
Abstract
This study aims to explore: (1) the validity of post-exercise ultra-short-term heart rate variability (HRVust) after two different bouts of repeated sprint ability test (RSA), and (2) the relationship between HRVust measure and RSA performance. Twenty adolescent male futsal players voluntarily participated in this study (age: 17.65 ± 1.81 years, body height: 170.88 ± 4.98 cm, body weight: 61.78 ± 4.67 kg). The participants performed a standard RSA test (RSAstandard) and an RSA test with a 10% decrement of the best sprint time test (RSA10%decrement) on two separate occasions within a week. On both occasions, a 5-min resting electrocardiography was administered pre- and post-RSA exercise protocols. The first 30-s (HRVust30s), 60-s (HRVust60s), and 60–120-s (HRVust1−2min) were extracted and used to compare with the standard of 5-min HRV recording (HRVcriterion). The natural logarithm (ln) of the standard deviation of normal-to-normal intervals (SDNN) and root mean square of successive normal-to-normal interval differences (RMSSD) HRV indices were utilised to establish intraclass correlation coefficient (ICC2,1), coefficient of variation (%CV), and Pearson product-moment correlation (r). Results revealed the ICC values of HRVust lnSDNN (RSAstandard = 0.77–0.88; RSA10%decrement = 0.41–0.71) and lnRMSSD (RSAstandard = 0.81–0.86; RSA10%decrement = 0.57–0.82). Furthermore, significantly positive correlations between best sprint time and post-exercise HRVust indices were found in lnSDNN (r = 0.47–0.62; p < 0.05) and lnRMSSD (r = 0.45; p < 0.05). Additionally, a large CV of lnSDNN (RSAstandard = 32%–45%; RSA10%decrement = 29%–39%), lnRMSSD (RSAstandard = 50%–66%; RSA10%decrement = 48%–52%), and ratio (RSAstandard = 45%–126%; RSA10%decrement = 27%–45%) was found after the RSA protocols. In conclusion, the number of bouts of RSA exercise potentially influences the agreement of post-exercise time-domain HRVust indices to standard HRV measure.
Keywords
Introduction
In the recent decade, short-term heart rate variability (HRV) measures have been widely used in athletic settings to assess sympathovagal balance. 1 A typical measurement for a short-term record of HRV involves a 5-min stabilisation phase followed by a 5-min measure.2,3 However, implementing such a technique during sports training could be challenging due to time limitations and the availability of portable equipment. Thus, exploring alternatives for short-term HRV may provide more support among sports science practitioners in athletic settings.3–5 Based on this demand, the ultra-short-term HRV (HRVust) has been suggested, requiring only a 10–60 s record and a 60-s stabilisation period. 6 Studies demonstrated that HRVust is valid and reliable for assessing the autonomic nervous system (ANS) in sporting contexts.4–9
Among the HRV indices, the standard deviation of normal-to-normal intervals (SDNN) and root-mean squared of successive differences (RMSSD) are strongly supported markers for parasympathetic nervous system (PNS) function.10,11 In a practical setting, the natural logarithm of RMSSD (lnRMSSD) determined in the first minute, following 1-minute of stabilisation, is sensitive to training-induced change and can be used to track cardiac autonomic adaptations. 7 Assessment of time-domain HRVust by using lnSDNN and lnRMSSD is valid and more convenient than frequency-domain HRVust due to the agreement of conventional record and time-saving. 12 Alternatively, Esco and colleagues 4 proposed the HRVust of the lnSDNN:lnRMSSD ratio as a marker for sympathovagal balance. Therefore, the HRVust is a promising method for strength and conditioning practitioners and sports scientists, requiring minimal time to identify autonomic activity.
