
Abstract
Introduction
Alexithymia is a personality trait characterized by difficulty in identifying, experiencing, and expressing emotions. It has been associated with a number of mental and physical health problems, including psychosomatic disorders. 1 Alexisomia is a related concept that refers to the difficulty in identifying and describing bodily sensations. 2 It has been proposed that alexisomia may play a role in the development and maintenance of psychosomatic disorders.3,4
The shitsu-taikan-sho scale (STSS) is a 23-item self-report questionnaire that measures alexisomia. 5 Previous studies have validated the STSS in Japanese and Turkish populations, demonstrating its good psychometric properties. 6 However, no studies have assessed alexisomia in the Mongolian population.
Mongolia is a developing country with a unique nomadic culture. Approximately one-third of the Mongolian population lives in rural areas as nomadic herders. It is possible that the subjective perception of alexisomia among Mongolian people may differ from standards in urbanized populations. Furthermore, there has been a global shift in disease burden from communicable to noncommunicable chronic diseases in recent decades, affecting developing countries like Mongolia more prominently than developed countries.7,8 Mental and neurological disorders, including psychosomatic disorders, constitute the majority of these noncommunicable chronic diseases. However, no studies have assessed alexisomia in the Mongolian population.
Therefore, the aim of this study was to evaluate the psychometric properties of the Mongolian version of STSS in a nonclinical population. This study will provide valuable information about the validity and reliability of the Mongolian version of STSS. This information can be used to develop and implement interventions to improve the mental and physical health of Mongolians.
Methods
Study design and participants
We validated the Mongolian version of STSS in a non-clinical setting. The sampling size was calculated to be 460 using the criteria that each item needs a minimum of 20 participants to be assessed, by MacCallum et al. 9 Considering a response rate of 60%, 644 individuals were invited to participate in the survey. All participants had to be older than 18 years old and Mongolian-speaking. Participants were excluded according to the following criteria: (i) who currently had an established diagnosis by physicians; (ii) who had a history of a traumatic injury. 10 The participants were entirely undergraduate students from various medical universities and attended the second year. Written informed consent was obtained from all participants before starting the survey. Nonrandom sampling was carried out. A total of 676 students were approached to complete the validation study, and 137 of those approached either refused to take the study or had missing data. The remaining 539 participants were included in the final analysis.
Data collection
The data were obtained in Mongolian universities during September–December 2021. The study was conducted in the official language (Mongolian). All participants completed the paper-based STSS. All 539 participants completed the STSS questionnaire again within 2 weeks of the initial administration to assess test-retest reliability. Prior to the study, all field study members completed a data collection training program. The training covered how to approach participants, ask for permission, explain the written consent, register participants, collect questionnaires, score the questionnaires, and interpret the results for participants.
Measures
Alexisomia among study participants was evaluated using the STSS questionnaire. This is a 23-item self-administered questionnaire rated on a 5-point Likert scale, which provides a total score ranging between 23 and 115. 5 The STSS subscales include: (1) difficulty identifying bodily feelings (DIB), overadaptation (OA), and lack of health management (LHM) based on bodily feelings. The original DIB consists of nine items (items 1, 5, 6, 10, 12, 14, 15, 18, and 19) which describe unawareness of normal and abnormal signals of the body homeostasis and allostatic load. The original OA includes six items (items 3, 7, 13, 17, 20, and 22), which refer to a tendency to prioritize social demands by neglecting bodily feelings. The original LHM (reverse-scored items 2, 4, 8, 9, 11, 16, and 21, but 23) extends to poor health care for demands from bodily feelings. The total score is the sum of responses to all 23 items, while the score for each subscale factor is the sum of the responses to that subscale. The original version of STSS does not have established cut-off scores. Scores are scaled in a positive direction, with higher scores indicating greater alexisomia.
