
Abstract
Introduction
Tooth avulsion is a complex traumatic dental injury which results in the complete displacement of tooth from the alveolar socket, severing the periodontium and dental pulp. Major causes of avulsion injury include cycling accidents, falls, sports injuries, assaults, and violence in kids. The reported incidence of dental avulsion ranges from 1–16% of all the traumatic dental injuries to permanent dentition. 1 After avulsion injury, dental pulp undergoes necrosis due to the severed apical neurovasculature. 2 Eventual necrosis of PDL leads to ankylosis and root resorption. 3 Optimum treatment for an avulsed permanent tooth is immediate re-implantation, the success of which is associated with a myriad of intra-oral and extra-oral factors. 2
Experimental studies prove that PDL viability is crucial to prevent root resorption and ankylosis. 4 Following tooth avulsion, an extended extra-oral drying time increases the likelihood of the PDL tissue undergoing necrosis which increases the probability of root resorption or ankylosis after replantation. 4 Multiple therapeutic and preventative modalities aim at preserving PDL viability and promote tissue regeneration postreplantation. Storing the tooth in a suitable storage media such as milk, saliva, saline, or Hank's Balanced Salt Solution (HBSS) has been observed to improve the outcomes of tooth replantation. 5 However, due to the lack of knowledge, patients (or their guardians or caregivers) store the avulsed tooth in inappropriate media or simply bring them in paper towers which adversely affects the outcomes of tooth replantation. 6 Therefore, recently, topical application of antiresorptive drugs and growth factors has been suggested to improve the outcomes of tooth replantation.7,8
Fibroblast growth factor-2 (FGF-2), also called basic fibroblast growth factor (bFGF), is a growth factor and a signaling protein that is generally associated with cells derived from mesoderm. 9 Studies have revealed that FGF2 has several important functions. FGF2 plays an important role in wound healing, tissue repair, and embryonic development.10,11 Moreover, it also possesses angiogenic and osteogenic properties. 12 The growth factor has also been immunolocalized in the human and animal periodontium, where it plays a vital role periodontal healing, angiogenesis, and bone regeneration.13,14 Therefore, studies have suggested that FGF2-based biomaterials can improve outcomes of periodontal regeneration. 15 Similarly, clinical trials also support the use of FGF-2 for periodontal regeneration.16,17 Recently, animal studies have indicated that FGF2-containing pre-replantation treatment may promote periodontal regeneration and prevent root resorption and ankylosis in replanted teeth.18,19 However, to date, no systematic review has been published summarizing and critically analyzing the studies conducted. Therefore, the aim of this review is to systematically summarize the literature concerning the influence of FGF-2 on the root resorption, tissue regeneration and prevention of ankylosis in a reimplanted tooth.
Materials and methods
Focused question
The protocol was produced during the planning of the review. It is available on 10.17605/OSF.IO/6NZK5. Using the Participants, Intervention, Control and Outcomes (PICO) 20 protocol described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 21 statement, the following research question was constructed: “Does application of FGF-2-based treatments reduce root resorption in replanted teeth?”.
Selection criteria
The inclusion criteria for the studies were: (i) animal studies, (ii) studies focusing on replantation of teeth, (iii) studies on using FGF2 as a pre-replantation treatment, and (iv) studies in English. Reviews, articles only describing in vitro outcomes, commentaries, letters to the editor, and short communications were excluded.
Search methodology
An electronic search was conducted via PubMed/Medline, Google Scholar and ISI Web of Knowledge, EMBASE using the Medical Subject Headings (MeSH) terms “Basic fibroblast growth factor,” “Fibroblast growth factor-2,” “tooth replantation,” “dental trauma,” “tooth avulsion,” “root resorption,” “replacement resorption,” and “replantation” for studies published between January 2001 and June 2021 by two authors, SN and FM, independently. Any disagreements were solved by discussion. A secondary hand-search was conducted by reading the reference lists of the articles meeting the inclusion criteria for additional studies relevant to this review.
Data extraction
Three investigators (SN, FM, and ZK) extracted and tabulated the data from each of the included studies according to (1) animal models used, (2) the number of animals used, (3) study duration, (4) site of FGF-2 application, (5) extra-oral drying time investigated, (6) treatment groups (controls and experimental), (7) formulations and concentrations of the growth factors used, and (8) the general outcomes. Any disagreements were solved by discussion.
