
Abstract
Malignant transformation arising in the background of jaw cysts is a rare and often misdiagnosed condition, particularly when developing from residual root-derived cysts. We present a case of epithelial malignancy originating from a residual root-derived cyst in the mandible of a man around 50 years old. Histological evaluation of the sections revealed that the epithelial lining of the cystic lesion contained well-differentiated squamous cell carcinoma components. Finally, a segmental mandibulectomy was performed, and the defect was reconstructed with free iliac bone grafting. This case underscores the critical role of chronic inflammation in the malignant transformation of mandibular cysts and enriches the current database on odontogenic cyst malignancy.
Introduction
The development of epithelial malignancies from odontogenic cysts is rare. This uncommon neoplasm is a subtype of primary intraosseous squamous cell carcinoma (PIOSCC). 1 According to the latest World Health Organization classification of tumors, PIOSCC is defined as squamous cell carcinoma that develops within the jaw and is derived from the residual odontogenic epithelium or tumor. The clinical presentation of PIOSCC is often atypical and may be accompanied with or without local pain and numbness, complicating diagnosis and potentially delaying treatment, which can lead to a poor prognosis.2–5 We present an asymptomatic case of epithelial malignancy caused by the residual root-derived cyst of the mandible in a man around 50 years old. The reporting of this study conforms to CARE guidelines. 6
Case report
A male patient, approximately 50 years old, was referred to the Department of Oral and Maxillofacial Surgery at Qingdao University Affiliated Hospital in April 2022, after cone-beam computed tomography (CBCT) detected low-density anomalies in the right mandibular region. His medical history indicated the loss of the crown of the right mandibular second premolar due to caries 8 years earlier, followed by fixed porcelain bridge restoration. Remarkably, throughout this period, the residual roots remained free of inflammation and were not extracted. CBCT revealed a localized radiolucent area at the site of the residual root in the right mandible, with well-defined, sharp margins and no sclerotic border (Figure 1(A)), and cystic bone destruction in the right mandibular region, with clear lesion boundaries and homogeneous density. The tooth root extended into the cyst cavity, with no periosteal reaction or soft tissue mass surrounding the lesion (Figure 1(B) to (D)). Additionally, the chest computed tomography revealed no abnormalities. The patient did not complain of discomfort or lower lip numbness. No mucosal abnormalities or jaw swelling were observed during the intraoral examination. The patient and his family