The exercise intensity mainly influences the function of ANS recovery due to the effects of exercise-induced vagal withdrawal. 13 During post-exercise recovery, parasympathetic activation and sympathetic withdrawal are crucial in dominating post-exercise autonomic control. 14 For example, prepubertal boys and endurance athletes showed faster HR recovery and higher lnRMSSD values after an incremental run field test than untrained adults, indicating a strong function of parasympathetic reactivation in these populations. 15 However, current knowledge regarding the application of HRVust in post-exercise conditions has yet to be fully understood.16–19 Previously, our laboratory reported that post-exercise time-domain HRVust measure requires one-minute stabilisation for acceptable agreement to a 5-min HRV record but not frequency-domain HRVust measure. 17 However, the contribution of exercise load to limit agreement of HRVust measures needs to be clarified in this previous report. Thus, more information should be given regarding the influence of exercise intensity on post-exercise HRV measures.
In light of the abovementioned, the primary aim of this study was to investigate the reliability of HRVust from standard repeated sprint ability protocol (RSAstandard) and RSA test with a 10% decrement of best sprint time test (RSA10%decrement). The secondary aim of this study was to examine the relationship between HRVust and RSA performance.
Materials and methods
Study design
A crossover research protocol was employed in this study, wherein the experimentation sessions for the RSAstandard and RSA10%decrement protocols were separated by 7 days. A 5-min HRV measurement was conducted before the exercise protocols. We extracted three time segments of HRVust from the standard 5-min HRV recording (HRVcriterion), which were: (1) 0–30 s (HRVust30s); (2) 0–60 s (HRVust60s); and (3) 1–2 min (HRVust1–2min). The lnSDNN and lnRMSSD were analysed due to the minimal interference of respiratory patterns during strenuous exercise.20,21
Participants