Quality assessment of studies
The quality of methodologies employed in the studies was assessed by means of the SYRCLE's risk of bias tool for animal studies. 22 Two investigators conducted this individually, solving any disagreements via discussion. Various aspects of the title, abstract, methodology, results, and discussion were analyzed and assigned quality scores to give an overall score out of Low, Moderate or High biases in the following areas: sequence generation, baseline characteristics, allocation concealment, random housing, blinding, random outcome assessment, completeness of reported data, and other sources of bias.
Results
Search results
After elimination of duplicate items, the primary search resulted in 247 articles. After exclusion of irrelevant articles 37 papers were screened. After exclusion of further 23 articles on the basis of titles and abstracts, full texts of 14 articles were read to exclude additional irrelevant studies. No additional articles were found after scanning the reference lists of the full texts. After exclusion of five full-text articles (two reviews,23,24 one no outcomes of interest, 25 one ex vivo study design, 26 and one in which FGF-2 was not used 27 ) and nine animal studies were included in this review for qualitative analysis.17–19,28–33 The PRISMA flow diagram (Figure 1) illustrates the search methodology employed for this review. The interexaminer reliability (kappa) score was calculated to be 0.81. The nine included studies are listed in Tables 1 and 2.
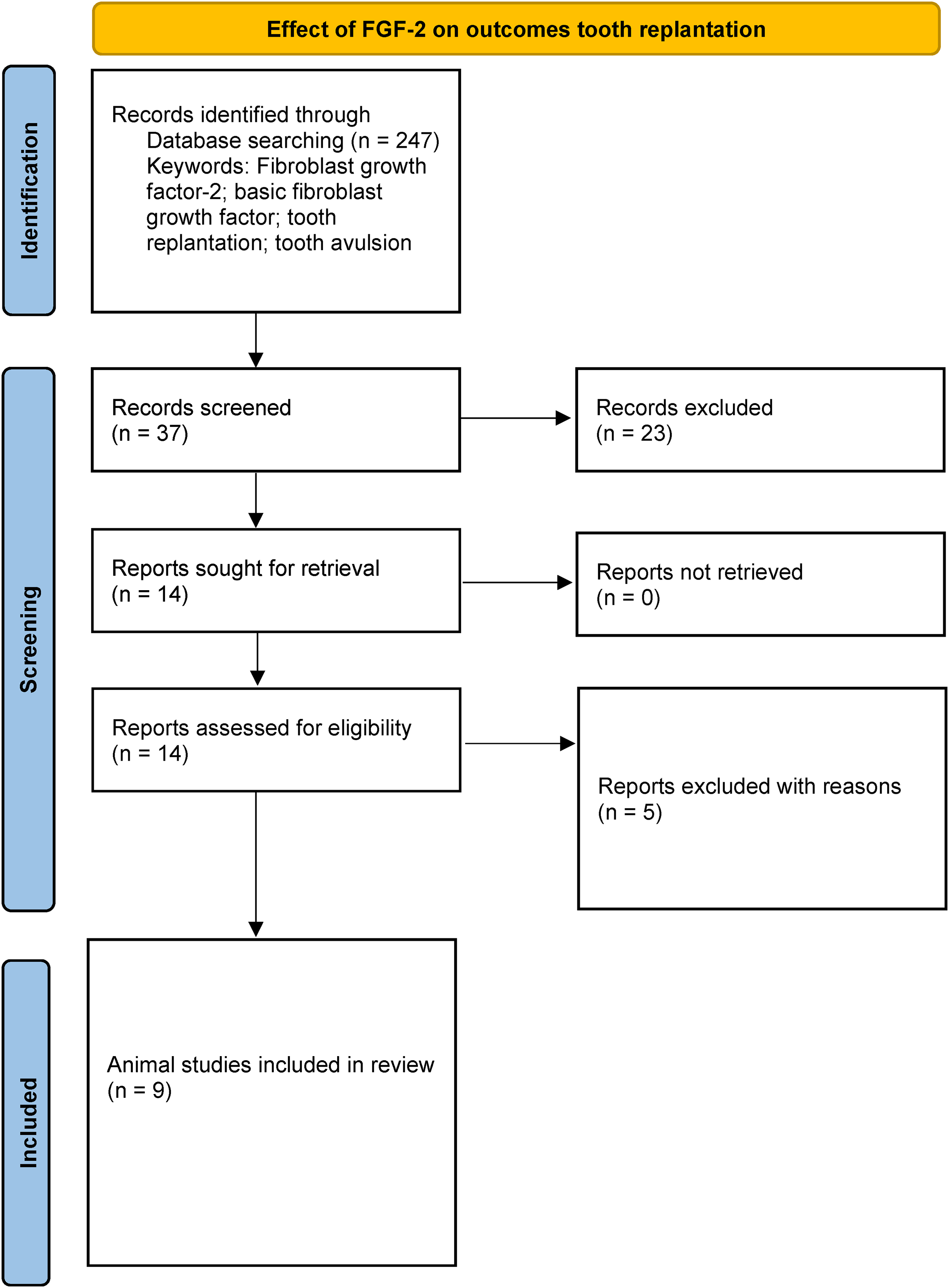
Effect of FGF-2 on outcomes tooth replantation. FGF-2: fibroblast growth factor-2.
