
Abstract
The COVID-19 pandemic has come to stay, at least for a while. The initial bewilderment and restrictive measures have given way to the population's mental decay and increased stress on workers facing work and family demands in a difficult-to-manage situation. For this reason, this descriptive cross-sectional study sought to analyze stress levels in a sample of 263 general and healthcare workers (from 24 to 67 years of age) and their relationship with negative work-home interaction (WHI) and with gender in the second wave of contagions and deaths caused by the COVID-19 pandemic in Spain (October-December 2020). The results showed that having a higher level of WHI, the presence of work overload, health concerns, economic concerns, and lower-income were predictors of stress among these workers. Age and health-related occupations were contributing factors to work overload and health-related concerns. In addition, the relationship between being a woman and suffering from higher stress levels was mediated by income level, economic concern, and the WHI. Other variables such as having children or dependents, marital status, concern for the health of others, and teleworking were not associated with the stress levels detected in the sample. This research pays attention to the health state of workers beyond the initial stage of the pandemic, where most studies on this issue have concentrated. Thus, this study provides evidence of the uneven impact this crisis has on women and men, contributing to clarifying the relationship between gender, the WHI, and stress.
Introduction
On 25 October 2020, the Spanish Government declared a new State of Alarm in the light of increased contagions and deaths resulting from Coronavirus SARS-CoV-2, and due to the consequent hospital pressure that the country was suffering. In this way, Spain and most European countries began to face the so-called second wave of the pandemic. 1 This State of Alarm was again declared on 9 November 2020 and, in the previous days, it was extended for the next six months. Among other measures, freedom of movement through public roads or spaces at specific times of the day was limited, as well as the entry and exit of the territory of each autonomous city or community, and gatherings in public and private spaces to a maximum of six, except for domestic partners. 2 The second wave of the pandemic spread in the country from mid-October to December 2020, with the highest peak of daily contagion recorded on 2 November (55,019) and of deaths on 4 November (1623). 3
The pandemic has undoubtedly affected the labour and economic market, due to the closure of businesses, job adaptations, or telework, in a more negative and pronounced way in Southern European countries such as Spain and Italy, as compared to other European powers. This is because the southern countries present a greater proportion of jobs in sectors such as hospitality, leisure, and personal services, as well as having higher rates of precarious employment and lower tradition of the teleworking modality. 4 This situation not only results in losses but also in new demands for workers who must carry out their work in compliance with strict health measures that in many cases lead to an overload of responsibilities and increased stress levels.5,6 More importantly, the impact of the pandemic on the labour and financial market translates unequally between men and women, affecting most of the greatest feminized sectors, including formal and informal care work.6–8 The existing gender pay gap that is widely observed in all countries9,10 and particularly in Spain, being more pronounced in health and social services activities, 11 has increased with the situation generated by COVID-19. 12 Therefore, following Smith, 13 it is necessary to include the gender perspective as a priority in studies that cover the psychological, work, and family impact of the COVID-19 pandemic.
National14–16 and international research17–19 have highlighted the effects of the pandemic on the mental health of the population during the first wave of contagions. In this sense, psychological stress, understood as the individual's perception of an over-demand from the environment that tests their adaptive capabilities 20 has been studied since the beginning of this crisis given the distress it causes and its contribution to the development and/or intensification of physical and mental illnesses such as anxiety, depression, post-traumatic stress disorder, cardiovascular disease, or cancer.21–23
For example, Park et al. 18 found a significant percentage of Americans with extreme stress levels (10.1%) in early April 2020, a month after the World Health Organization declared the pandemic. 24 In Spain, the data collected on these dates are similar, as shown by the study by Odriozola-González et al., 15 in which they identified a quarter of the sample with stress levels from moderate to severe (25.6%). The figures are higher among healthcare staff, between 41.1% and 68.3%, 25 as was the case in Spanish healthcare workers, of which 46.7% had clinical levels of stress. 26
Heterogeneous results have been shown in workers’ stress levels with respect to the role of certain sociodemographic variables, such as gender. More than that, Gyllensten & Palmer 27 argue that it is not possible to firmly conclude on differences between men and women due to the quality of some of the research in this regard and its capacity for generalization. However, there appears to be a greater consensus that women are more stressed since they are being affected by a multiplicity of roles, lack of career progress, and discrimination and stereotypes. The diversity of positions on gender and stress is also shown in studies conducted during the COVID-19 pandemic in which, on the one hand, higher levels of stress have been observed among women as compared to men both in the general population 28 and in the healthcare working population. 26 However, on the other hand, there are also studies that observed higher levels of stress in men, 29 and others that do not show differences in this regard, in this case, among healthcare workers. 30
Other sociodemographic variables associated with stress during the pandemic have also been explored. Thus, higher levels of stress have been identified among the general Spanish population in those who live without a partner —because they are separated during confinement or because they are single—, childless, underage, and with lower income. 28 However, other studies, also on the general population, have found no relationship between stress and age,18,29 financial resources, 18 marital status,29,31 and parental status, 29 nor has there been an association between stress and marital status among healthcare staff, 30 although it has been found regarding age in this same professional group. 26 As can be seen, most studies on stress involving workers, conducted during the pandemic, have focused on healthcare staff, so there are few fields of study regarding stress and its associated variables among workers belonging to other sectors.
