
Abstract
Objectives
This study compared the clinicopathological, immunohistochemical characteristics and Epstein-Barr virus (EBV) detection of Burkitt's lymphoma (BL) in the abdomen and jaw of Iraqi patients.
Methods
A cohort/retrospective study was carried out between August and September 2024 using 25 tissue blocks (14 gnathic and 11 abdominal BL) from the Oral and Maxillofacial Laboratory, University of Baghdad, College of Dentistry, and the National Centre for Educational Laboratories. The sections were stained with haematoxylin and eosin (H&E), while CD10, CD20, Bcl-2, BCl-6, C-Myc and Ki-67 markers were used for diagnosis. The DNA detection of the EBV was performed by polymerase chain reaction (PCR).
Results
The tumours showed 22 classical and 3 atypical histological patterns. The mean age of the patients was 6.3 years, and the male-to-female ratio was 3.1:1. The younger patients were affected by the gnathic BL (P = 0.01), and the EBV was detected with a positive correlation (P = 0.005) in 14% of the gnathic and 72% of the abdominal tumours. There was no significant correlation between the Ki-67 expression and the clinicopathological features.
Conclusions
A critical finding of this study was that gnathic BL tends to affect people of a younger age. In addition, the abdominal presentation of EBV suggests a regional pattern of viral exposure, while there was no correlation between the aggressiveness of BL and viral exposure or the tumour site.
Keywords
Introduction
Non-Hodgkin lymphoma (NHL) is comprised of a heterogeneous group of lymphoid neoplasms. According to the classification of the World Health Organisation (WHO), the distribution of subtypes is significantly different in childhood and adulthood. In 1958, Dennis Burkitt initially identified Burkitt's lymphoma (BL) as a sarcoma in the jaws of African children. 1
Malignant head and neck lymphomas can involve the lymph nodes, soft tissues and bones in the maxillofacial region in 5% of all malignancies while representing 2% to 8% of thyroid malignancies. Three subtypes of BL have historically been recognised: endemic, non-endemic or sporadic and immunodeficiency associated. However, recent data suggest that the Epstein-Barr virus (EBV-positive and EBV-negative BLs), forms distinct biological groups, based on their molecular features, regardless of the epidemiological context and geographical location.2,3
According to the EBV status, there may be two different mechanisms involved in the pathogenesis of BL: virus-driven and mutational coding. In recognition of these discoveries in the biology of BL, the WHO-HAEM5 recommended separating BL into two subtypes: EBV-positive and EBV-negative BLs. 4
BL affects 2 to 3 cases per million people annually in the United States.5,6 In the African equatorial region, on the other hand, children account for up to 74% of childhood malignancies and the incidence of endemic BL is 5 to 10/100000.7,8
Several studies have examined the prevalence and incidence of BL among patients with NHL in various regions of Iraq. These studies also revealed unique characteristics that set this cancer type apart from Western and Mediterranean lymphomas. Research on the role of EBV in the pathogenesis of NHL in Iraq is ongoing in several different fields. The virus can be detected using a variety of techniques, including polymerase chain reaction (PCR), in situ hybridisation (ISH) and serological testing for immunoglobulin G (IgG) and immunoglobulin M (IgM). The percentage of BL positivity for EBV varied greatly among these studies.
This study analysed 25 case series of Iraqi patients with BL of the abdomen and jaw and compared their clinicopathological features and their relation to EBV infection.
Materials and methods
Nature of the study
The purpose of this cohort/retrospective study was to investigate the clinicopathological, molecular and immunohistochemical features of jaw and abdominal BL in a series of Iraqi patients to constitute an important addition to previous research and contribute to the advancement of diagnostic methods for these tumours in Iraq and the whole world. The reporting of this study conforms to STROBE guidelines. 9
Sample size calculation
Using G power 3.0.10 (Program written by Franz-Faul, Universitatit Kiel, Germany). With the power of study = 85%, alpha error of probability = 0.05 two-sided, and Correlation phi = 0.6 (moderate), with all these conditions the sample size is about 25 subjects. 10
Sample
Twenty-five tissue blocks of BL, in which 14 gnathic BL had been diagnosed between 1980 and 2023, were obtained from the Oral and Maxillofacial Laboratory, Department of Oral Diagnostic Sciences, University of Baghdad, College of Dentistry, and 11 abdominal BL diagnosed over the past 3 years only were retrieved from the National Centre for Educational Laboratories, Baghdad Medical City. The study was performed between August and September 2024. The patients selected consecutively which mean that all the cases, which were suggestive of BL, were examined first under the microscope by two experienced pathologists and then, immunoassayed for CD10 and CD20, Bcl-2, c-Myc, Bcl-6 B and Ki-67. The positive cases were included, while the negative cases were excluded, PCR detection of EBV was carried out at biotechnology research centre/Alnahrain University.