The general characteristics and outcomes of the studies included in this review.

bFGF: basic fibroblast growth factor; BMSCs: bone marrow-derived stem cells; EMD: Enamel Matrix Derivative; FGF-2, fibroblast growth factor-2; HPC: hydroxypolymethylcellulose; PEI: polyethylenimine; pFGF-2: plasmid DNA for FGF-2; DL: diode laser; PLGA: poly-L-glycolic acid; SDF-1: stromal cell-derived factor 1.
Results of the risk of bias assessment using SYRCLE.

General characteristics of selected studies
All studies included were animal studies.17–19,28–33 Monkeys were used in one study, 18 seven studies used beagle dogs,17,19,28–30,33 one study used rats, 32 and one study used mongrel dogs. 31 The number of animals reported varied from 4 to 50.17–19,28–33 In one study, scaffolds containing plasmid FGF-2 (pFGF-2) were wrapped around roots of replanted teeth 19 and in another one, the efficacy of FGF-2 in collagen gel was compared was compared to that of collagen gel alone. 17 In all nine studies, teeth were replanted into the jaws of the animals.17–19,28–33 In another study, a combined use of FGF-2 and stromal differentiating factor-1 (SDF-1) was compared to that of saline controls. 33 The duration of studies ranged from 14 days to 12 weeks.17–19,28–33 Extra oral drying time before replantation, which ranged from 60 min to 2 h, was investigated in 4 studies.18,19,29,32 In five studies, the effect of FGF-2 on only immediate replantation was investigated.17,28,30,31,33 In one study, defects were created on the root surface to simulate periodontal damage. 17 The general characteristics, including the treatment groups and concentrations of FGF-2 used in the studies, are provided in Table 2.
Main outcomes of selected studies
In all examined studies, histological assessments were conducted following the sacrificial process of the animals.17–19,28–33 Within the majority of the nine studies systematically reviewed, it was consistently observed that FGF-2 demonstrated a favorable impact on the regeneration of tissues surrounding the roots of replanted teeth when compared to alternative treatment groups.17,28–33 Notably, a singular study, comparing the effects of FGF-2 and fibrin glue with fibrin glue alone, did not reveal any significant differences between the two treatment modalities. 18
In instances where FGF-2 was found to enhance the outcomes of tooth replantation, there was concurrent improvement in periodontal regeneration,28,29 cementogenesis,29,31 and the reinsertion of PDL fibers. 32 Furthermore, FGF-2 exhibited preventive effects against root resorption19,28–30,32 and demonstrated an increase in collagen formation. 19 In the investigation conducted by Carvalho et al., 32 FGF-2 was found to promote the reinsertion of PDL fibers, both with and without the application of diode laser therapy.