Twenty adolescent futsal players participated in this study (see Table 1). The inclusion criteria for participation included: (1) undergoing weekly futsal training of at least three sessions (more than 6 h) per week; (2) experience in futsal training of ≥5 years; and (3) competition level of division of a national senior high school/university championship. Exclusion criteria for participation included: (1) severe neuromuscular injury history; (2) lower extremity injury of ≤6 months; and (3) neurological or cardiovascular diseases. Participants submitted written informed consent before further participation. The participants were instructed to avoid vigorous exercise 24-h before the experimental visit. They were requested to skip caffeine-containing substances 2-h prior to the tests. Ethical approval by the institutional board of human ethics committee at the University of Taipei was obtained prior to the experiment (code number: UT-IRB-2019-081). This study was conducted in compliance with the Declaration of Helsinki.
Physical characteristics and performance of repeated sprint ability tests of the participants.
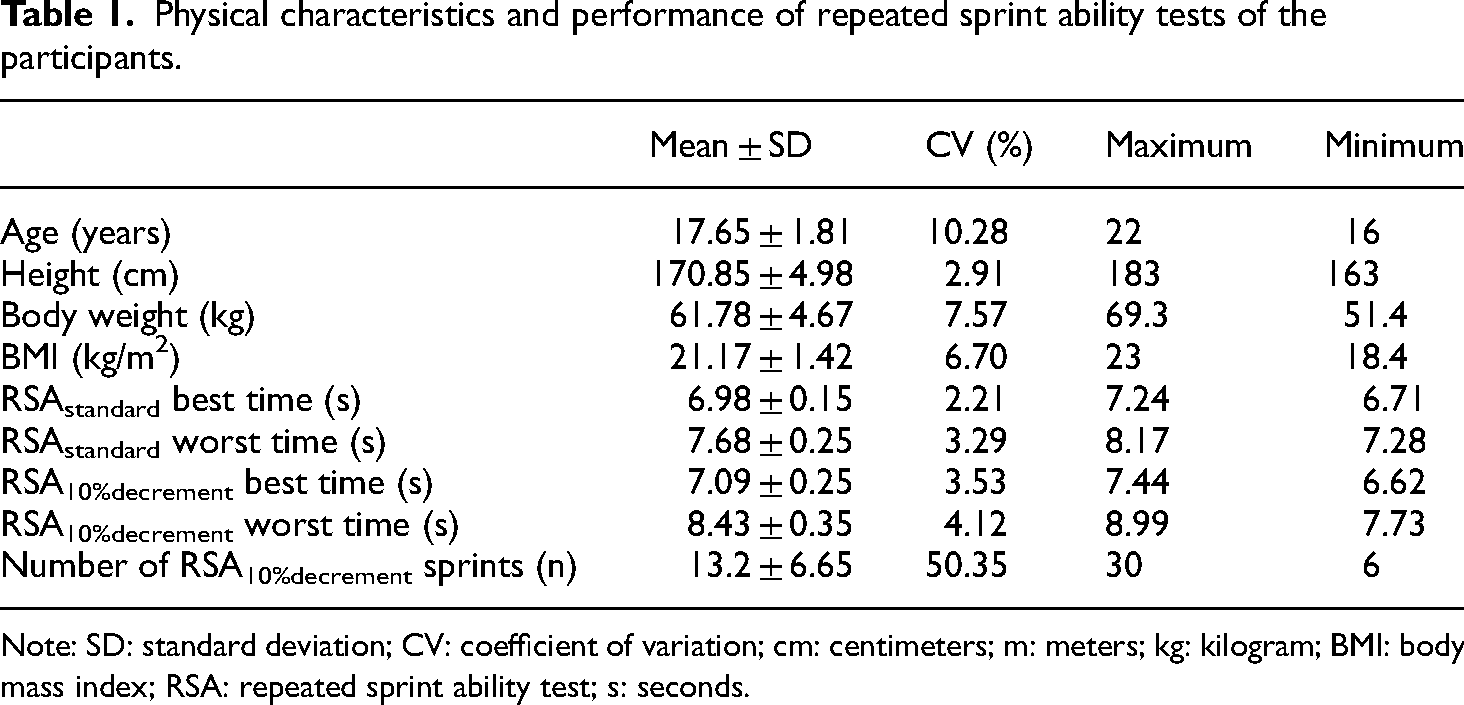
Note: SD: standard deviation; CV: coefficient of variation; cm: centimeters; m: meters; kg: kilogram; BMI: body mass index; RSA: repeated sprint ability test; s: seconds.
Experimental procedures
Participants visited the exercise science laboratory on three occasions at similar times. In the first visit, measurement of physical characteristics and habituation with exercise protocols were conducted. The second and third visits included the RSAstandard and RSA10%decrement measurements in a randomised order. Randomisation was achieved using an online randomiser tool (https://www.randomizer.org). Both sessions preceded a 5-min HRV recording and 10-min warm-up exercises, respectively. The warm-up included dynamic stretching exercises (lunge and reach, reverse lunge and twist, leg swing to toe touch, and knee hug to quadstretch) performed for 2 sets of 5 repetitions and 2 repetitions of 20-m sprint at 80% subjective maximal effort. The rest interval in between sprints is 2 min. Afterwards, they performed the RSAstandard or RSA10%decrement on an indoor artificial track. This was succeeded by a 5-min HRV recording. All experimental sessions were conducted between 8 am and 12 pm in the exercise performance laboratory of the University of Taipei Tianmu campus.