Ethical approval statement
The Ethics Committee of the University of Baghdad, College of Dentistry, Iraq gave its approval for the study, which was carried out in compliance with the Declaration of Helsinki in 1975 which revised in 2013 (Ref. number: 935. Date: 11/8/2024). The consent of the patients was obtained through a written consent form, as required by the Ethics Committee, names, phone numbers, addresses and any other data that may identify the patients were removed from our study to protect the patient's privacy.
Histology and immunohistochemistry
Tissue blocks fixed in paraffin were regularly sectioned and stained by haematoxylin and eosin (H&E). BL was ultimately diagnosed by comparing the morphological features with the immunohistochemistry findings for an antibody panel, including CD20 (Dako: IR604), CD10 (Dako: IR648), Bcl-2 (Dako: M0887), Bcl-6 (Dako: M7211), c-Myc (PathnSitu: PR034) and Ki-67 (Dako: IR626). The immunohistochemical analysis was meticulously carried out by two experienced pathologists. The Ki-67 expression was used to assess the proliferation index for all the cases. All the stained nuclei were counted as positive regardless of the staining intensity. The Ki-67 labelling index (LI) was determined by multiplying the number of positive Ki-67 cells by 100 and dividing the result by the total number of identified neoplastic cells.
Polymerase chain reaction
By the instructions of the Geneaid® kit manufacturer, DNA was extracted from the paraffin-embedded samples. All the DNA samples were measured and stored at −20°C in a freezer. The DNA qualification was made by measuring the absorbance of the samples at 260 (A260) and 280 nm (A280). A Nanodrop® spectrophotometer was used to assess the content and purity of the DNA. The purity of the DNA was (108-2). The extracted DNA and PCR products in agarose gel were electrophoresed. A PCR was performed using primers specific to the EBV sequencing gene. The primer sequence is shown in Table 1. The PCR protocol included a 5-minute initial denaturation stage at 94°C, 30 cycles at 94°C for 30 seconds, annealing at 55°C for 30 seconds, extension at 72°C for 30 seconds, and a final extension stage at 72°C for 5 minutes.
The primer sequence of DNA.
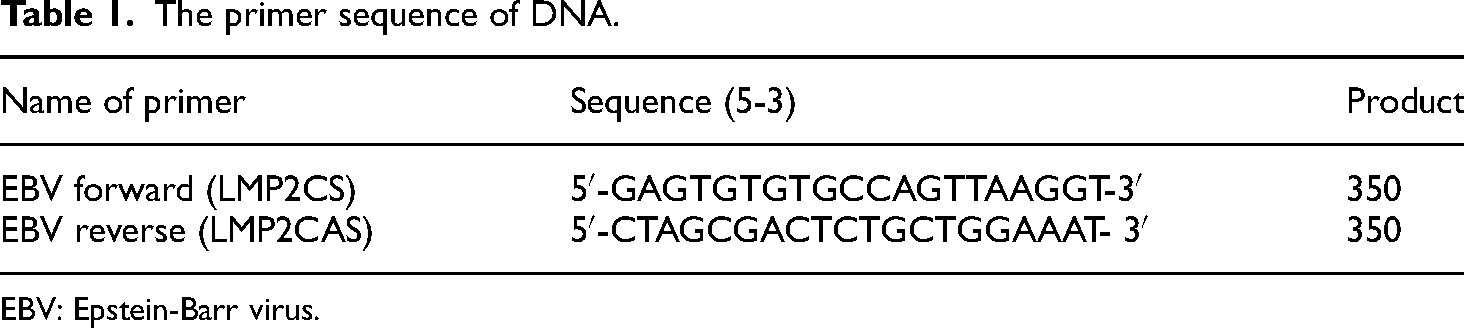
EBV: Epstein-Barr virus.
EBV NA2 gene (product size 339) was used as a control for PCR with a primer sequence as follows:
F- GCTGCTACGCATTAGAGACC R- TCCTGGTAGGGATTCGAGGG
Statistical analysis
The chi-square test was used for the nominal data. The independent sample t-test was used for the normally distributed numerical data, while the Mann-Whitney U test was used for the non-normally distributed data. The Spearman's test was used to correlate the age and the Ki-67 expression. P < 0.05 was considered as statistically significant. All the statistical analyses were performed using the IBM® Statistical Package for Social Sciences (SPSS®) 26.
Results
Histopathological features
All the cases of BL of the jaw presented with a classical histological morphology. At low power, a characteristic starry-sky pattern was obtained. This was caused by the many benign macrophages consuming the apoptotic tumour cells dispersed throughout the basophilic tumour cells. The tumour mass infiltrated the alveolar bone surrounding the roots of teeth. At high power, classically monomorphic, medium-sized cells with round nuclei, multiple dark nucleoli, and basophilic cytoplasm were seen. These tumour cells had infiltrated the periodontium and cementum of the roots of teeth (Figure 1(a) and (d)).

