
Abstract
Bacterial meningitis after percutaneous radiofrequency trigeminal ganglion is a rare but severe complication. In this article, we report a case of meningitis due to Streptococcus parasanguinis and review the related literature. A 62-year-old male patient with uremia and severe trigeminal neuralgia presented to another hospital and was offered to undergo radiofrequency treatment for a trigeminal ganglion lesion (2022.08.05). The next day (2022.08.06), he presented with a headache and right shoulder and back pain. The pain continued to worsen, so he came to our hospital (The First Affiliated Hospital of Wannan Medical College) and received a diagnosis of bacterial meningitis, which was confirmed by a lumbar puncture. The patient was treated with appropriate antibiotics, and subsequently recovered before being discharged. Although this complication is relatively rare, its progression is rapid. Meningitis must be suspected when a patient presents with headache, fever, and other symptoms associated with meningitis within days after undergoing radiofrequency treatment for a trigeminal ganglion lesion, especially if the patient has an underlying disease that causes a decline in immunity. We discuss this case in terms of clinical presentation, time of onset, treatment, prognosis, past history, and sex. Although early detection of this complication is beneficial, it is better to effectively prevent its occurrence.
Introduction
Trigeminal neuralgia is characterized by stimulus-evoked, intermittent unilateral shock-like pain in one or more branches of the trigeminal nerve. 1 The most common cause of trigeminal neuralgia is neurovascular compression syndrome; however, other etiologies, such as multiple sclerosis, tumors, or vascular abnormalities, may also play a role. The overall incidence of trigeminal neuralgia is estimated to be in the range of 4–20/100,000, and the prevalence is higher in women than in men. The most frequently affected branch is the mandibular division, and pain attacks can occur spontaneously or be triggered by otherwise innocuous stimuli in the area. 2
First-line treatment is a prophylactic medication with sodium channel blockers, either carbamazepine or oxcarbazepine, and second-line treatments are neurosurgical intervention with glycerol blockade or mechanical intervention by balloon compression or percutaneous radiofrequency.1,3 In radiofrequency ablation of the trigeminal nerve, the electrode needle is passed through the facial muscle and the foramen ovale to ultimately reach the semilunar ganglion. When electricity is applied, the electrode is gradually heated, and the semilunar ganglion of the trigeminal nerve is thermally damaged.4,5 As a result, the treatment increases the risk of either skin or intraoral bacteria being introduced into the brain. 