Heart rate variability measures
A lead II electrocardiogram (ECG) configuration (SS2LB, Biopac Inc., Goleta, CA, USA) was employed to acquire pre- and post-exercise HRV. Disposable ECG electrodes were used for data collection (Kendall™ 200 Series Foam Electrodes; Covidien, Mansfield, MA, USA). Measurement of 5-min seated HRV was administered in a dimly lit room. The ECG signals were processed through a commercial data acquisition unit (MP35, Biopac Inc., Goleta, CA, USA) with a sampling rate set at 1000 Hz. After recording, the ECG data were extracted to Kubios HRV software (Premium version 3.3.1, Kuopio, Finland) for subsequent analysis. The ECG data was filtered at a medium-level threshold for artefact correction. Also, the window width acquisition was set at 300 s and a 50% window overlap. Further, a detrending method of 500 Lambda smoothing priors was utilised. 22 The SDNN and RMSSD were transformed into natural logarithms (lnSDNN and lnRMSSD) and used for analyses. Additionally, the ratio of lnSDNN : lnRMSSD was examined to interpret sympathovagal responses after the RSA exercises. 4
Repeated sprint ability test
The RSAstandard consists of 6-bouts of 20-m all-out shuttle running, with a 20-s recovery interval between the bouts. The RSA10%decrement involved repeated bouts of 20-m shuttle sprint performance until a 10% decrement of the best RSA sprint time in the first 6-bouts was achieved. This criterion was used due to the median value of sprint number for target fatigue index.23,24 During the 20-s recovery interval, the participants were encouraged to engage in passive or active recovery before the next bout. The sprint time for each bout was recorded via a photocell timing gate system (Fusion Sport, Brisbane, Queensland, Australia). The timing gate was placed 30-cm behind the starting line and the light beam was set 1.2-m. Two preliminary trials were given to participants before measuring RSA performance.17,25 The reliability of the RSA test at a level of interclass correlation coefficients (ICC) was 0.81. 26
Statistical procedures
A post-hoc power analysis from the correlation: the bivariate normal model was used to estimate the sample size in this study (G*Power 3.1.9.4, Düsseldorf, Germany). Post-hoc compute achieved power was used for a type of power analysis. The power was determined at the 2-tailed and α = 0.05 levels. Correlation ρ H1 was set for the optimal correlation value and correlation ρ H0 was set as “0.” The power (1-β err prob) was determined as 0.85.
Statistical analyses were performed via an SPSS software package (SPSS® 25.0, IBM, Armonk, NY, USA). The normality of data was assessed via Kolmogorov–Smirnov test. The intraclass correlation coefficient (a model of two-way random and a type of single measure, ICC2,1) was used to determine the reliability among variables. The level of ICC value is defined as poor (<0.40), fair (0.41–0.59), good (0.60–0.74), and excellent (0.75–1.00). 27 The coefficient of variation (CV) was also employed to identify the dispersion of data. Moreover, the bias of the measure was quantified to evaluate the mean difference between the HRV measures. Furthermore, Pearson's product-moment correlation (r) was used to examine the relationship between different time segments of HRV variables and RSA performance. The level of r value is defined as trivial (r < 0.1), small (0.1 < r < 0.3), moderate (0.3 < r < 0.5), high (0.5 < r < 0.7), very high (0.7 < r < 0.9), nearly perfect (r > 0.9), and perfect (r = 1). 28
Results
Anthropometric characteristics and performance variables
Descriptive statistics of anthropometric characteristics and RSA performance are presented in Table 1.
Validity of post-exercise heart rate variability measures
At the pre-exercise measure, the results of HRVust showed the ICC values of lnSDNN ranging from 0.80 to 0.95. Additionally, the ICC values of lnRMSSD HRVust were 0.91 to 0.98. The HRVust of lnSDNN : lnRMSSD ratios demonstrate ICC values from 0.49 to 0.86.
Regarding the post-exercise measure, the HRVust ICC values in the RSAstandard protocol range 00.77–0.88 for the lnSDNN, 0.81–0.86 for the lnRMSSD, and 0.33–0.66 for the lnSDNN:lnRMSSD ratio. However, in the RSA10%decrement protocol, the lnSDNN ICC values for the HRVust30s, HRVust60s, and HRVust1–2min were 0.41, 0.56, and 0.71, respectively. For the lnRMSS, the ICC values were identified at 0.57, 0.64, and 0.82 in HRVust30s, HRVust60s, and HRVust1–2min time segments. For the lnSDNN : lnRMSSD ratio, the ICC values were 0.70 in the HRVust30s, 0.87 in the HRVust60s, and 0.93 in the HRVust1–2min time segments. All parameters demonstrate the largest bias in the HRVust30s (see Table 2).
Agreements of the natural logarithm of standard deviation of normal-to-normal intervals (lnSDNN), the root mean square of successive normal-to-normal interval differences (lnRMSSD), and the ratio of lnSDNN : lnRMSSD during 0–30 s, 0–60 s, 1–2 min, and 0–5 min time segments of the baseline and post-exercise measures in the repeated sprint ability test protocols.