Bridgland et al. 32 warn that the situation generated by COVID-19 is a stressor in itself that could lead to mental pathologies. This effect is also the case with events that have not yet occurred, i.e. a response to future and/or imagined events such as expected contact with the virus, loss of work and/or income, job changes, and changes in children or dependents, and also concern about the duration of the crisis and for close persons getting infected.28,29,32 In other major disasters for the population such as the one caused by Hurricane Katrina in 2005, researchers found that the financial and social support losses experienced by survivors were determinants of post-traumatic stress disorders within two years of the event. 33
One factor that workers have associated with stress is the negative work-home interference (hereinafter referred to as WHI), which refers to a conflict that occurs when pressures from work and family roles are incompatible with each other in some aspect, either due to time pressure, the effect of stress or fatigue on the performance of duties, or task-related opposing behaviours. This results in a mismatch in the work-life balance and, in turn, performance in the work role hinders performance in the family one. 34 WHI has been observed to affect the psychological state of the individual, so a greater WHI is related to increased perception of stress35,36 and general psychological distress. 37
So far, there is little research published to study the WHI during the pandemic. Among the literature, we find the two studies by Vaziri et al. 38 that allow us to assess the changes produced in this field among American workers from various sectors (Information Technology, Mathematics, Sales, Education, Administration, Health, etc.). Their results show that 40% of the sample had a high WHI during the pandemic and that a significant proportion experienced negative transitions from the pre-pandemic stage, i.e. worsening their levels of WHI and positive work-home enrichment. Among other results, the authors found that this was greater in the case of those experiencing increased technological stress or having high work-home segmentation preferences; for these people, their performance and job satisfaction worsened significantly. Other research has also shown a link between stress, WHI, and attitude towards teleworking during the COVID-19 pandemic among Chilean teachers. 39
The differences between men and women regarding the WHI have been addressed by previous literature albeit, again, with diverse results. Thus, in Jacukowicz & Merecz-Kot's study 40 on Polish office workers, no gender differences were found, as in the study by Merecz-Kot & Andysz, 41 conducted in the same country, and that by Kinnunen et al. 37 involving workers from various occupational sectors in Finland. On the other hand, Jansen et al., 42 who studied workers belonging to 45 different companies in the Netherlands, identified a greater number of men than women in the high WHI group. On the other hand, in the work by Van der Lippe & Lippényi 43 on teleworkers from various European countries including Spain, a greater WHI was observed in women versus men. Studies conducted during the pandemic also show disagreement regarding the role of gender in the WHI, with results pointing to higher levels among female teachers 39 and others with high levels among men among public officials. 44 On the other hand, Vaziri et al. 38 found no differences according to gender in the changes produced regarding the WHI, which they attribute to inadequate statistical power. This disparity in results may be due to, in addition to issues specific to research design and the type of studied occupations, the country from which the data are obtained, as the results in the WHI will depend on the existing level of gender equality that pervades the working life and on the standards relating to female employment in the specific context. 45
Research that studies the impact of the early months of the pandemic on the mental health of the population and stress, in particular, has grown exponentially (e.g. Sun et al., 19 Wang et al., 29 ) although now it is necessary to continue to examine the long-term effects of this situation on people's lives and health, especially in both general and healthcare workers. Also, as mentioned above, it is necessary to further study the WHI in the pandemic and its relationship with stress, as well as to prioritize gender analysis for further clarification and understanding.