We completed the translation and adaptation of the STSS into Mongolian according to the established procedure. 11 We translated the STSS into Mongolian based on the guidelines of cross-cultural adaptation via the following steps: initial translation of the items into Mongolian was performed independently by two translators (one holding a PhD degree in medicine, another holding a PhD degree in neuroscience), and the translation was combined into one version with a focus on sentence structure, word choice, and best fit to the original version. A subsequent pilot test examined the understanding of items, the ability to answer, and the meaningfulness of the scale as a whole. The pilot testing was performed in a group of 18 undergraduate students at a medical school. Back-translation was performed independently by two translators unfamiliar with the original STSS and revealed no meaningful disagreement with the original version. Finally, the expert committee reevaluated item translation based on the pilot test and reviewed the back-translation process before administering the Mongolian version of STSS to study participants.
We also collected the demographic characteristics of the participants, including the gender, age, and housing arrangement.
Statistical analysis
The normality of the data was evaluated using the Kolmogorov-Smirnov test. Differences between the two groups were examined using the Mann-Whitney U-test for continuous data. Descriptive data were presented as number (n), percentage (%), mean, and standard deviation (SD).
The reliability of the questionnaire was assessed for internal consistency using Cronbach's α (good, ≥ 0.8; acceptable, ≥ 0.7; marginally acceptable, ≥ 0.6). 12 To evaluate how well each item is measuring the underlying construct that the STSS is intended to measure, we employed the item-scale correlation analysis. A high item-scale correlation indicates that the item is measuring the construct consistently, while a low item-scale correlation indicates that the item is not measuring the construct consistently. 13 To evaluate external reliability, a test-retest procedure was performed at a 2-week interval. The intraclass correlation coefficients (ICC) were calculated using a two-factor mixed-effects model. ICC of <0.5, 0.5–0.75, 0.75–0.9, and >0.9 were considered to have poor, moderate, good, and excellent test-retest reliability, respectively. 14
Further, questionnaire validity was evaluated by exploratory factor analysis (EFA) using principal likelihood analysis with oblimin rotation. Factor analysis suitability was examined by the Bartlett test of sphericity (p < .001) and Kaiser-Meye-Olkin (KMO) test of sampling adequacy (KMO > 0.65), followed by determining the number of relevant factors via eigenvalue analysis. 15 The factors with eigenvalues >1 were assumed to be meaningful and retained for rotation.
Confirmatory factor analysis (CFA) was performed using the maximum likelihood estimator to confirm the EFA results. The overall model fit was assessed using the chi-square test, and alternative fit indices with the following cut-offs for acceptable fit as follows: < 0.05 for the root mean squared error of approximation (RMSEA), ≥ 0.8 for the comparative fit index (CFI) and Tucker-Lewis index (TLI), and ≥0.40 for the factor loading. 16
A receiver operating characteristic (ROC) curve and area under curve (AUC) were constructed to evaluate the diagnostic capacity of different cut-off points for STSS to predict the abnormal alexisomia for each participant. To create an ROC curve, we adopted the statistical analysis described in a previous study. 17 Briefly, we used a cut-off point of 72 (1 SD above the mean score) to dichotomize the total score variable measured at the retest procedure. Using the new nominal variable, we evaluated the screening ability of the STSS scores at a range of cut-off points to create ROC curves. The optimal cut-off point was determined by the maximum value of the Youden index (J > 0.5), which indicates the maximum sum of the sensitivity and specificity, of an ROC curve. 18
Statistical significance was set at p < .05, and all tests were two-tailed. Data are presented as means ± standard deviation with a 95% confidence interval (CI). Data were analyzed using JAMOVI v.2.2.5, except for the ICC and CFA, which were performed using IBM SPSS v.21 and Amos v.26, respectively.
Ethics approval and consent to participate
All procedures performed in this study were done so in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments. 19 The design and methods were reviewed and approved by the ethics committee at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia (number: MNUMS 2021/З-06). This study was not a trial and did not require registration. Written informed consent was obtained from all participants.
Results
Participant characteristics and preliminary analysis
Five hundred thirty-nine individuals participated in this study, of whom 59.9% (n = 355) were women. This rate was relatively close to that of the general population of Ulaanbaatar, where 53.9% of the population was female in 2021. 20 The mean age of the sample was 21.7 ± 1.5 years (age range: 18–25 years). All participants were undergraduate students residing in Ulaanbaatar. Regarding housing arrangement, 36.6% (217) resided with their family, while 63.4% (376) lived in dormitories.