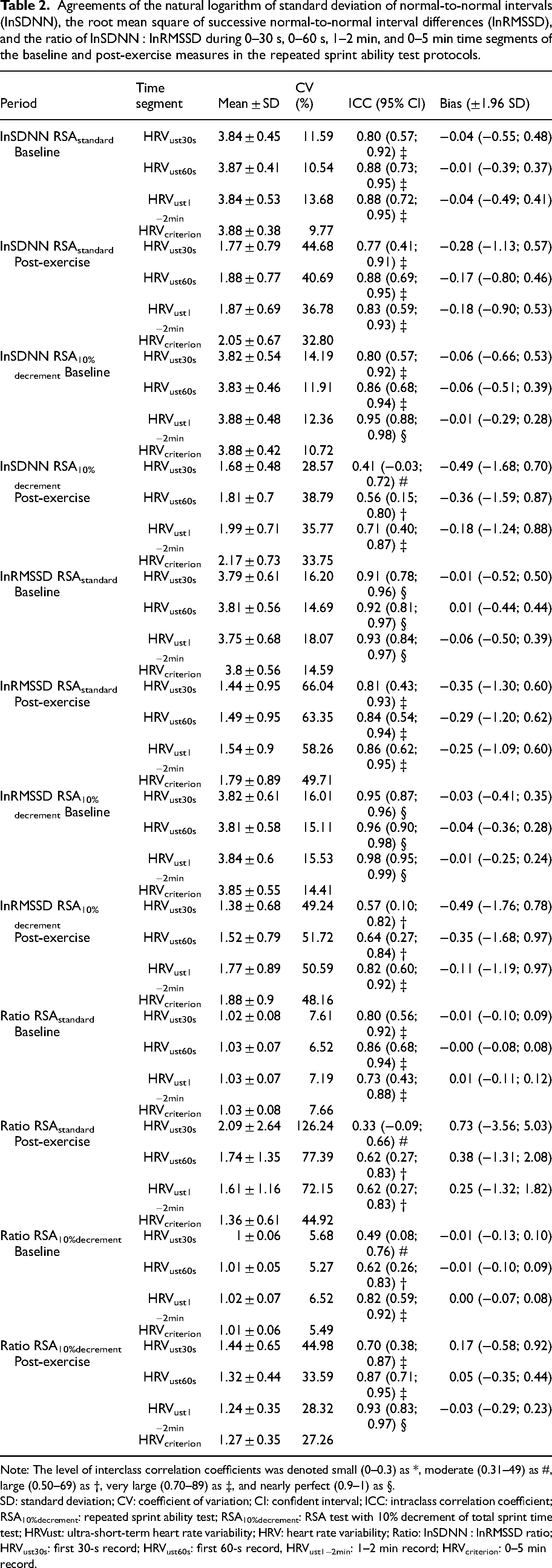
Note: The level of interclass correlation coefficients was denoted small (0–0.3) as *, moderate (0.31–49) as #, large (0.50–69) as †, very large (0.70–89) as ‡, and nearly perfect (0.9–1) as §.
SD: standard deviation; CV: coefficient of variation; CI: confident interval; ICC: intraclass correlation coefficient; RSA10%decrement: repeated sprint ability test; RSA10%decrement: RSA test with 10% decrement of total sprint time test; HRVust: ultra-short-term heart rate variability; HRV: heart rate variability; Ratio: lnSDNN : lnRMSSD ratio; HRVust30s: first 30-s record; HRVust60s: first 60-s record, HRVust1−2min: 1–2 min record; HRVcriterion: 0–5 min record.
Relationship between post-exercise heart rate variability and RSA performance
There was a significant relationship between post-exercise HRV and best time (r = 0.62) and worst time (r = 0.45) during the RSA10%decrement protocol (see Figure 1). Regarding the lnSDNN, positive correlations were between sprint time and HRVust time segments (r = 0.50–0.62, p < 0.05). Furthermore, the lnRMSSD showed a significantly positive correlation between the best time and the HRVust30s and HRVust60s time segments (r = 0.45, p < 0.05).