For this reason, the objective of this study was to analyze the relationship between stress, WHI, and gender during the COVID-19 pandemic (second wave) in a sample of workers residing in Spain. It was hypothesized that the WHI had an interaction with perceived stress at this time of the pandemic (Hypothesis 1), as well as gender (Hypothesis 2), having minors under their control (Hypothesis 3), and being a healthcare worker (Hypothesis 4). Other sociodemographic and labour variables (age, marital status, dependents, work overload, and income) and concern for one's health, concern for the health of others, and economic concerns about WHI and stress will be explored.
Method
Design
This study followed a descriptive cross-sectional survey design.
Participants
A total of 320 people initially accessed this study through an online questionnaire. In applying the inclusion criteria (being at least 18 years old, residing in Spain, currently having a job, and responding to the questionnaire in its entirety), the final sample consisted of 263 people, 76.4% of them women, and aged between 24 and 67 years (M = 44.49; SD = 10.70), 69.6% lived as a couple, 44% had minors, and 9% had other dependents in their charge. In the sample, which was represented by all Spanish regions, it was observed that 60% were active professionals in healthcare services, while the remaining 40% included workers from different labour sectors (trade and public service, education, administration and finance, engineering, public officials, law, ICT, and social and community services).
Instruments
Background factors. Information was recorded on gender (male vs. female), age, province, marital status (with couple vs. no partner —single, separated/ divorced, widowed), coexistence with minor children (yes vs. no), and with dependents (yes vs. no), employment situation (multicategory), income (less than 500 euros; €501 - €1000; €1001 - €1500; €1501 - €2000; €2001 - €2500; €2501 - €3,000, more than €3001), teleworking (yes vs. no), and present work overload perception due to the COVID-19 situation (yes vs. no).
Perceived Stress Scale (PSS-14, 46 ) adapted version of Remor. 47 A self-applied instrument that provides an overall measure of perceived stress in the last month based on an assessment of situations considered to be stressful for the person. It contains 14 items with a 5-point response scale (0 = never - 4 = very often). To calculate the total score, it is necessary to reverse the scores of items 4, 5, 6, 7, 9, 10, and 13, and to add the scores of the 14 items (0–54 points), so that higher scores indicate higher levels of perceived stress. The Spanish version has shown appropriate psychometric properties. 47 In this study, the internal consistency is also very adequate (α = .92).
Work-home interaction (WHI). Subscale of the Survey Work-Home Interaction-Nijmegen (SWING, 48 ) validated in Spanish by Moreno-Jiménez et al. 49 It measures the degree of negative work-home interaction through 8 items with a 4-point response scale (0 = never - 3 = always). The final score is calculated based on the mean score of each item, so higher scores indicate higher WHI. The instrument as a whole showed adequate psychometric properties. 49 In this work, the internal consistency of the WHI subscale was successful (α = .92).
Concerns due to COVID-19. Three items were designed, following the consensus of a panel of experts based on existing evidence, that measured the degree of concern that participants had about their health, the health of others, and their economic situation in the context of the pandemic. These items had a 10-point response scale (1 = not concerned at all – 10 = very concerned).
Procedure
The data in this study come from a sample of people who participated in the initial ImpactCOVID-19 project in April 2020 (first wave), conforming a total of 4180 participants.14,50 In that project, participants who agreed could freely provide their emails to participate in further studies. In this way, the researchers sent an invitation by email to request collaboration in this second study through an online questionnaire designed through the Qualtrics® survey platform. Data collection took place from 11 November to 14 December 2020, in the second wave of contagions in Spain and after the declaration of a new national State of Alarm. Before responding to measurement instruments, participants had to explicitly provide their informed consent after reading the details of the study. Participation was voluntary and confidential, and unpaid. This data collection has respected the laws in force on the protection of personal data. The project was approved by the Research Ethics Committee of Huelva, belonging to the Regional Ministry of Health of Andalusia, Spain (PI 036/20-2).
Data analysis
The SPSS version 26 statistical programme (IBM, Armonk, NY, USA) and the PROCESS macro 51 were used.