The distribution of the data was nonparametric for all subscales and the total score (DIB: p = 0.008, OA: p = .042, LHM: p = .039, total score: p = .023). After data collection, two items that showed a strong floor effect were eliminated (Supplemental Table 1). The remaining 21 items built the final Mongolian version of STSS that was further examined for its psychometric properties (Supplemental Table 2).
The total score of STSS was 61.1 ± 10.5, that did not differ between the sexes and housing arrangement (p = .508 and p = .886, respectively, Mann-Whitney test). The subscale scores of STSS were 18.6 ± 5.72, 18.8 ± 4.03, and 23.7 ± 4.11 for DIB, OA, and LHM, respectively, which did not differ by sex or housing arrangement. Possible range scores for the STSS were 7–35 for each subscale and 21–105 for the total score.
Exploratory factor analysis
EFA using the oblimin rotation and principal likelihood extraction method for 21 items identified three components with eigenvalue greater than 1, as presented by the scree plot in Figure 1A.

Factor analysis and ROC for the 21-item Mongolian version of STSS (n = 539). (A) Scree plot, (B) confirmatory factor analysis, and (C) receiver operating curves for the three-factor model of the Mongolian version of STSS.
Furthermore, the results of EFA indicated a three-factor solution (Table 1).
Exploratory factor analysis of the Mongolian version of STSS (n = 593).

The principal axis factoring extraction method was used in combination with the oblimin rotation; * a reverse scaled item.
Abbreviations: DIB: difficulty in identifying bodily feeling; LHM: lack of health management; OA: overadaptation; STSS: shitsu-taikan-sho scale; RMSEA: root mean squared error of approximation; TLI: Tucker-Lewis index.
Items with factor loadings ≥0.40 on the dimensions were retained, and these factors accounted for 40.9% of the total variance. KMO and Bartletts test results were 0.916 and p < .001, respectively, indicating that the data obtained were suitable for factor analysis. RMSEA was 0.049, and TLI was 0.929 for the overall model fit (χ2 = 372, p < .001). The results of the EFA showed a good fit with the model.
Additionally, we conducted EFA on participants who lived with their families (RMSEA = 0.046, TLI = 0.932, χ2 = 225, p < .001; KMO = 0.892).
Confirmatory factor analysis
We applied a three-factorial measurement model using CFA to evaluate how well the three subscales were combined to identify the underlying latent construct of STSS. As shown in Figure 1B, the arrows are the factor loadings, representing the direct effects of the indicators on the latent STSS. The value ranged from 0.01 to 0.83 for the correlation coefficients between the subscales and from 0.39 to 0.80 for the standardized regression weights. The squared multiple correlations were 0.15–0.63, whereas the measurement errors were represented from e1 to e21. The results of CFA using the maximum likelihood method indicated a good fit with the model: χ2 = 703, p < .001, RMSEA = 0.068, TLI = 0.861, CFI = 0.876, SRMR = 0.074.
Additionally, we conducted CFA on participants who lived in a dormitory (χ2 = 383, p < .001, RMSEA = 0.067, TLI = 0.863, CFI = 0.879, SRMR = 0.078).
Internal consistency and test-retest reliability
Reliability analyses included inspecting Cronbach's α to determine internal consistency and item-to-rest correlations to determine external reliability (Table 2).
Internal consistency and test-retest reliability of the Mongolian version of STSS (n = 539).