Results of quality assessment
The detailed results of the quality assessment are presented in Table 2. Overall, six studies were graded as high,17,29–31,33 two studies as moderate,18,19 and one as low. 32
Discussion
FGF-2 plays a vital role in promoting the repair of periodontal tissues, including the gums, ligaments, cementum, and bone. FGF-2 stimulates cell proliferation, angiogenesis (blood vessel formation), and the production of extracellular matrix components. It also encourages the differentiation of stem cells into bone and cementum-forming cells while reducing inflammation. FGF-2's multifaceted actions contribute to the regeneration of damaged periodontal tissues, making it a promising candidate for therapies aimed at treating periodontal diseases and injuries.9–11
The optimum treatment for an avulsed tooth is immediate replantation. 33 However, in many cases, by the time the avulsed tooth is brought into the dental clinic, it may have already undergone extended periods of drying time. Additionally, storing the avulsed tooth in inappropriate media or wrapping in paper towels further adversely affects the outcome of replantation. 34 The prognosis of a replanted avulsed tooth also includes factors such as the degree of mechanical strain to the PDL and its cell viability and extent of dehydration.34,35 Furthermore, extended periods of extra-oral time also increase the probability of bacterial contamination. 36 While the condition of PDL is crucial for the replanted tooth to survive replantation, extent of revascularization of the dental pulp also determines the success of the procedure. 37 Studies have indicated that if the extra oral drying out time exceeds 60 min, it can lead to extensive PDL cell necrosis and extension of damage side in periodontal tissue over root surface, thus having a detrimental effect on prognosis of replantation. 2 Several storage media, such as milk and saliva have been observed to improve the prognosis of replantation, but most people are not aware about them. 38 Although HBSS and saline are considered superior to milk and saliva, they are not readily available for in-home management of avulsed teeth. Moreover, due to the lack of awareness about immediate replantation, by the time the patient is brought to the clinic, the PDL may have already necrosed in many cases. Therefore, the effects of topical applications of several drugs, 8 bioactive materials, 33 and growth factors 39 on the outcomes of replanted teeth have recently been studied.
FGF-2 is a cytokine with a distinctive molecular structure. 9 It is a single chain polypeptide, a heparin binding protein which stimulates cell proliferation, differentiation and also promotes extracellular matrix generation. Thus, it plays an important role in wound healing tissue regeneration. 23 Prior studies have indicated the FGF-2 may induce angiogenesis and bone regeneration. 40 Therefore, gels containing FGF-2 have been used for periodontal regeneration. 41 Both, clinical 16 and animal studies 42 have demonstrated the osteogenic and periodontal regenerative potential of FGF-2. It exhibits angiogenic activity and has reported to effectively regenerate PDL, new cementum with Sharpey's fibers, structurally and functionally oriented PDL fibers, and alveolar bone in animal models. 43 Studies also suggest that topical application of FGF-2 might stimulate multipotent mesenchymal cells inside the PDL and potentially induce periodontal regeneration. 44
Due to the abovementioned regenerative abilities of FGF-2, it has been studied as a topical reagent to prevent root resorption and ankylosis, and to promote the regeneration of periodontal tissues after replantation of avulsed teeth. 19 Indeed, studies reviewed in this review indicate that FGF-2 may also induce cementogenesis, re-insertion of PDL fibers and bone regeneration.28–32 However, only four of the nine studies reviewed in this systematic review investigated the effect of FGF-2 in improving the outcomes of delayed replantation18,19,29,32 and, in others, teeth were replanted immediately. Since delayed replantation generally leads to worse outcomes compared to immediate replantation, 1 additional stem cell sources or cell-homing mechanisms may need to be employed to overcome this. In many cases, the avulsed tooth has already undergone extra-oral drying time exceeding 60 min, indicating beyond which the survival of the PDL becomes unlikely. 2 Nonetheless, in three out of the four studies in which delayed implantation was carried out, FGF-2 does seem to assert a positive impact on PDL regeneration, bone regeneration, cementogenesis, and reinsertion of PDL fibers.28–32 This suggests that pretreatment with FGF-2 prior to replantation may improve the survival rate of the replanted teeth.
Burst-release of growth factors may have an initial positive impact but for long-term periodontal regeneration, a growth factor needs to be released into the defect in a slow and sustained fashion. For periodontal regeneration, FGF-2 has been mostly used in a hydroxypropyl methylcellulose (HPC) carrier gel. 45 HPC is a biodegradable and biocompatible cellulose-based carrier and can release FGF-2 into the tissues for periodontal regeneration. 43 Even among the studies that were reviewed, only two studies mentioned using HPC as a carrier gel29,32 and in one study, the composition of the gel was not mentioned. 28 However, studies indicate that HPC-based FGF-2 gels do not release the growth factor beyond first few hours of application. Therefore, there is a need for a drug delivery system that releases FGF-2 in a slow and sustained manner.
