
Abstract
Background:
This study investigated the use of ultrasound-guided extracorporeal shock wave lithotripsy (ESWL) to break stones in the genitourinary tract and prevent genitourinary injury. Our goals were to achieve accurate focusing and minimal X-ray exposure for the benefit of the patients.
Methods:
The LiteMed LM-9200 lithotripter with ultrasonography and fluoroscopy was used for two different procedures: autoaimed and autoperiodical. These procedures enabled dual focusing on stone localization and tracking.
Results:
Out of 108 patients who underwent autoperiodical procedures, 29 had no gross hematuria. Among the 335 patients who received autoaimed procedures, 194 had no gross hematuria. The average duration of X-ray exposure during autoperiodical and autoaimed procedures was 120 and 50 s, respectively.
Conclusion:
The ultrasound-guided ESWL with minimal X-ray exposure was found to be useful in treating genitourinary upper-tract urolithiasis in the autoaimed procedure. Patients who underwent the autoaimed procedure experienced less gross hematuria compared to those who underwent the autoperiodical procedure.
Introduction
With funding from the German Ministry of Defense, Dornier began a study of the effects of shock waves on tissue in 1969. The Dornier lithotripter progressed through various prototypes, ultimately culminating in clinical experience with the first shock wave lithotripsy (SWL) treatment of a human in 1980. The production and distribution of the Dornier HM3 lithotripter began in late 1983, and SWL was approved by the US Food and Drug Administration in 1984. 1 Dornier was the first company to develop a machine to treat urolithiasis. It has been proven to be a safe and efficient way of treating non-infected urolithiasis. The safety of minimally invasive treatment for any disease is crucial, regardless of the device or medication used. In terms of patient care, the impact of minimally invasive procedures—the gold standard—is far-reaching. Extracorporeal shock wave lithotripsy (ESWL) is a non-invasive procedure performed to fragment stones in parts of the genitourinary system, excluding stones in the renal parenchyma and bladder. ESWL has also been used to treat gall bladder and pancreatic stones, but the effects remain unclear. 2 Although soft tissue injury has been launched for the treatment of chronic prostatitis and chronic pain syndrome, the long-term results are unknown. 3
The research and development of our ESWL machine is done in Taiwan. Litemed was initially studied at the National Cheng Kung University.4,5 The LiteMed LM-9200 ELMA lithotripter with ultrasonography and fluoroscopy was used for the dual focusing of stone localization and tracking. With the newly developed computer software, the important feature of the real-time tracking system is the real-time analysis of ultrasound images. Generally speaking, all ESWL machines with the autoperiodical procedure utilize fluoroscopy to track the stone. In recent years, medical treatment for urolithiasis has been used.6,7 However, the expulsion of ureteral stones that are nearly 1.0 cm in size remains equivocal when medical expulsive therapy with an alpha-blocker is used.8–10 ESWL remains the mainstay in stone management with the fitted size. The primary goal of the treatment is to achieve not only a stone-free status but also strive to reduce any factors that would be hazardous to the patient and any resulting sequelae. Many case studies have reported various side effects requiring urgent surgical and nonsurgical intervention, including acute renal failure due to obstruction, sepsis, hematoma of the spleen, liver, and kidney, cardiac arrhythmia,
Methods
General requirements
This study retrospectively reviewed the medical records of patients with radiopaque or radiolucent stones in different parts of the genitourinary tract other than the bladder and parenchyma between September 2020 and December 2022 in the Department of Urology, Shuang Ho Hospital. The stones measured between 0.5 and 2.5 cm, with an average size of 1.0 cm. The Taiwan Medical Insurance Policy covers shockwave lithotripsy treatment limited to these stone sizes. The patients signed an informed consent form for the treatment procedure. All the patients were treated with the same machine, which could undergo both autoaimed and autoperiodical procedures. This lithotripter contained electromagnetic shockwave source, dual localization (ultrasound and C-arm fluoroscopy), and ultrasound real-time tracking system.
Demographic data and treatment indications
This retrospective study included 443 patients (mean age: 60.51 ± 14.35 years), of whom 283 were men and 160 were women. No statistically significant differences in demographics were observed between the two groups. We prospectively enrolled these patients in a continuous cohort study. A total of 132 patients had right renal stones (RRSs), 60 had right ureteral stones (RUSs), 203 had left renal stones (LRSs), and 48 had left ureteral stones (LUSs). This study excluded patients with congenital anomalies, surgical urinary diversion, pediatric cases, coagulopathy patients, and pregnant patients. The stone burden and locations were thoroughly assessed to ensure an acceptable outcome. Various factors such as size, location, stone composition, anatomy of the genitourinary tract, surgeon judgment, handy equipment, patient preferences, and duration of symptoms, which might affect the outcomes, were considered.