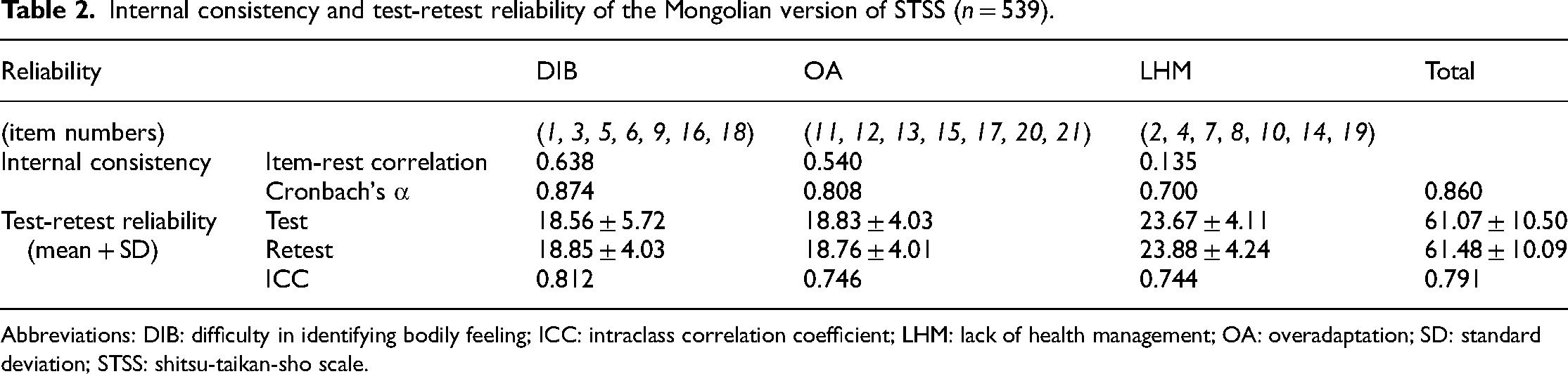
Abbreviations: DIB: difficulty in identifying bodily feeling; ICC: intraclass correlation coefficient; LHM: lack of health management; OA: overadaptation; SD: standard deviation; STSS: shitsu-taikan-sho scale.
The Cronbach's α coefficients of the STSS subscales were as follows: DIB, 0.874; OA, 0.808; and LHM, 0.700. The overall Cronbach's α coefficient of the STSS questionnaire was 0.860. These results indicated good internal consistency of the STSS.
A total of 539 participants completed the STSS within 2 weeks of initial administration to assess test-retest reliability. Results from ICC analyses showed that the total score (0.791) showed good reliability, while the results of the subscales (0.744–0.812) indicated moderate to good reliability.
Item-scale correlation
We analyzed the correlation of each item with its corresponding subscale (corrected item-total correlations) and interitem correlations between the subscales (Table 3).
Item-scale correlation of the Mongolian version of STSS (n = 593).
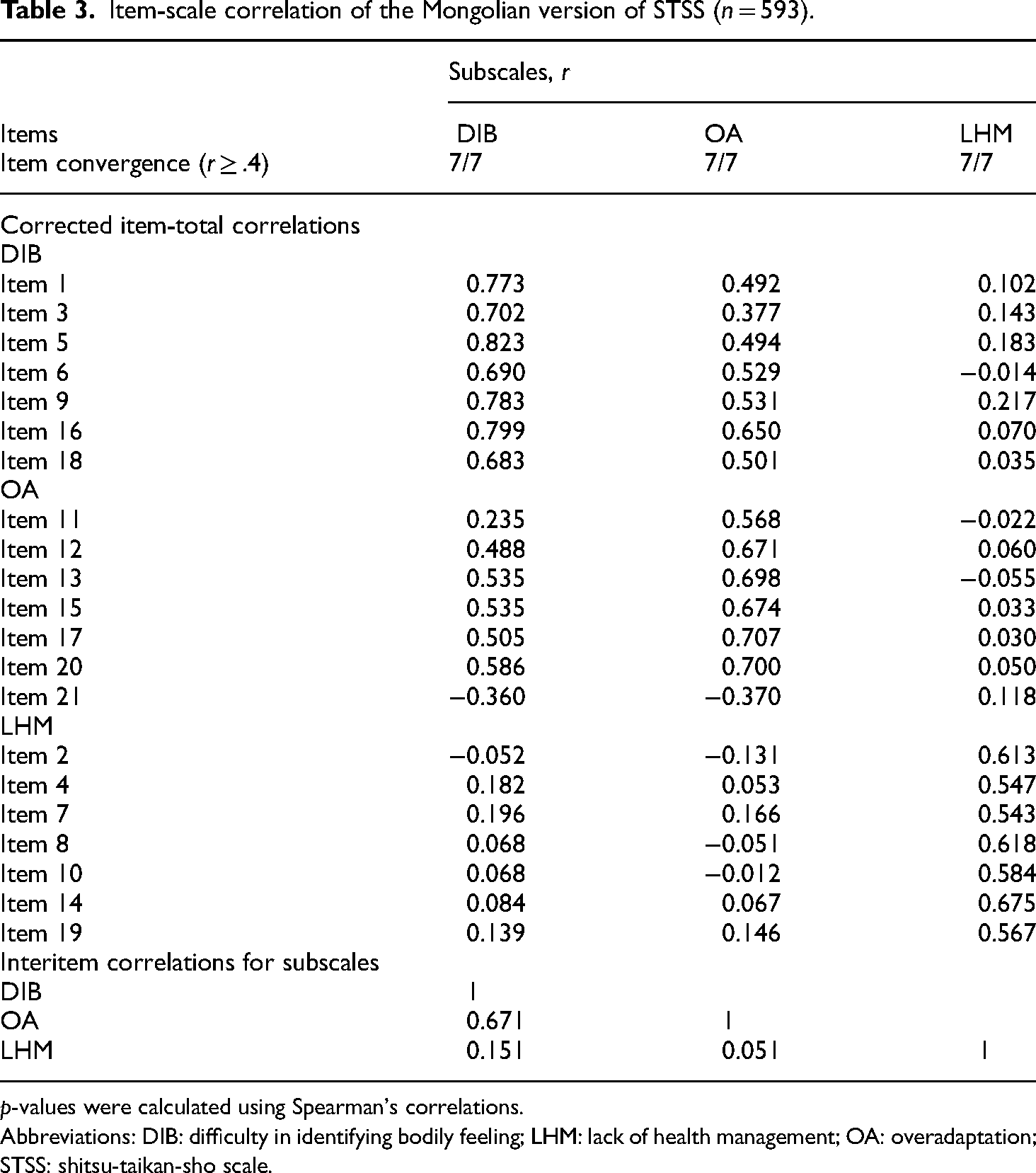
p-values were calculated using Spearman's correlations.
Abbreviations: DIB: difficulty in identifying bodily feeling; LHM: lack of health management; OA: overadaptation; STSS: shitsu-taikan-sho scale.
We expected each item to be more strongly correlated (r ≥ .4) with its corresponding subscales than with the other subscales. In line with this, no items correlated more strongly with another subscale than with its corresponding subscale. Therefore, 21 out of 21 items (100%) met the criteria for item convergence. These results support the existence of a three-factor structure.