Pearson correlation between post-exercise heart rate variability indices and the best time and worse time during the repeated sprint ability test with 10% decrement of best repeated sprint protocol (RSA10%decrement). (A) Relationship between lnSDNN value and best RSA time; (B) relationship between lnSDNN value and worse RSA time; (C) relationship between lnRMSSD value and best RSA time; (D) relationship between lnRMSSD value and worse RSA time.
Discussion
This study aimed to examine the agreement of HRVust after repeated sprint performance. Compared to the standard 5-min HRV record, a large variation in HRVust measures was identified after the RSA exercise protocols (RSAstandard CV = 36.8%–66%; RSA10%decrement CV = 28.6%–51.7%). The post-exercise ICC values of HRVust measures were excellent during the RSAstandard protocol (0.77–0.88) but ranged from fair to excellent levels during the RSA10%decrement protocol (0.41–82). Moreover, 1-min stabilisation during the post-exercise period of the RSA10%decrement exercise protocol is recommended to provide acceptable levels of validity and tight limits of agreement of HRVust measures of time-domain variables (lnSDNN = 0.71; lnRMSSD = 0.82). The HRVust lnSDNN and lnRMSSD variables posted a positive relationship with the best sprint time during the RSA10%decrement protocol. The number of bouts of RSA exercise potentially influences the agreement of HRVust measure in time-domain variables.
Interestingly, the agreement of HRVust lnSDNN and lnRMSSD records during the pre-exercise assessment was excellent compared to standard HRV records. However, during the RSA10%decrement protocol, post-exercise HRVust measures have moderate to large levels of ICC value to standard HRV record. Furthermore, a large CV % of post-exercise HRVust measures was observed (lnSDNN = 28.6%–38.8%; lnRMSSD = 49.2%–51.7%). The finding of the present study revealed that the lnSDNN and lnRMSSD HRVust1–2min demonstrated good to excellent relative reliability with the post-exercise HRVcriterion during the RSAstandard and RSA10%decrement. Thus, a minimum of a 2-min record is suggested for the accuracy of post-RSA exercise lnSDNN and lnRMSSD measures. 16 Additionally, the relative agreement of lnSDNN:lnRMSSD ratio was large and very large at the RSAstandard and RSA10%decrement protocols, respectively. These findings somehow coincide with the results of post-exercise time-domain HRVust shown by Esco et al. 4 The time-domain HRV poses an advantage in reproducibility in assessing sympathovagal balance compared to frequency-domain HRV measures during the post-exercise period.4,17 The individual variation of respiratory rate and metabolite removal during the early phase of recovery may underlie a potential factor to large CV % of time-domain HRVust measures. 29
Another finding in this study revealed a positive correlation between post-exercise HRVust indices (lnSDNN and lnRMSSD) and the best sprint time during the RSA10%decrement. It is known that parasympathetic reactivation and decreasing sympathetic activity are critical mechanisms to regulate cardiac-related responses during recovery. 30 Storniolo et al. 31 reported a decrease in symbolic markers of HRV in association with a significant tachycardia and low respiratory sinus arrhythmia after a single bout of 60-m maximal sprint in healthy adults, indicating a strong vagal activation and sustained sympathetic modulation. The shift of sympathovagal balance during the post-exercise period was also evidenced by the time delay and time constant of HR kinetics after the same pattern of exercise. 32 In our study, the lnSDNN showed a significantly positive correlation between the best RSA10%decrement time and all HRVust time segments. Additionally, the lnRMSSD showed a significantly positive correlation between the best sprint time and the HRVust30s and HRVust60s time segments during the RSA10%decrement protocol.