Definitions
The autoaimed procedure is a technique that mainly utilizes the ultrasound-based real-time system to track the stone. The autoperiodical procedure is a technique that mainly utilizes fluoroscopy to target the stone. Initially targeting the stone, dual focusing was performed by alternately using fluoroscopy and ultrasonography.
Procedure
Plain abdominal radiography of the kidney, ureter, and bladder (KUB) imaging; intravenous pyelogram imaging; computed tomography (CT); and renal ultrasonography were used to evaluate the stone. Patients with radiolucent stones were excluded as plain x-rays were used as the standard follow-up procedure. All patients were required to be nil by mouth for at least 4 hours before treatment. Complete blood count, blood chemistry, and coagulation profiles were also investigated. The patients were required to stop taking anticoagulants 1 week before the treatment. Physiological signals such as vital signs and real-time electrocardiogram were monitored during the treatment. The patients were in a supine position with no anesthesia or analgesia. Cushions with lubricating jelly were used to touch the patient. Dual ultrasound and fluoroscopy were initially used for stone localization. The machine has an autofiring system; the shock waves are only fired when the stone is in the focal zone in the autoaimed procedure. During ESWL, the initial energy level was 16.5 kV and gradually increased to 19.0 kV if the stones fragmented adequately at low-energy settings, with a fixed rate of 90 shock waves per minute. The average number of shock waves delivered per session was 3650.5 (range: 3500–5000). Treatment was halted when the observed stone fragmentation targeted by both the ultrasonography and/or fluoroscopy image was reached. Two options were used to track the stones: the autoperiodical option, in which the stone cannot be tracked through ultrasound, hence fluoroscopy was utilized to track the stone, and the autoaimed option, in which all the stones can be focused on through sonography, was used to target the stone. The average treatment time, including the initial localization in the autoaimed and periodical procedures, was 39.7 min (range: 30–45 min) and 39.0 min (range: 30–50 min), respectively. All patients were treated in an outpatient facility and prescribed nonsteroidal anti-inflammatory drugs or acetaminophen and antibiotics empirically.
Data regarding stone size and location, blood pressure, urinary tract infection, and perirenal hematoma diagnosed by ultrasound were collected after treatment. All patients were followed up at the outpatient department after 2 weeks, 1 month, and 2 months for the evaluation of the treatment outcomes. Stone fragmentation was defined as observed stone fragments less than 3 mm. On the other hand, the stone-free status was defined as no residual stone seen 2 weeks after treatment in the post-treatment images, namely KUB and ultrasound. The Clavien-Dindo classification system was utilized to classify the complications. 13 Treatment failure was defined as the presence of residual stone fragments bigger than 4 mm after 1 month. Patients with treatment failure were subsequently retreated with auxiliary methods at our hospital or other tertiary hospitals.
Statistical analysis
The significance of age was evaluated using the Student's t-test in Table 1. The t-test's most common application is to test whether the means of two populations are different. The Fisher's exact test was utilized in Tables 1 and 2–4. The odds ratio (OR) is a statistic that quantifies the strength of the association between two procedures: autoaimed and autoperiodical. The statistical significance can be evaluated in terms of visible hematuria, stone-free rate, and dosage of radiation. Statistical significance was defined as a p-value of < 0.05. Numbers and percentages were used to represent categorical data.
Characteristics of the patients.

Mean ± SE.