Haematoxylin and eosin tissue sections of Burkitt's lymphoma (BL). (a) Jaw BL at low power section (100×) showed tumour mass infiltrate the alveolar bone, high power sections (400×) showed tumour cells infiltrate the periodontium and cementum of teeth roots. (b) Abdominal BL showed a classical histological pattern with a starry sky appearance (400×). (c) Atypical histological pattern of BL. (D) Jaw BL showing classical stray sky appearance (scale bar:100 µm for all images).
The abdominal BL cases presented with classical (Figure 1(b)) and atypical forms (three cases out of 11 were atypical BL), whereas the lesional cells were medium to large, with relatively uniform nuclei, small nucleoli, thin rims of cytoplasm, nuclear pleomorphism, frequent mitoses and apoptotic bodies, with focally interspersed macrophages and sparse small T cells (Figure 1(c)).
All the tumour cells were positive for the CD20 and CD10 which showing membranous and cytoplasmic reactivity (Figure 2(d) and (e)) with nuclear expression for C-Myc and Bcl_6 (Figure 2(a) and (b)), Bcl-2 antibody showing negative reactivity in all cases (Figure 2(c)) while the Ki-67 LI was higher than 90% (Figure 2(f)).

Immunohistochemical staining of Burkitt's lymphoma showing: (a) Bcl-6 positive nuclear staining, (b) c-Myc nuclear and cytoplasmic positive staining, (c) Bcl-2 negative staining, (d) CD20 with cytoplasmic and membranous reactivity, (e) CD10 with membranous reactivity and (f) Ki-67 with nuclear reactivity (magnification = 400× and scale bar = 100 µm for all images).
Demographical and anatomical characteristics
As seen in Table 2, the male-to-female ratio was 3.1:1, with the median age being 6.3 years. Of the 25 cases, 14 (56%) had a gnathic presentation (maxilla and mandible) that appeared as a large infiltrative mass which appear radiographically as a heterogenous lesion infiltrating the surrounding cavities such as maxillary sinus and orbital cavity as seen in Figure 3(a) and (b), while 11 (44%) had abdominal involvement (ileocecal, retroperitoneal and abdominal lymph nodes).

Clinical and radiographical images of Burkitt's lymphoma (BL) of jaw. (a) Large palatal mass in 9-year female patient involving the whole maxillary alveolar bone. (b) Coronal section computed tomography image of the face showing heterogenous lesion of BL infiltration to orbital cavity (scale bar :1000 µm for all images).
Clinicopathological features of BL cases.

** Small bowel (2), ileocecal (3), lymph nodes (4), and retroperitoneal (2).
Statistically, there was no significant correlation between gender and the presentation site (P = 0.6), but there was a significant correlation between age and the presentation site (P = 0.01), suggesting that gnathic BL affected the younger patients in this sample.
Polymerase chain reaction
EBV DNA was found in 10 out of the 25 cases, 14% of them being gnathic cases (2 cases), and 72% (8 cases) abdominal cases. As a result, there was a statistically significant correlation between EBV detection and the presentation site, with abdominal BL showing a higher positive correlation (P = 0.005). No statistically significant correlation was found between EBV detection and the patient's age (P = 0.007). However, the median age of positive cases (8.4) was higher than that of negative cases (5.01).
Proliferation index
Overall, the Ki-67 expression was high (mean = 90.4%). However, there was no statistically significant relationship between the Ki-67 expression and age, gender, location or EBV detection, where the P values were 0.4, 0.5, 0.7 and 0.9, respectively.