ROC curve and cut-off points
The ROC curve in Figure 1C describes the sensitivity and specificity of the three subscales and the total score of STSS in this study to predict alexisomia. AUC values were 0.81, 0.74, and 0.64, for DIB, OA, and LHM, respectively. As indicated by the maximum values of the Youden index, the cut-off points were 22, 21, and 23, for DIB, OA, and LHM, respectively. The cut-off point for the STSS total score (AUC: 0.83) was 69 yielding a sensitivity of 68% and a specificity of 84%. The maximum value of the Youden index was defined by the J statistics, indicating the optimal cut-off scores. The range of cut-off scores with the respective sensitivity and specificity for the Mongolian version of STSS were represented in Supplemental Table 3.
Discussion
The study suggests that the Mongolian version of the STSS showed good validity and reliability for measuring alexisomia in a nonclinical population in Mongolia. The results indicated that the Mongolian version of STSS had good internal consistency and test-retest reliability. A previous validation study for STSS conducted in a clinical population reported that Cronbach's α values were acceptable (0.7–0.84) for all domains. 5 Compared with this result, our results showed a high level of reliability (> 0.8) in terms of internal consistency. Furthermore, the strong test-retest reliability results (> 0.7) suggested that the construct being measured was consistent over time. Therefore, this study provided another reliable source to compare the STSS scores for a nonclinical population.