Contemporary regenerative materials function as scaffolds that recruit native progenitor cells to induce tissue regeneration. 45 Tissue regenerative scaffolds provide support for the cells to grow and can also be used to deliver bioactive growth factors to further induce tissue regeneration. 46 Although many materials have been observed to induce bone regeneration, PDL regeneration is still a challenge that has yet to be overcome. 47 Recent studies have attempted to achieve PDL regeneration by using regenerative cytokines encapsulated in scaffolds. 48 Similarly, the study Jiang et al. 19 used a fibrous scaffold containing plasmid FGF-2 DNA to deliver FGF-2 into the tissues. However, although scaffolds did improve periodontal regeneration when compared to no scaffolds after delayed replantation, there was no statistical difference between scaffolds containing plasmid FGF-2 DNA and those without any growth factors which suggests that it is perhaps the nanofibrous structure of the scaffold that promoted periodontal regeneration rather than the plasmid FGF-2 DNA. A nanofibrous scaffold mimics the extracellular matrix (ECM) to promote fibroblast attached and proliferation.49,50 Therefore, using scaffolds holds potential in improving the outcomes of delayed replantation of avulsed teeth.
Since none of the studies reviewed in this study were conducted on humans, it is not possible yet to determine the clinical efficacy of using FGF-2 to improve the outcomes of tooth replantation. Although animal models provide a better experimental design to assess the efficacy of a treatment when compared to just in vitro studies, they have several limitations when compared to studies conducted on humans. 51 Firstly, the microflora is different in animals. Additionally, owing to the difference in the magnitude of masticatory forces and dietary habits of human and animals, it is difficult to translate the results of animal studies into clinical practice. There were several sources of bias in the studies reviewed. Investigators were blinded in only two studies.18,32 Similarly, only three studies mentioned some sort of randomization.18,19,32 A combined lack of randomization and blinding may have impacted the outcomes of these studies. Furthermore, none of the studies reported if there were any local or systemic adverse effects of FGF-2. Nonetheless, to the best of authors’ knowledge, no adverse effects of FGF-2 have been reported in literature. Additional shortcomings of the studies are the lack of standardization of the doses and formulations of the FGF-2 used. Hence, it is difficult to compare the outcomes of the studies. Moreover, the maximum duration of study was 12 weeks. 18 Future studies should focus on improving the experimental design and evaluating the dose-dependent effects of the FGF-2 on outcomes of avulsed teeth, and they should be of adequate duration to ascertain the efficacy of FGF-2 in regenerating periodontium after replantation. In particular, we also propose studies of durations of 3 to 6 months with adequate postreplantation observation periods to document any instances of late failures or complications. Also, future studies could compare FGF-2 with other cell-free tissue regenerative in improving the outcomes of tooth replantation. 52
Conclusion
Within the limitations of this study, it may be concluded that FGF-2 may improve the outcomes of delayed replantation of avulsed teeth. However, more long-term animal studies, with improved experimental designs, and clinical trials are required to determine the clinical potential of the growth factor in improving the outcomes of delayed tooth replantation.
Footnotes
Author contribution
SN and FAM were involved in conceptualization; SN and MSKS in methodology; SN and NA in software and formal analysis; SN, AH, ZK, and MSZ in validation and writing—review and editing; SN, FAM, and MSKS in investigation; SN, ZK, AH, and MSZ in resources; SN, FAM, NA, and MSKS in data curation, writing—original draft preparation, and visualization; SN and MSZ in supervision; and SN in project administration. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Shariq Najeeb is an adjunct professor at the University of Western Ontario and the research lead at Evidental Dental Outcomes Research. He has published more than 50 articles in various dental journals.
Farwa Ali Manekia earned her BDS degree with 15 distinctions from Karachi Medical and Dental College. Following a year of practicing dentistry at her alma mater, she served as a general dentist at 'The Dental Sphere' in Karachi, Pakistan for four years. Her research passions converge at the crossroads of regenerative medicine and public health, reflecting her ambition for focused progress in these fields.