Discussion
BL is a highly aggressive B-cell neoplasm, often presented in extranodal sites, and typically associated with MYC gene translocation, EBV, HIV and malaria infections. Although its aetiology has been extensively assessed, information regarding its prognostic factors, especially when it involves the oral and maxillofacial region, remains limited to case reports, case series and small cohort studies. 11 BL must be distinguished from diffuse large B-cell lymphoma and other high-grade B-cell lymphomas that may have an MYC translocation. Other entities in the differential diagnosis of BL include lymphoblastic lymphoma/leukaemia and blastoid mantle cell lymphoma. 12 As far as is known, this study represents the second-largest sample of gnathic BL in Iraq after Uccini et al.. 13 The prevalence of BL among lesions submitted for biopsy at the Oral and Maxillofacial Laboratory, University of Baghdad, College of Dentistry was 0.2%. Most studies focused on the prevalence of BL among patients with NHL, with results varying widely among different Iraqi regions. In northern Iraq, two studies have reported that BL accounts for nearly 7% of NHL cases, with the abdomen being the most common site of occurrence.14,15
However, research conducted at child teaching hospitals in Baghdad Medical City has shown that BL accounts for 40% and 58.33% of NHL cases.6,13,16,17 Nonetheless, a study conducted at the al-Hussein Cancer Hospital in Karbala revealed that the frequency of BL in the middle Euphrates region was 14.2% of 92.47% B-cell lymphoma, with gnathic BL accounting for only 4% to 6% of all instances. 18
The patient demographics in this study were in line with those of most other research investigations conducted in Iraq.13–24
Morphologically, as mentioned above, the majority of the cases revealed histological features of classical BL, except for three abdominal cases that showed atypical BL. So, the findings of this study were like those reported in the literature, with most tumours of head and neck BL showing the classical morphological characteristics of BL.13,25
The prevalence of EBV-positive cases of BL in this study (40%) was in agreement with two previous studies. One of them determined the frequency of EBV lmp-1 in Iraqi patients with NHL, while the other study was conducted by ISH,21,22 but disagreed with four previous Iraqi studies,13,15,19,23 which detected EBV in 80%, 73%, 84% and 78% of Iraqi patients, respectively. These discrepancies in the results on the role of EBV among cases of Iraqi patients with BL may be related to the multiple laboratory methods used by these studies for virus detection such as PCR, ISH, fluorescent in situ hybridisation (FISH), serological detection of virus IgG and IgM, as well as to tumour site, sample size, and regional distribution of cases.
The relation between EBV infection and the age of the patient had no statistically significant correlation in this sample, which might have been due to the small sample size. However, the median age of patients with positive EBV infection was higher than that of the negative cases. This result was in agreement with a study conducted in Sulaimani by Muhaldeen et al., which found that 90% seropositivity was reached at age 15. Seropositivity is often delayed until adolescence or early adulthood in Europe and North America, with adult BL predominating over childhood BL. On the other hand, early childhood exposure to EBV is predominant in Africa and much of Asia, with virtually all children being infected by the time they are 5 years old. Childhood BL is somewhat common and adult BL is uncommon in the Middle East. It is proposed that the high childhood and low adult BL rates may be a regional effect of a pattern of EBV exposure intermediate between early childhood and adolescent and young adult infections. 19
The greater incidence of abdominal rather than gnathic presentations and the propensity for these cases to be EBV-positive were further characteristics that set the Iraqi BL apart. Yet the results of this study were consistent with those that had been previously documented for BL in Turkey, Brazil, Argentina and India. All of them point to the existence of at least two distinct types of sporadic BL. One is more prevalent in Japan and the West and is distinguished by a low incidence of EBV-positive cases (20–30%), while the other is more prevalent in poorer nations and is distinguished by a large percentage (40–80%) of cases with EBV infection. The disparity between the two types is most likely brought about by the poorer socioeconomic standing of emerging nations, which may also be the cause of early-life EBV infection.
Ki-67 has been employed as a tumour cell proliferation marker for a long time because it is involved in both interface and mitotic cells. In this work, the proliferation index was measured using the proportion of Ki-67 expression, which does not show any statistically significant link between demographical and pathological characteristics.
The current investigation found no variations in antibody expression compared to prior studies analysed by immunohistochemistry. As reported by others, our immunohistochemical data revealed that the key antibodies utilised in the diagnosis of BL include B-cell markers, mainly CD20, and markers of germinal center B-cell origin such as CD10 or Bcl-6. 26 All these markers show strong positivity in BL cases of this study with membranous and cytoplasmic expression of CD10 and CD20 and nuclear and cytoplasmic expression of c-Myc with nuclear expression of Bcl-6 while Bcl-2 showing negative reactivity in all cases including jaw and abdominal cases
Acknowledging the retrospective nature of this study, the focus was narrowed to biopsy-proven BL cases. The relative rarity of this tumour inherently limited the scope for broader statistical analyses. It is posited that future studies, benefiting from multicentre data pooling, could offer a more precise delineation for the demographical and clinicopathological features of BL, thus enriching the existing body of knowledge on this peculiar type of lymphoma.
Conclusion
In conclusion, this Iraqi sample of BL has unique characteristics, such as the younger age at which jaw tumours present and the tendency of abdominal tumours to be infected by the EBV in later childhood. It is proposed that the aggressiveness of abdominal and gnathic BL may be independent of the presence of the EBV and vice versa.
Footnotes
Acknowledgements
We would like to acknowledge and give our special thanks to assistant professor Dr Ameer Thahir for his guidance and assistance in sample collection and diagnosis of Burkitt's lymphoma submitted for our oral and maxillofacial laboratory, also special thanks to our colleague assistant lecturer Noor Allawi for his assistance in statistical analysis of this study.
Authors’ contribution
AWI was involved in conception, data curation and preparation of the manuscript; BA-D in analysis of data and supervision; FI in conception, data curation and preparation of the manuscript; and BA in conception, supervision and revision for important intellectual content.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.