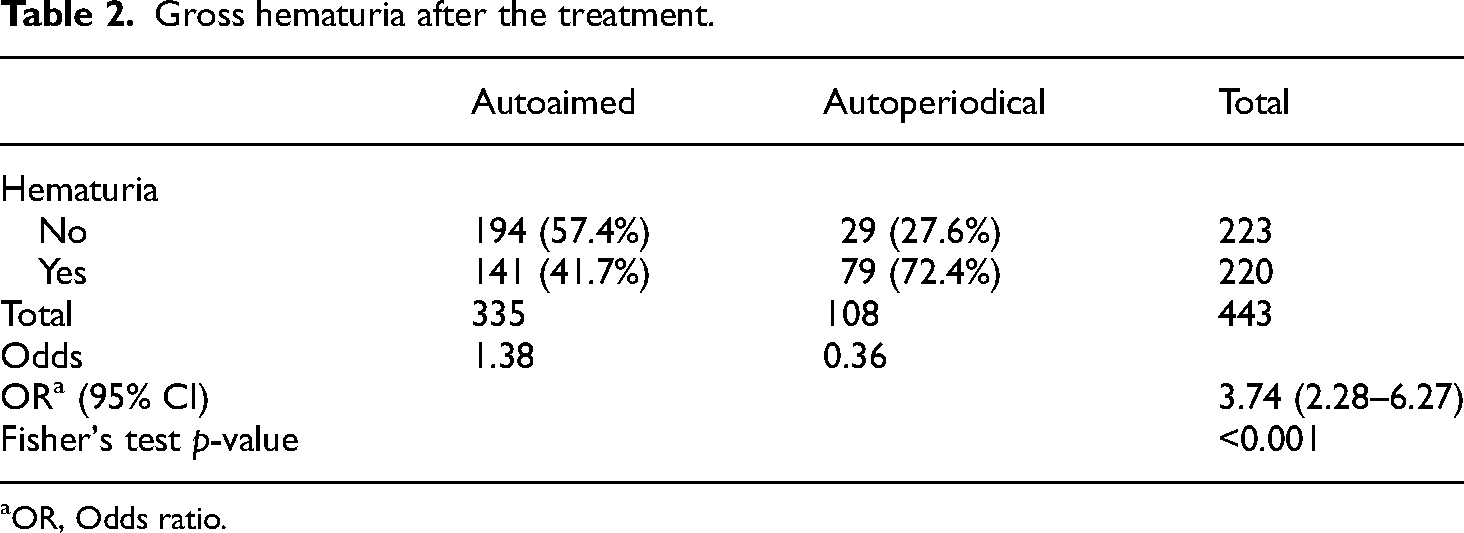
Gross hematuria after the treatment.
OR, Odds ratio.
Results
The patients were reviewed from September 2020 to December 2022. This retrospective study included 443 patients (mean age: 60.51 ± 14.35 years), of whom 283 were men and 160 were women (Table 1). The mean age of the patients who received the autoaimed and autoperiodical procedures was 61.29 ± 13.67 and 58.01 ± 16.18 years, respectively. The age in both procedures showed statistically significant differences (p-value = 0.040). The stone size was found statistically significant (p-value = 0.001) in which the mean of the stone size in the autoaimed and autoperiodical is 0.93 ± 0.35 cm and 0.80 ± 0.29 cm, respectively. A total of 216 (63.9%) male and 122 (36.1%) female patients received the autoaimed treatment. A total of 67 (63.8%) male and 38 (36.2%) female patients underwent the autoperiodical procedure. Gender also did not statistically influence the procedure in which the patients underwent (p-value = 1). A total of 198 patients (58.6%) with LRSs, 3 patients (0.9%) with LUSs, 130 patients (38.5%) with RRSs, and 7 patients (2.1%) with RUSs received the autoaimed procedure. Similarly, 5 patients (4.8%) with LRSs, 45 patients (42.9%) with LUSs, 2 patients (1.9%) with RRSs, and 53 patients (50.5%) with RUSs received the autoperiodical procedure. A significant correlation was observed between stone location and procedure type (p-value < 0.001). The average stone size was 1.0 cm (range: 0.5–2.5 cm). The average energy of the shock wave was 18 kV (range: 16.5–20.5 kV). The average treatment time of the autoaimed and autoperiodical procedures was 39.7 min (range: 30–45 min) and 39.0 min (range: 30–50 min).
Of the 335 patients receiving the autoaimed procedure, 141 patients (41.7%) had gross hematuria (Table 2), whereas 194 patients (57.4%) had no hematuria. A total of 76 (72.4%) of the 105 patients who received the autoperiodical procedure experienced gross hematuria, whereas 29 patients (27.6%) had no hematuria. Fisher's test revealed that the autoaimed procedure caused less hematuria with statistical significance (p < 0.001) and had an OR of 3.74. In Table 3, compared with the autoperiodical procedure, we found that complete stone expulsion in the autoaimed procedure was statistically insignificant (p = 0.882). However, the autoaimed and autoperiodical procedures had stone-free rates of 83.7% and 81.8%, respectively. These results were similar to previous studies (Table 4).
Stone fragments completely expelled after the treatment.

OR, Odds ratio.