6 Bacterial meningitis occurs when bacteria enter the central nervous system. Bacterial meningitis is a highly fatal infection characterized by a triad of clinical signs: symptoms of infection, meningeal irritation signs and symptoms of increased intracranial pressure. Streptococcus is a common cause of pneumonia and meningitis. Streptococcus parasanguinis, a mitis group streptococcus, gram-positive, nonsporulating facultative anaerobe. Streptococcus parasanguinis is a common human commensal bacterial species. It is a prevalent bacterium in the oral cavity and an opportunistic pathogen for infective endocarditis and infection of the heart valves and endocardium.7–9
It increases the risk of bacterial infection when a patient's immunity decreases. patients with uremia can result in retention of uremic toxins and defective renal metabolic activities, which contribute to the increased risk of infections by directly or indirectly affecting the functions of immune cells.10,11
Case report
A 62-year-old male with uremia presented with 1 day of progressive headache, and right shoulder and back pain. The patient then developed fever, dizziness, and vomiting. He had no previous history of headaches. Twenty days ago (2022.07.16), the patient developed pain in the right jaw. He was treated with medications (carbamazepine, phenytoin, or gabapentin) according to the doctor's advice. However, he had no response to pharmacological treatment with those medications. One day prior (2022.08.05), he underwent radiofrequency treatment for a trigeminal ganglion lesion. Then, the patient came to our hospital (The First Affiliated Hospital of Wannan Medical College). On admission (2022.08.06), neurological examination revealed neck stiffness, Kernig sign (+), and Brudzinski sign (−). Blood tests showed elevated white blood cells (14.0 × 109/L), elevated C-reactive protein (138.45 mg/L), and elevated procalcitonin (1.890 ng/mL). A CT scan of the brain showed a small lacunar cerebral infarction. Based on the patient's symptoms and examination results, meningitis was considered. Intravenous cefoxitin sodium (2 g q8 h) and ganciclovir were commenced. We performed a lumbar puncture immediately. CSF analysis showed elevated white blood cells (1800 × 106/L), elevated protein (180.8 mg/dL), and decreased glucose (2.11 mmol/L). Medications were immediately switching to intravenous ceftriaxone (3000 mg once daily) according to the CSF results. The first cranial magnetic resonance imaging (MRI) (scan + contrast-enhanced) was performed on Day 4 and showed edema in the right temporal lobe, patchy shadows in the trigone of bilateral lateral ventricles, and no enhancement, so inflammatory lesions were considered (Figure 1). On Day 6, the bacterial culture of the cerebrospinal fluid showed Streptococcus parasanguinis. Therefore, the diagnosis of bacterial meningitis was confirmed. One week after treatment with antibiotics, the patient's body temperature returned to normal, and a routine blood examination showed a normal white blood cell level (4.9 × 109/L). Then, we reduced the dose of ceftriaxone (2000 mg once daily). The patient was treated with a 1-day course of cefoxitin sodium and 12 days of ceftriaxone; after showing no special discomfort, he was discharged home on Day 16. The patient's symptoms of trigeminal neuralgia were relieved.