First, the relationship between the predictive variables, one by one, and stress and WHI was assessed, applying Student's T-test for independent samples when the factors had two categories (Cohen's d = .20: small; = .50: median; >.80: large) and its non-parametric alternative (Mann-Whitney U test) when the assumption of data normality with groups with less than 30 responses was breached. Pearson's correlation coefficients were also calculated when the predictors were quantitative variables (r = .10: small; = .30: intermediate; = .50: large). Although neither scale that measures the WHI and stress has a cut-off point, it was decided to report the number of participants with levels considered high in both measures. Specifically, greater than or equal to 2 points in the WHI and greater than or equal to 28 points regarding stress levels. In the latter case, the pattern marked by previous works was followed.52,53
Second, hierarchical multiple linear regression analysis was performed to determine stress predictors (R2 = .01: small, = .10: intermediate, >.25: large), including all the variables as simple factors and two-to-two interactions. We centred all the continuous predictive variables. To analyze the interactions, it was necessary to divide the age variable and the concern for one's health variable into two halves based on the median (low vs. high levels). Student's T was used for independent samples to examine differences in mean stress scores based on these observed interactions.
Third, as gender was not a predictive factor of stress in this multi-regression model used, it was analyzed whether its relationship was mediated by the WHI, income, and economic concern. To do this, the macro Process was used to test a predictive mediation model designed according to Hayes indications 54 and guided by the results observed in preliminary analyses and previous literature. Standard errors were generated using heteroscedasticity-consistent covariance matrix estimator HC4, and the number of bootstrap samples to get confidence intervals was 10,000.
Results
