected bacterial infections, a treatment duration of 6 weeks to 6 months is recommended, with chronic suppressive therapy advised in select cases.3,6,7,17 In the described case, central nervous system involvement was excluded, and there was no documented evidence of infection by other microorganisms, warranting treatment for tertiary syphilis with crystalline penicillin. The low levels of treponemal deoxyribonucleic acid in clinical samples and the inherent challenges in culturing render identification difficult.6,8,10 However, antibiotic therapy alone does not curtail the expansion rate of the aneurysm or prevent rupture, necessitating intervention. Open surgical repair is the preferred technique, with expert recommendations estimating a 5-year survival rate of 60%.12,17–20
Conclusion
Syphilis is a public health problem that has resurfaced, and its early diagnosis and appropriate treatment can prevent serious complications such as syphilitic aortitis, a rare but dangerous condition that can endanger the patient's life. It is important to consider syphilis as a possible cause of aneurysms and endocarditis in high-risk populations and take preventive measures for timely detection and treatment.
Supplemental Material
sj-docx-1-sci-10.1177_00368504241308956 - Supplemental material for Endocarditis and ascending aortic aneurysm with aortic valve insufficiency secondary to late syphilis: Case report
Supplemental material, sj-docx-1-sci-10.1177_00368504241308956 for Endocarditis and ascending aortic aneurysm with aortic valve insufficiency secondary to late syphilis: Case report by Henry Robayo-Amortegui, Juan Rojas-Perdomo, Eduardo Tuta-Quintero, Natalia Valenzuela-Faccini, Carlos Fuentes-Pérez, Alexander Cely-Cely and Efraín Gómez-López in Science Progress
Footnotes
Acknowledgments
The authors are most thankful for the support of the Fundación Clínica Shaio.
Authors’ contributions
J.R.P., E.G.L., E.T.Q. and H.R.A. drafted the manuscript; N.V.F., C.F.P., A.C.C. and H.R.A. diagnosed and treated the patients; J.R.P. and E.G.L. analyzed the cases; H.R.A. provided the radiology images; M N.V.F., C.F.P., A.C.C. and H.R.A. analyzed the cases and provided critical revision of the manuscript; A.C.C. and H.R.A. collected the data; All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethics approval for reporting individual cases or case series.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fundación Clínica Shaio, DIB code 22-25.
Informed consent
The authors obtained written informed consent from the patient for the publication of the case information and any images.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.