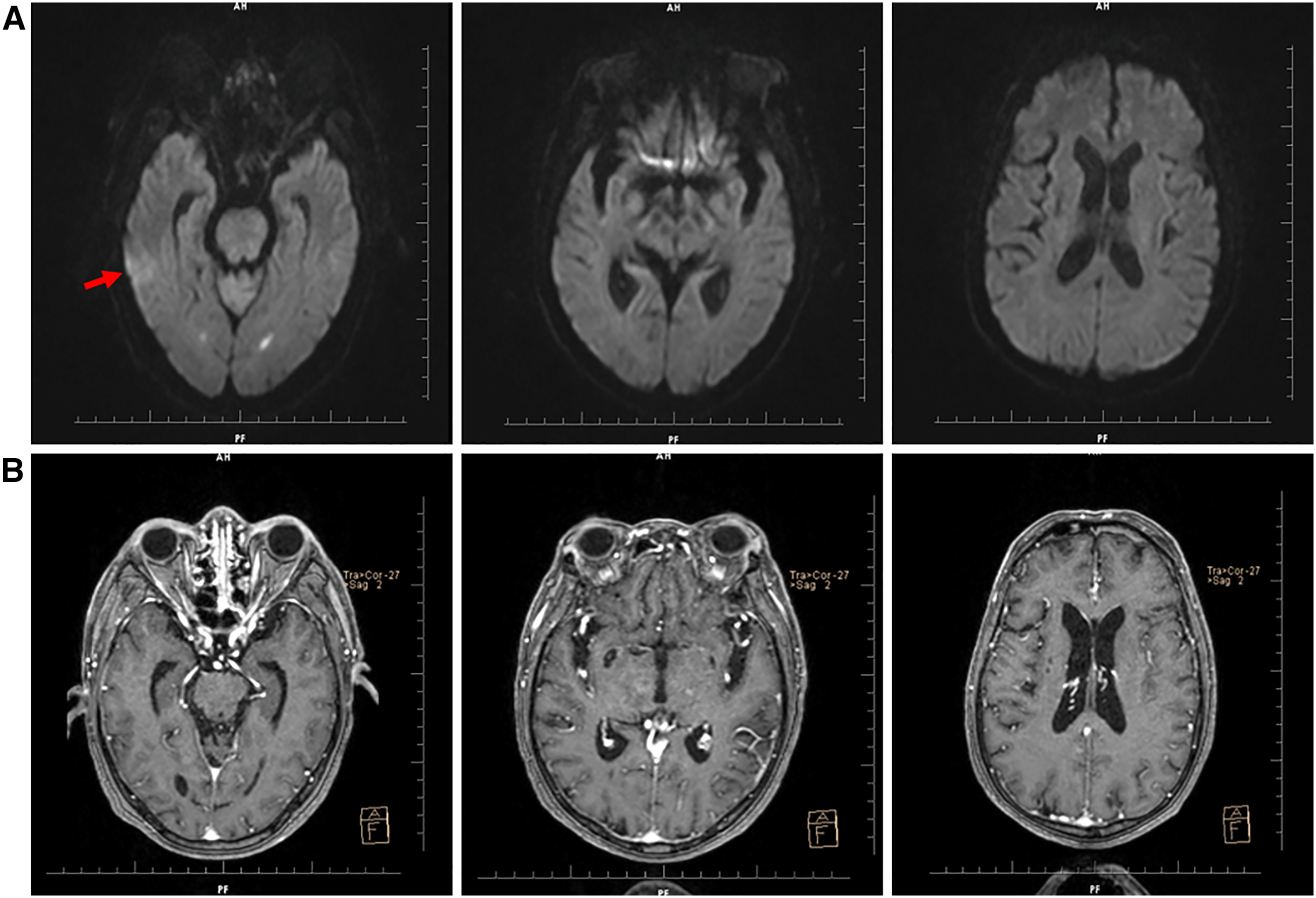
A 62-year-old uremic male with meningitis. (A) Magnetic resonance imaging (MRI) scan shows edema (red arrow) in the right temporal lobe, patchy shadows in the trigone of bilateral lateral ventricles and (B) contrast-enhanced MRI images show no enhancement.
Discussion
In general, the occurrence of bacterial meningitis after percutaneous radiofrequency treatment for a trigeminal ganglion lesion is very rare. By assessing all the published data on meningitis, we found that its overall mean incidence is 0.15%. 3 By searching the literature in PubMed, we found that 27 cases of meningitis had been reported after an invasive procedure. The characteristics of the case reports are presented in Table 1. We will discuss these cases in terms of clinical presentation, time of onset, treatment, prognosis, past history, and sex. Although early detection of this complication is beneficial, it is better to effectively prevent the occurrence of this complication.
Case reports of bacterial meningitis after invasive treatment of the trigeminal neuralgia.

Silverberg 1978, 12 Mitchell 1985, 13 Sweet 1986, 14 Torroba 1987, 15 Young 1988, 16 James 1995, 17 Enting 1997, 18 Blomstedt 2002, 19 Hirooki 2002, 20 Pickett 2005, 21 Ward 2007, 3 Koning 2012, 6 and von Kietzell et al. 2015. 22
HBP: high blood pressure; MS: multiple sclerosis.
According to Table 1, the first symptoms of 28 patients were fever and headache. It is not difficult to see that the onset of this complication is serious; in most patients, the onset of this complication is within 3 days after the operation, and individual symptoms appear after a week. Acute onset, headache, and fever are consistent with the clinical manifestations of meningitis. Despite an acute onset and severe symptoms, the prognosis was not poor after treatment with antibiotics. This prognosis indicates that the complication has a good response to antibiotic treatment after the occurrence of symptoms. When patients have similar symptoms, doctors need to distinguish the symptoms from those of other diseases. Once the diagnosis of meningitis was established and therapy was started, the patient recovered without any damage. 6 Considering the characteristic clinical manifestations of meningitis, (1) infectious symptoms (fever or upper respiratory tract infection), (2) meningeal irritation sign (stiff neck, positive Kernig, and Brudzinski signs), and (3) increased intracranial pressure, patients should undergo routine blood, cerebrospinal fluid, and imaging examinations in a timely manner.