In order to individually explore the relationship between variables, stress and WHI levels were assessed in the entire sample and based on background factors (Table 1). On the one hand, 82 participants (31.2%) were identified with considerably high levels of stress. Women had higher stress levels than men (t = 2.60, p = .010, d = 0.38), as did people who reported work overload (t = −2.47, p = .014, d = 0.32). No statistically significant differences in stress scores were found based on marital status, having minor children, having dependents, teleworking, and being healthcare staff (all p > .05). On the other hand, it was determined that 29 people (11%) had high levels of WHI. Women scored significantly higher (t = 2.11, p = .036, d = 0.31) than men. This was also the case of those with minor children (t = −2.66, p = .008, d = 0.33), those who did not telework (t = 2.38, p = .018, d = 0.36), those that reported work overload (t = −4.61, p < .001, d = 0.59), and healthcare staff (t = −3.49, p < .001, d = 0.44). The rest of the variables were not related to stress levels (all p > .05).
Work-Home interaction and stress according to background factors.
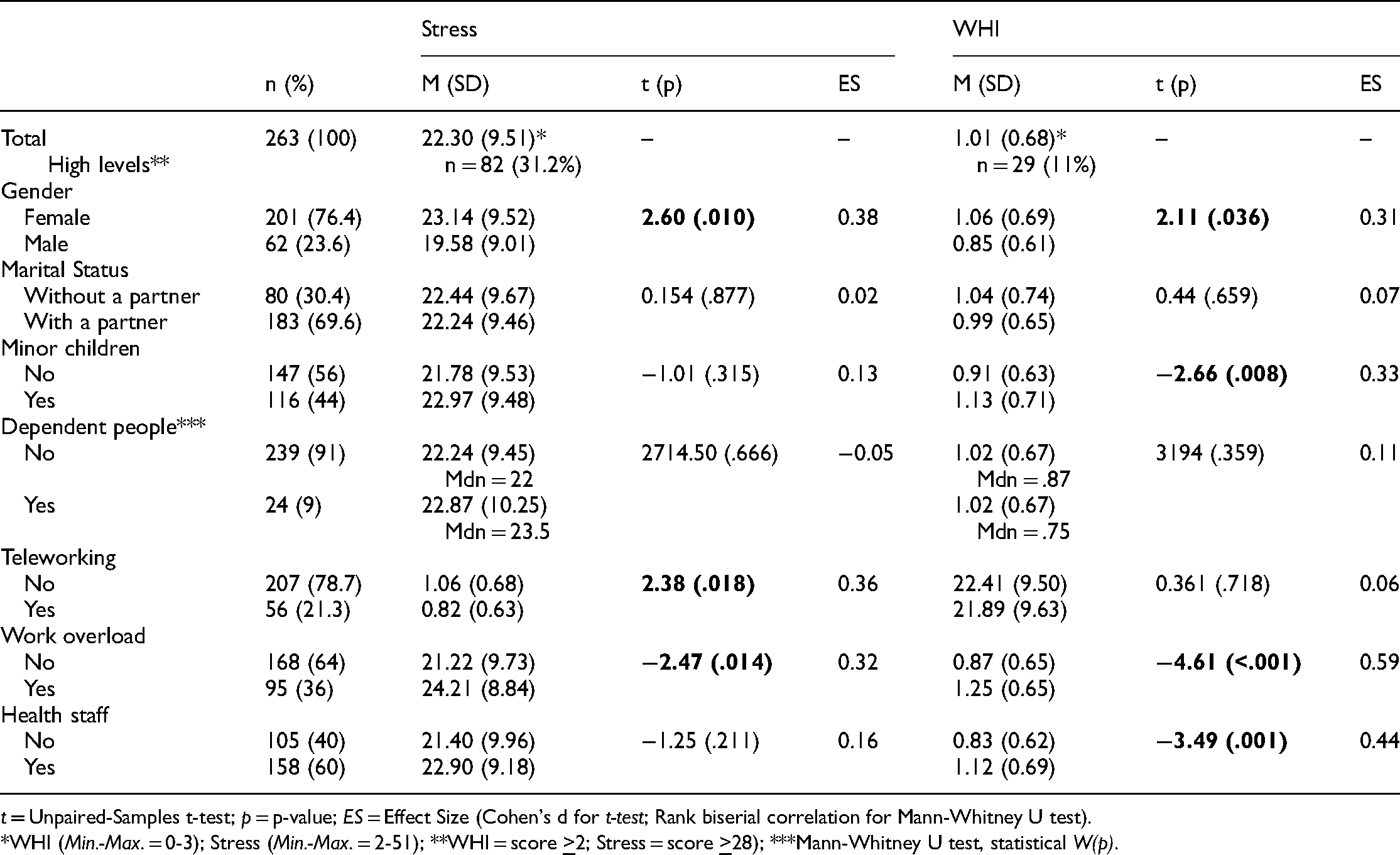
t = Unpaired-Samples t-test; p = p-value; ES = Effect Size (Cohen's d for t-test; Rank biserial correlation for Mann-Whitney U test).
*WHI (Min.-Max. = 0-3); Stress (Min.-Max. = 2-51); **WHI = score
Table 2 shows data on the degree of concern of participants regarding different issues and their relationship to background factors (Table 2). Under no circumstances were statistically significant differences found depending on the level of concern for one's health or the economy (p >.05). Only healthcare staff showed greater concern for other people's health, as compared to general workers. Statistically significant differences in the income variable were observed. Thus, it was higher among men versus women (t = −3.43, p = .001, d = 0.50), in those who reported work overload (t = −2.03, p = .043, d = 0.26), and among healthcare staff (t = −4.65, p < .001, d = 0.62).
Concerns and income according to background factors.
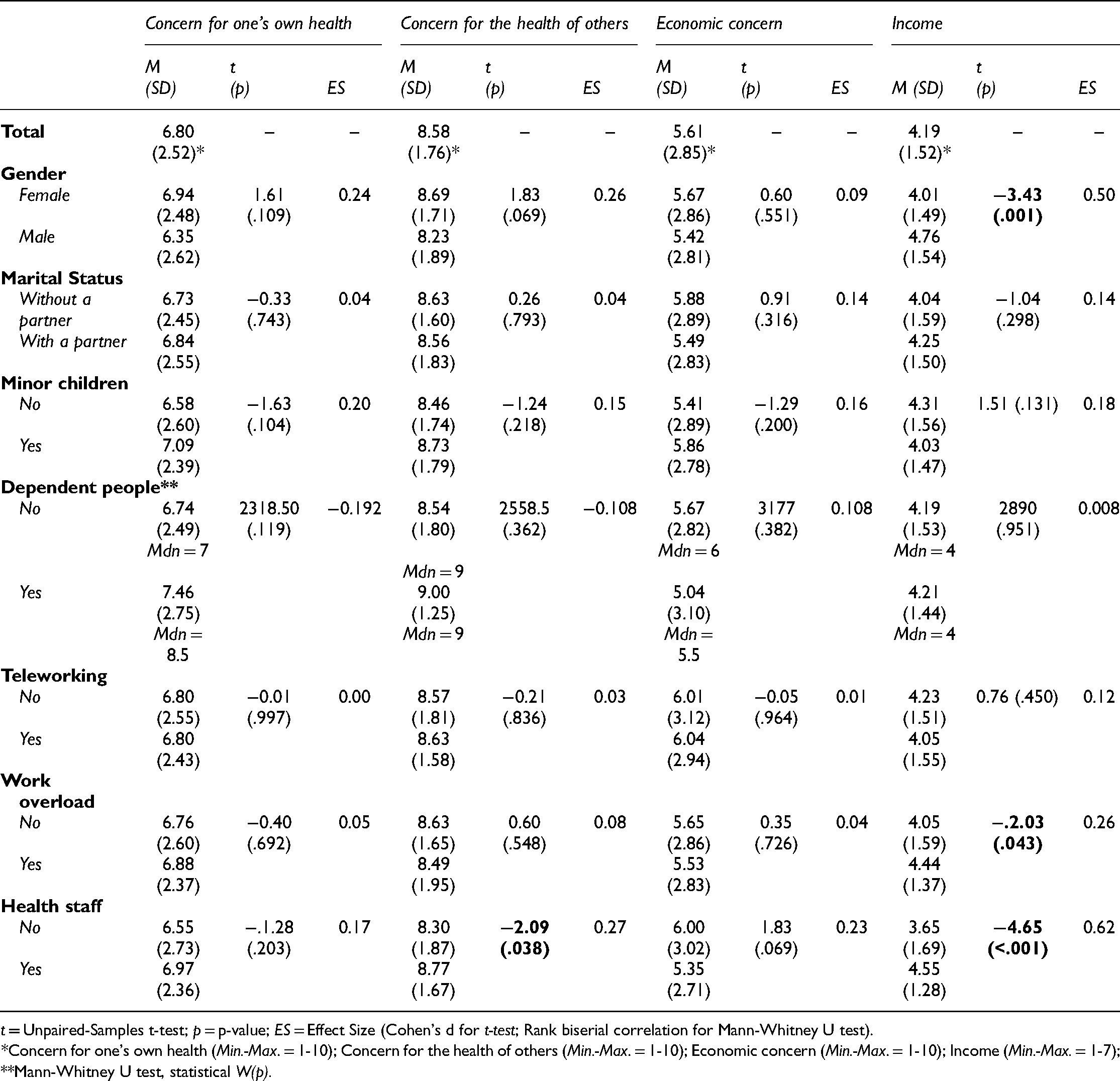