Construct validity was assessed. CFA of the Mongolian version of STSS confirmed a three-factor structure, the same as the original factorial structure of the instrument. The EFA suggested that a three-factor model was appropriate and potentially equivalent in terms of factor loadings and factor correlations among the study sample. Of note, we had to remove two items from the original 23-item version (specified in Supplemental Table 1). The reasons were, first, their response frequency showed high floor effects, and furthermore, they showed low factor loadings in the rotated component matrix, resulting in a high RMSEA value for the model fit analysis. Accordingly, we obtained a three-factor model with 21 items for better results. After EFA, some differences in item positions in the subscales emerged compared to the original STSS subscales. A total of four DIB items were moved to OA, whereas three OA items were moved to DIB. However, these shifts might be reasonable because some items in both DIB and OA subscales are interchangeable behaviors that are triggered either due to OA or DIB. 21 In contrast, only one item from LHM was moved to OA based on a slight difference in loading score. The correlations between the subscales reflect these relationships as well. DIB and OA are strongly correlated, whereas LHM did not correlate with both of them. However, the fit indices for the two-factor model by EFA were not as good as those for the three-factor model (RMSEA = 0.068, TLI = 0.861, χ2 = 629). Therefore, we retained the three-factor model, which is more consistent with the original construct of the STSS. Furthermore, the item-scale correlation results showed that all items had higher item-total correlations with their corresponding domains than with other domains. These findings supported the three-factor model of the instrument in a nonclinical population.
Previous research has suggested that it may be necessary to conduct EFA and CFA on two independent samples to account for potential differences in the factor structure of a measure across different populations. 22 However, we found that the EFA and CFA results on the same data were similar to the EFA and CFA results on two separate data sets that were divided by living conditions. This suggests that the STSS is a valid and reliable measure of alexisomia, regardless of living conditions.
The STSS total score and subscale scores were relatively higher than the scores reported in previous Japanese studies.5,23,24 This result is noteworthy due to the reduced item count in the Mongolian version of the STSS, compared to its original Japanese version, and the use of healthy participants, in contrast to the previous studies which utilized patients from clinical settings. The observed disparity may stem from cultural differences, as more than a third of Mongolian citizens lead a nomadic lifestyle, distinct from an urbanized lifestyle. 25 Another contributing factor might be the fear and anxiety instigated by the COVID-19 pandemic that peaked during the research.26–28 This phenomenon might have influenced higher scores in specific symptom-related items, such as fever or fatigue. Further investigation with a cross-cultural design is required to clarify the discrepancy.
The present study has provided cut-off scores to facilitate quantification of both the total and subscale scores of the STSS, thereby serving as a valuable tool for comparing STSS scores among diverse populations and approximating the prevalence of alexisomia. Although the maximum Youden index for the total score was above 50%, the subscale scores, particularly for LHM, were below 50%. Therefore, we recommend using it as a continuous measure.
Overall, introducing an alexisomia scale is of great significance in enhancing diagnostics, care, and treatment of psychosomatic disorders, although alexisomia is not a medical diagnosis like diabetes or major depressive disorder. Psychosomatic disorders, particularly those associated with stress, frequently manifest alexithymia and alexisomia. If left unidentified, it can exacerbate these disorders and impair treatment outcomes. The STSS can provide medical professionals with a reliable method for detecting and diagnosing alexisomia, allowing for the customization of treatment interventions geared towards psychosomatic disorders like anxiety, depression, and eating disorders. Furthermore, introducing STSS can foster more comprehensive research in this area, thus improving the understanding and management of psychosomatic disorders.
The main limitations of this study were: (1) as the participants were recruited from only young students, the population surveyed did not represent the entire Mongolian population; (2) although construct validity was assessed, this study did not examine the incremental, discriminative, and criterion validity; (3) the EFA and CFA were not conducted on two independent samples.
Despite these limitations, this is the first study to evaluate the psychometric properties of the STSS in the Mongolian language within a nonclinical population. To further assess the sensitivity and specificity of the instrument, the assessment needs to be conducted in both population-based and hospital-based settings using a longitudinal design. To improve the validity of the instrument, future studies should compare the STSS scores with other relevant measures.