agreed with surgical interventions after thorough communication, and written informed consent was obtained. Under general anesthesia, the cyst and granulation tissue were completely removed according to the treatment plan for odontogenic cysts. During the operation, it was observed that the cyst was not connected to the oral mucosa. Unexpectedly, the histopathological findings revealed a well-differentiated squamous cell carcinoma (Figure 2). Finally, a segmental mandibulectomy was performed, and the defect was reconstructed with free iliac bone grafting. No postoperative adjuvant radiotherapy was recommended in our case by the multidisciplinary team, and after nearly two years of follow-up, there was no evidence of recurrence or locoregional metastasis.
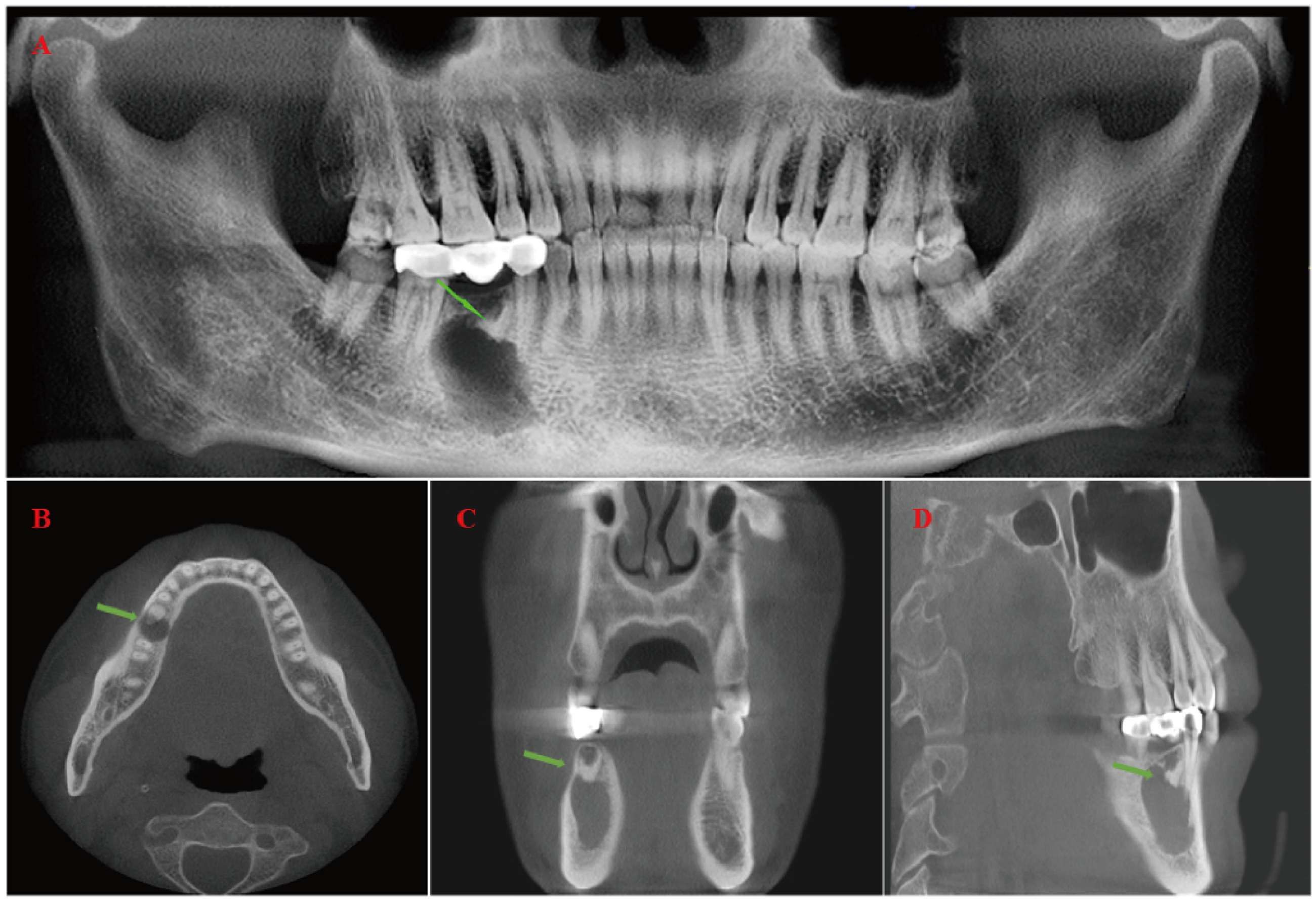
Cone-beam computed tomography (CBCT) revealed a relatively well-defined unilocular radiolucency with the residual root in the right mandible. (A) Panoramic (dental) radiograph. (B) Axial plane. (C) Coronal plane. (D) Sagittal plane. (The residual root is shown by the green arrow.)
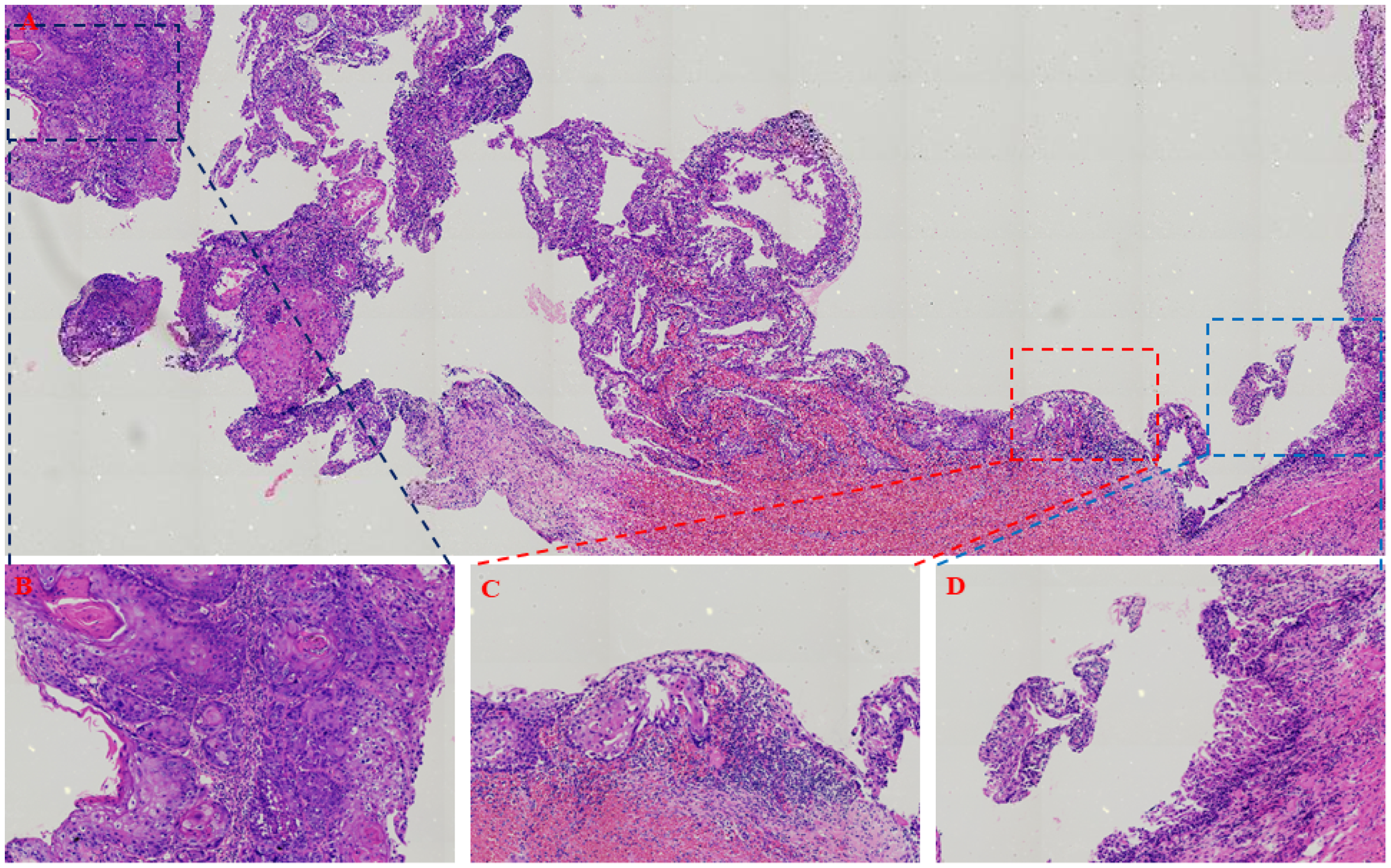
The histopathological examination revealed the transformation of the residual cyst into squamous cell carcinoma. (A) The cystic lining is composed of stratified squamous epithelium, with areas exhibiting mild to moderate atypical hyperplasia or cellular atypia, accompanied by the formation of keratin pearls (×200). (B) Squamous cell carcinoma (×400). (C) Atypical epithelial hyperplasia (×400). (D) The epithelium of the normal cyst wall (×400).
Discussion
PIOSCC is characterized as a rare malignant tumor originating from residual odontogenic epithelium or developing from odontogenic cysts. 7 This tumor presents a challenge in diagnosis due to the absence of clear clinical and radiographic features. 8 PIOSCC is a subtype of squamous cell carcinoma. Microscopically, cellular atypia of the squamous epithelium is observed, characterized by hyperkeratosis, incomplete keratinization, and the formation of keratin pearls, with no mucinous cell components present, distinguishing it from mucoepidermoid carcinoma. 9 Furthermore, PIOSCC lacks palisaded columnar cells and stellate reticulum-like cells, further differentiating it from ameloblastic carcinoma. 10
Furthermore, current reports on this type of disease often lack descriptions of the transitional areas between cystic epithelium and squamous cell carcinoma, hindering a deeper understanding of PIOSCC. Here, we report a case of a cystic lesion associated with a residual root presenting epithelial malignancy in a man around 50 years old. Pathological examination revealed the transition from normal cystic epithelium to atypical proliferation culminating in squamous carcinoma.