Muhammad Shahrukh Khan Sadiq is a dental professional with a BDS from Dow University and an MPhil in the field of Oral Pathology from Ziauddin University. He has over five years of experience at Bahria University Dental College, Bahria University Health Sciences, Karachi, focusing on research and publications in oral health care with 20 national and international publications to his name. Notable achievements include establishing Pakistan's first oral submucous fibrosis cell line and receiving the Best Young Dentist Award in 2022–23 by the Pakistan Society of Oral and Maxillofacial Pathology.
Necdet Adanir (DDS, PhD, MDTFEd) is an alumnus of Hacettepe University's Faculty of Dentistry and earned his PhD in Restorative Dentistry and Endodontics from the Faculty of Dentistry at Selcuk University in 2002. His academic journey led him to Suleyman Demirel University's Faculty of Dentistry, where he began as an assistant professor and was elevated to the rank of associate professor in 2009. From 2010 to 2013, he held the positions of vice dean and head of the Endodontics Department at Gaziantep University. He was the dean of the Graduate School of Health Sciences and the chief physician of the faculty hospital at Suleyman Demirel University. In 2017, he joined the Faculty of Dentistry at King Faisal University, where he has been leading the Department of Restorative Dentistry since. Additionally, he is the Editor-in-Chief of the European Journal of Dentistry. His scholarly contributions include numerous international publications and over 35 presentations at international congresses. He is a member of the Royal College of Surgeons of Edinburg.
Zohaib Khurshid, with qualifications including BDS, MRes, FHEA, MDTFEd, and MFDS RCPS (Glasgow), specializes in Prosthodontics and Dental Implantology. Currently affiliated with the Department of Prosthodontics and Dental Implantology at King Faisal University, KSA. He holds a Dental Education PGCert from Dundee. Recognized globally as a top 2% scientist, he has authored over 200 Scopus indexed papers and edited numerous international books. Additionally, he is a member of the Faculty of Dental Surgery, Royal College of Physicians and Surgeons (Glasgow).
Muhammad Sohail Zafar completed his PhD at the Nottingham Trent University (2011) after obtaining master's degree in Dental Materials from Queen Mary University of London, UK (Distinction level research project; 2007). Currently, he is affiliated with the College of Dentistry, Taibah University, Saudi Arabia, where he has been a faculty member since 2012. Before that (2011–2012), he worked as an associate researcher at Nottingham Trent University, UK. He is a fellow of the Higher Education Academy (FHEA) and Faculty of Dental Trainers, Edinburgh (FDTFEd). Being a research-led academician, he has considerable exposure of teaching, research, and clinic management and the successful implementation of operating procedures in academic and clinical activities. He has substantially contributed to research publications (more than 250 peer reviewed publications since 2013) in the field of dental materials, tissue engineering and clinical dentistry (Scopus h-index of 40; Google Scholar h-index of 55; i10-index of 181). He is an editorial board member for various peer-reviewed journals. His research interests include advanced biomaterials, biomedical sciences, tissue regeneration, nanomaterials and polymeric biomaterials for dental applications.
Artak Heboyan received a bachelor's degree in Stomatology from Yerevan State Medical University after Mkhitar Heratsi (YSMU), Armenia in 2011 and a Master of Science (Qualified as Doctor of Stomatology) degree in Stomatology from the Faculty of Stomatology, YSMU, Armenia in 2013. In 2016, he qualified as a Medical Specialist in the field of “Prosthodontics,” YSMU, Armenia. From 2016 to 2021 he worked at the Central Clinical Military Hospital, Ministry of Defense, Republic of Armenia. From 2018–2021, he was an invited lecturer at The Center of Excellence in Dental Education at YSMU, Armenia. In 2021, he defended and received a PhD in the field of Medicine (Stomatology) at YSMU, Armenia. In 2023, he qualified as a Medical Specialist in the field of “General Dentistry”, YSMU, Armenia. From 2016–2021 he was an assistant professor. Since 2022, he has served as an associate professor at the Yerevan State Medical University after Mkhitar Heratsi, Armenia. Simultaneously, he works as a Dentist-Prosthodontist at the “Art Classic Dent” Dental Centre. Currently, he serves as a reviewer in various peer-reviewed journals and as an editor in BMC Oral Health, PLoS ONE, Frontiers in Oral Health, Journal of Applied Biomaterials & Functional Materials SAGE, Frontiers in Dental Medicine and many more journals.