Furthermore, our study exhibited a positive correlation between the best sprint time and the HRVust30s and HRVust60s during the RSA10%decrement protocol when the lnSDNN and lnRMSSD were compared. The best performance during the RSA10%decrement test positively correlates to the lnSDNN and lnRMSSD indices in the first minute post-exercise recovery. Wu et al. 16 reported that the values of the SDNN and RMSSD in the HRVust are significantly different from the 5-min HRV record after the 6, 9, and 12 km/h treadmill running, and the reliability of HRVust is less optimal. Additionally, Hung et al. 17 reported that the post-exercise time-domain HRVust indices (lnSDNN, lnRMSSD, and ratio of lnSDNN : lnRMSSD) after RSA and Yo Yo intermittent recovery level 1 test have an excellent agreement to the standard HRV record. Conversely, Canino et al. 18 reported that the HRVust (less than 5-min record) could not strongly predict aerobic fitness capacity during incremental stationary cycling exercise Our finding is consistent with a recent study that demonstrated the reliability of HRVust60s in the SDNN and RMSSD after an 8-min stationary cycling exercise (14–16 m/s). 18 It should be noted that the lnSDNN and lnRMSSD are predominantly vagal-related HRV makers used to evaluate post-exercise parasympathetic reactivation. 30 The positive correlation between the HRVust60s time segment of lnSDNN and lnRMSSD and the best RSA sprint time indicates a relationship between optimal anaerobic-based shuttle running and post-exercise measure of time-domain HRVust measure during the recovery period. 33 Future studies suggested to examine the interplay between repeated sprint performance and mechanisms of HRVust during an early recovery phase.
Limitation
There are two major limitations in the present study. Firstly, the physical level and variability of training status among the participants may contribute to a large disparity in RSA performance. Secondly, the study results come from participants with athletic backgrounds in team sports, limiting its generalizability to other populations, such as sedentary and individual sports.
Conclusions
In conclusion, an ultra-short-term record of the lnSDNN and lnRMSSD is valid and reliable during the recovery phase after repeated sprint exercises. One-minute stabilization prior to the 60 s HRVust measure is recommended to provide excellent agreement of post-exercise measure when the bouts of RSA increased. The number of bouts performed in the RSA exercise influences validity and reliability of acute post-exercise HRVust records. The positive relationship between post-exercise vagal-related HRV and best RSA performance is warranted.
Footnotes
Acknowledgment
The authors appreciate the study participants.
Author contributions
Conceptualization: Chin-Hwai Hung and Yung-Sheng Chen. Methodology: Wen-An Lu, Jeffrey Cayaban Pagaduan, and Yung-Sheng Chen. Formal analysis and investigation: Wen-An Lu and Yung-Sheng Chen. Writing—original draft preparation: Chin-Hwai Hung, Cheng-Deng Kuo, and Yung-Sheng Chen. Writing—review and editing: Chin-Hwai Hung, Wen-An Lu, Jeffrey Cayaban Pagaduan, Cheng-Deng Kuo, and Yung-Sheng Chen. Supervision: Cheng-Deng Kuo and Yung-Sheng Chen.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant MOST 109-2410-H-845-020 from the National Science and Technology Council, R.O.C. (Taiwan).
Author biographies
Chin-Hwai Hung is an assistant professor of the Department of Physical Education at Fu Jen Catholic University, Taiwan. His research field is football training.
Wan-An Lu is a full professor and Chinese medicine doctor at the College of LOHAS Industry at Fo-Gang University, Taiwan. His research field is Chinese medicine and cardiovascular research.
Jeffrey Cayaban Pagaduan is a postdoctoral researcher at the Faculty of Physical Culture at Palacký University, Czechia and a strength and conditioning practitioner. His research is on sports training and cardiovascular physiology.
Cheng-Deng Kuo is a full professor and a clinical physician of internal medicine at Taipei Veterans General Hospital Hsinchu Branch, Taiwan. His research field includes biomedical engineering, human physiology, and medicine.
Yung-Sheng Chen is a full professor of the Department of Exercise and Health Sciences at the University of Taipei, Taiwan. His research fields are sports training, football sciences, and human physiology.