Comparison of different lithotripter Models. 6

Thirty-three patients were lost to follow-up after treatment. The duration of x-ray exposure is presented in Table 5. The average duration of x-ray exposure during the autoperiodical and autoaimed procedures was 105.9 ± 27.5 and 51.4 ± 15.8 s, respectively. The most common exposure duration during the autoaimed procedure was 40–49 s (44.1%), and 120–129 s (74.3%) during the autoperiodical procedure. Nine patients were focused and targeted with ultrasound only in the autoaimed procedure. Compared with the treatment in the autoperiodical procedure, it appeared that there was less x-ray exposure in the autoaimed procedure, which was found to be statistically significant.
The duration of the x-ray exposure in seconds.

The most common complication was flank pain (Clavien-Dindo grade I), which occurred in two (0.5%) patients in the autoaimed group and five patients (4.7%) in the autoperiodical group. However, no patients required admission. In the autoaimed group, two patients developed steinstrasse and required ureteroscopic lithotripsy (grade III). In the autoperiodical group, two patients developed post-ESWL ureteral steinstrasse and both required endoscopic intervention (grade III). Two patients in the autoaimed group and one patient in the autoperiodical group suffered from urinary tract infections and required admission for intravenous antibiotics (grade II).
Discussion
Minimally invasive procedures, including extracorporeal shock wave lithotripsy (ESWL), rigid and flexible ureteroscopic lithotripsy, and percutaneous nephrolithotripsy, have emerged as the gold standard for the treatment of urolithiasis. Stone size is a critical factor to consider when opting for ESWL treatment. 14 Medical expulsive therapy has also been employed as an alternative for treating ureteral stones smaller than 5 mm. 15 ESWL has been a widely used technique for urolithiasis since the 1980s.16,17 One of the key advantages of ESWL is its non-invasive nature, eliminating the need for anesthesia. However, there are certain limitations and considerations associated with ESWL, such as contraindications for bladder stones according to national insurance schemes, as well as factors like obesity, steep and narrow infundibulum, lower pole calyx stones, and shock wave-resistant stones. 18 Importantly, ESWL, despite its ability to fragment renal stones, can potentially harm the renal parenchyma. 18
Our study revealed a statistically significant difference in the occurrence of non-hematuria between the autoaimed and autoperiodical procedures, with an OR of 3.74. The autoaimed procedure employed ultrasound for precise localization of stones, enabling the delivery of pulse energy exclusively to the targeted stones and reducing the risk of directing shock waves to the renal parenchyma. Patients taking blood-thinning medications or those with a genetic bleeding tendency should be excluded from ESWL treatment.19,20 Preventing hematuria necessitates accurate stone localization, adjustment of pulse energy, and consideration of changes in stone fragmentation. 21 These findings align with studies emphasizing the crucial role of accurate stone localization in preventing genitourinary injury.
On the other hand, the autoperiodical procedure utilized fluoroscopy for stone targeting. A meta-analysis has shown that a shock wave rate of 60 shocks per minute yields more favorable outcomes compared to a rate of 120 shocks per minute. 22 It is important to apply effective pressure from shock waves specifically to the stones, minimizing the impact on surrounding tissues. 23 Lowering the initial energy and shock wave frequency results in a reduced total number of shock waves and energy delivered, thereby decreasing the potential damage to the kidney, minimizing side effects, and improving patient outcomes.