The mechanisms underlying the malignant transformation of jaw cysts remain unclear. This is probably associated with inflammation-induced epithelial damage and the special anatomical and histological structure of the jaw. In addition, recurrence and multiple surgical stimuli may be related to the malignant transformation of odontogenic cysts. 11 Patients with an initial malignant transformation of an odontogenic cyst often have no specific symptoms. According to the imaging data, it is often difficult to diagnose malignant lesions, which may lead to treatment delays. By sharing this case, clinicians may be aware that a residual root-associated cystic lesion with epithelial malignancy may initially present as a relatively well-defined unilocular radiolucent lesion. Additionally, for the pathological examination of all surgically excised cysts to make a diagnosis, it is necessary to avoid relying solely on the clinical experience of doctors. A careful pathological examination is vital to identify the potential malignant features of this rare entity. According to the histological examination, various treatments, such as conservative treatment, bone resection, and mandibulectomy with or without adjuvant treatments, have been reported in the literature. 12 In addition, Hegde et al. 13 suggested that segmental mandibulectomy with neck dissection should be performed in patients diagnosed with epithelial malignancy during the second histological examination. To date, the literature lacks sufficient detailed data to evaluate the recurrence and survival rates of epithelial malignancies from odontogenic cysts due to the limited number of cases. In our case, there was no evidence of recurrence or locoregional metastasis after nearly two years of follow-up. Theoretically, early diagnosis and surgical intervention have a potential role in improving patient outcomes.
Conclusion
Malignant transformation of jawbone cysts is exceedingly rare. This report presents a case of PIOSCC arising from a residual tooth root. It serves as a reminder that PIOSCC may not present with typical symptoms or imaging abnormalities in its early stages, even though malignant transformation may already be underway.
Footnotes
Author contributions
Zongxuan He: conceptualization, methodology, and software. Yueqin Tao: data curation and writing—original draft preparation. Jieying Li: visualization and investigation. Wei Shang: supervision, software, and validation. Kai Song: writing—reviewing and editing.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 81502340).
Ethical approval
Ethical approval for this case report was not required according to the guidelines stated by the Research Ethics Board of Qingdao University. The board has approved the publication of the case report.
Informed consent
We have obtained the written informed consent form signed by the patient for publication.