Taken together, this study validated the STSS in Mongolia and provided an assessment of its strengths and weaknesses for future work on alexisomia. By demonstrating good internal consistency and external reliability, the current study has supported the construct validity of a three-factor model.
Conclusion
The 21-item Mongolian version of STSS demonstrated evidence of good reliability and validity for assessing alexisomia in a nonclinical population in Mongolia. This suggests that the Mongolian version of the STSS may allow for the comparison of alexisomia among adults in Mongolia with those in other countries.
Ethics approval and consent to participate
All procedures performed in this study were done so in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments. The design and methods were reviewed and approved by the ethics committee at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia (number: MNUMS 2021/З-06). This study was not a trial and did not require registration. Written informed consent was obtained from all participants.
Supplemental Material
sj-docx-1-sci-10.1177_00368504231225075 - Supplemental material for Psychometric properties of the Mongolian version of shitsu-taikan-sho (alexisomia) in young adults
Supplemental material, sj-docx-1-sci-10.1177_00368504231225075 for Psychometric properties of the Mongolian version of shitsu-taikan-sho (alexisomia) in young adults by Battuvshin Lkhagvasuren, Enkhzaya Batkhuyag, Enkhnaran Tumurbaatar, Tserendolgor Urtnasan, Delgermaa Tsengel, Gantsetseg Tumur-Ochir and Takakazu Oka in Science Progress
Footnotes
Author contributions
TO and GT designed the study. BL and GT completed the interpretation of data, data analysis, drafting the manuscript, and revision of the manuscript. EB and ET contributed to data collection and the interpretation of data. TO provided critical advice and contributed to the revision of the manuscript. All authors reviewed the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported in part by a grant from the Mongolian National University of Medical Sciences (2020/03–05 to BL).
Supplemental material
Supplemental material for this article is available online.
Author biographies
Battuvshin Lkhagvasuren (MD, PhD) is the Director of the Brain Science Institute at the Mongolian National University of Medical Sciences, and also the Advisor to the Brain and Mind Research Institute of Mongolia. His work involves investigating thermoregulation, neuroinflammation, and brain-related disorders. He is also interested in understanding the underlying mechanisms of chronic fatigue syndrome and identifying effective treatments for this condition.
Enkhzaya Batkhuyag (MSc) is a graduate student in the Department of Psychology at the School of Public Health, Southern Medical University, China. Her studies focus on adaptability and psychological distress among young adults, shift workers, and medical professionals.
Enkhnaran Tumurbaatar (MD, MSc) is the Head of the Clinical Neuroscience Research Cluster at the Brain and Mind Research Institute. She has studied touch perception, and is currently investigating the clinical characteristics of sleep disorders and stress-related disorders.
Tserendolgor Urtnasan (MD, PhD) is an Assistant Professor in the Department of Psychiatry at Etugen University, Mongolia. She conducts research on the effects of physical exercise on mental distress and adaptation in migrants.
Delgermaa Tsengel (MSc) is an Assistant Teaching Professor in the Department of Medical Education at the School of Medicine, National University of Medical Sciences, Mongolia. Her research interests are attention, fatigue, and burnout among medical students.
Gantsetseg Tumur-Ochir (MD, PhD) is the Head of the Department of Mental Health Surveillance at the National Center for Mental Health, and a Consultant Physician in psychiatry at the University Hospital of the Mongolian National University of Medical Sciences. She has carried out research on the epidemiology and clinical characteristics of paranoid schizophrenia and bipolar disorder. Her research interests include sleep, stress, neurotic disorders, and addiction, especially tobacco.
Takakazu Oka (MD, PhD) is Professor and Director of the Department of Psychosomatic Medicine, International University of Health and Welfare, School of Medicine, Japan. His research includes basic and clinical research on the mechanisms and treatment of stress-related psychosomatic disorders, including psychogenic fever. His recent research also focuses on the development of assessment tools to assess shitsu-taikan-sho (alexisomia), the evaluation of the clinical significance of shitsu-taikan-sho, and the treatment of shitsu-taikan-sho.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.