Ultrasound serves as a suitable imaging modality for detecting urolithiasis. Low-frequency ultrasound applications (3–6 MHz) are used for abdominal and transabdominal studies, while high-frequency applications (7–14 MHz) are suitable for superficial structures like the breast and testis. Ultrasound can detect calculi as small as 0.5 mm, appearing as echogenic foci with shadowing within the urinary tract. Color Doppler can be employed to reveal twinkle artifacts, confirming the presence of renal calculi. 24 However, ultrasound has certain limitations, including its efficacy being influenced by factors such as obesity, stone size, location, density, operator dependence, and interference from bone and air, which may hinder imaging of deep structures or structures obscured by bowel gas.25,26 The primary advantage of ultrasound lies in its real-time tracking capability for breakable stones, minimizing radiation exposure during ESWL treatment. Optimization of patient radiation exposure is essential for ensuring their safety.27–29
In terms of x-ray radiation exposure, our study identified a statistically significant difference favoring the autoaimed procedure compared to the autoperiodical procedure. Adequate training in radiation interventional procedures and techniques is crucial. Real-time ultrasound and post-treatment ex vivo MRI can be employed to detect burst wave lithotripsy (BWL)-induced renal injury with high sensitivity and specificity.28,30 To ensure patient safety, it is imperative to consider effective radiation doses and the amount of background radiation.31,32
While our study provides valuable insights, it is essential to exercise caution when interpreting the results due to the number of patients and the use of multiple comparisons. Some limitations need to be addressed for the benefit of the patients. The availability of CT scans, specifically non-contrast CT (NCCT), varied among different hospitals, limiting the evaluation of certain patients. NCCT is considered the most useful tool for assessing urolithiasis. Expanding the patient sample size would enhance the statistical power and validation of the findings. During fluoroscopy or ultrasound, small or invisible stones may be confused with calcification spots, high echo-density kidneys, or other tissue structures. Precise localization of the stone requires the expertise of a skilled and experienced urologist. In cases where stone fragments become smaller and disperse from the original location, fluoroscopy is often necessary to track the remaining largest fragment, which increases the patient's risk of x-ray exposure. Our clinical study required restarting the tracking system one to three times, leading to longer treatment duration and potential patient discomfort such as claustrophobia in the x-ray shielded treatment room. Physical symptoms such as a choking feeling and palpitations can hinder the effective delivery of shock waves to the stone. Treating stones larger than one cm, especially those located in the renal pelvis, and treating stones in the lower calyx with ESWL pose challenges for urologists. Furthermore, our protocol did not include the study of stone components based on stone analysis. Understanding the stone composition is fundamental in comprehending the etiology of lithogenesis associated with ESWL. 33 Collecting more demographic data, such as basal metabolic index and drug interactions related to BWL, would help identify factors influencing stone treatment with ultrasound-guided ESWL and improve prognosis, thereby enhancing the outcomes of ultrasound-guided ESWL. Despite the clinical use of the machine for several years, ongoing research and development in our laboratory aim to further validate the efficacy of the lithotripter.
Conclusions
Minimally invasive procedures are considered the gold standard for the treatment of urolithiasis. While ESWL has been widely used, there is a preference for a low dose of x-ray radiation and reduced genitourinary injury in the treatment of fragile stones using the autoaimed ESWL procedure. The LiteMed LM-9200 lithotripter, equipped with an ultrasound-based real-time tracking system, offers significant benefits for patients with urolithiasis in the upper genitourinary tract.
Footnotes
Acknowledgements
The clinicians sincerely thank the chief scientist, James Su, in the laboratory of the LITEMED INC, the pioneer of the research and development of the ESWL in Taiwan, for his help.
Author contributions
YT Chiang and SM Chen involved in writing the original draft. HM Tsui involved in writing the original draft. KH Tsui contributed to conceptualization and writing the original draft. HH Juang, MH Chiang, CH Liu and SW Hu involved in writing the review and editing. HM Tsui, WT Kao, and KC Chen contributed in data curation and methodology. KY Tzou, CT Lin, CC Wu, and WL Wu involved in conceptualization, supervision, and writing the review and editing.
Consent for publication
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The present clinical study, including research protocols and data collection, was approved by the Institutional Review Board of the Taipei Medical University (TMU-JIRB: N202211053).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the statistical assistance and wish to acknowledge the support of the Maintenance Project of the Centre for Big Data Analytics and Statistics This study was funded by Taipei Medical University, Grant: TMU111-AE1-B03. Hospital for study design and monitor, data analysis and interpretation.
Author biographies
Yi-Te Chiang, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Shao-Ming Chen MB, MSc (Surgery), is a consultant in Urology. He works in Heping Campus, Taipei City Hospital. His area of interest is urolithiasis and erectile dysfunction.
Hsuan-Mao Tsui, MD, is in resident training in Urology.
Horng-Heng Juang, PhD, is a professor of anatomy. His area of research is biomarker and endocrinology.
Chia-Wei Lin, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Meng-Han Chiang is a fellow in Chang Gung Memorial Hospital. His interest area of research is biostatistics and biomarker.
Chia-Hung Liu, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Su-Wei Hu, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Wei-Tang Kao, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Kuan-Chou Chen, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Kai-Yi Tzou, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Chia-Chang Wu, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Wen-Ling Wu, MD, is a consultant in Urology. He specializes in prostate and urolithiasis.
Ke-Hung Tsui, MD, consultant, professor in the urology, His research is in prostate, urolithiasis, biomarker and tranlation medicine.