The causative organism was identified in 64% of the cases, and in these confirmed cases, streptococci accounted for 78% of the total infections (Figure 2). These pathogenic organisms include Streptococcus mutans, Streptococcus salivary, Streptococcus viridis, and Streptococcus pneumoniae. Streptococci are found in almost every part of the human body, mainly in the mouth and upper respiratory tract. Streptococcus bacteria are acquired after birth and therefore play an important role in the functioning of the oral microbiome. 23 We found that percutaneous radiofrequency treatment for a trigeminal ganglion lesion led to more complications attributable to puncturing. One of the most important steps of this approach is tracking the needle at the entrance to the foramen ovale. The ideal penetration zone of the foramen ovale is located at the posteromedial border of the foramen. Entrance to the foramen ovale warrants extreme caution, and even a small displacement of the cannula in either depth or direction can lead to more complications.24,25 In this process, the mouth, and skin may be punctured, and bacteria from the skin and mouth may be introduced into the foramen ovale. These bacteria cause associated complications. This evidence indicates that the most likely cause is contamination from the oral microbiome. In the treatment of trigeminal nerve invasion, attention should be given to avoid damage to the oral mucosa, especially when the needle is inserted and removed from the foramen ovale.3,17 Although this complication is rare, we should be aware that meningitis is a potential complication of the procedure when patients develop related symptoms after surgery, and physicians need to have a high level of suspicion for this potential complication.

The classification of organisms reported to cause bacterial meningitis after invasive treatment of the trigeminal neuralgia.
A literature search revealed no reports in which prophylactic use of antibiotics was recommended after treatment for trigeminal nerve invasion. Twenty-eight patients had symptoms of meningitis, such as headache and fever, after treatment for trigeminal nerve invasion and were over 50 years old. This group of people has decreased immunity, making them prone to other diseases despite prophylactic antibiotic use.
In conclusion, meningitis should be considered when patients develop headaches and fever after treatment for trigeminal nerve invasion. In addition, patients should be warned about the risk of complications after surgery. Once the symptoms of headache and fever appear, a doctor should be seen in time. Do not mistake it for a cold and delay visiting a doctor. Special attention should be given to elderly patients and patients with underlying diseases who have a compromised immune system.
Footnotes
Author's note
The authors obtained informed consent from the patient for publication of the case report and related images and signed a written informed consent form.
Authors’ contributions
Jianfei Wang: Conceptualization, Methodology, Writing Original Draft. Wenjie Hu: Writing Review, Editing. Ruirui Zhang, Fanfu Jin: Formal analysis, Validation. Jia Hu, Qingqing Bai, Qi Wang: Data Curation, Resources. Shoucai Zhao: Supervision. Zhaohu Chu: Funding acquisition. Yang Xu: Project administration. All authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (82171329, 81701161); the Open Project of Key Laboratory of Non-coding RNA Transformation Research of Anhui Higher Education Institution (Wannan Medical College) (RNA202201); Education Department of Anhui Province, China (KJ2021ZD0096); Wannan Medical College, Anhui, China (YR201802, KGF2019G02, WK2022ZF16, WK2022F23, and WK2022F07). We thank X-Lab group for designing this research.
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Wannan Medical College (2021-18).
Author biographies
Jianfei Wang is an MM in neurology. His area of research is Cerebrovascular disease.
Wenjie Hu is an MD in neurology. His area of research is Cerebrovascular disease.
Ruirui Zhang is an MM in neurology. Her area of research is Cerebrovascular disease.
Fanfu Jin is an MM in neurology. His area of research is Cerebrovascular disease.
Jia Hu is an MD in neurology. Her area of research is Cerebrovascular disease.
Qingqing Bai is an MM in neurology. Her area of research is Cerebrovascular disease.
Qi Wang is an MM in neurology. His area of research is Cerebrovascular disease.
Shoucai Zhao is a professor in neurology. His area of research is Cerebrovascular disease.
Zhaohu Chu is a professor in neurology. His area of research is Cerebrovascular disease.
Yang Xu is a PhD in neurology. His area of research is Cerebrovascular disease.