t = Unpaired-Samples t-test; p = p-value; ES = Effect Size (Cohen's d for t-test; Rank biserial correlation for Mann-Whitney U test).
*Concern for one's own health (Min.-Max. = 1-10); Concern for the health of others (Min.-Max. = 1-10); Economic concern (Min.-Max. = 1-10); Income (Min.-Max. = 1-7); **Mann-Whitney U test, statistical W(p).
The relationship between stress, WHI, concern, income, and age (Table 3) was analysed. In this way, stress was positively related to all the variables (r = .25 - .63, p < .01), except for income (r = −.21, p < .01) and age (r = −.18, p < .01), whose associations were negative. WHI was not related to income, but it did react with the rest of the variables in a positive way (r = .25 - .37, p < .01), and negatively with age (r = −.18, p < .01). The three types of concern were positively related to each other (r = .22–.52, p <.01), although only economic concern was related to income (r = .37, p < .05) and age (r = −.13, p < .05) in a negative way. In addition, a positive relationship between age and income (r = .40, p < .05) was observed.
Correlational analysis of continuous variables.

*p < .05; ** p < .01.
To identify stress predictors, hierarchical multiple linear regression was performed including analysis of simple effects and two-to-two interactions. Table 4 shows the factors resulting from applying the model, with 55% of the variance explained (F = 31.24, p < .001). As for the simple effects, the most weighted factor was the WHI (β = .59, t = 12.34, p < .001), followed by income (β = −.16, t = −3.12, p = .002), and economic concern (β = .10, t = 1.99, p = .048). Consequently, higher scores in WHI and in concern for the economy, as well as lower levels of income, would be predictors of higher levels of stress. The simple effects of work overload and self-concern should be interpreted in the light of the interactions that arose, which were: age*own health (β = .14, t = 3.24, p = .001); healthcare staff*own health (β = −.19, t = −3.01, p = −.003), and healthcare staff*work overload (β = −.30, t = −3.32, p = −.001).
Multiple linear regression models.
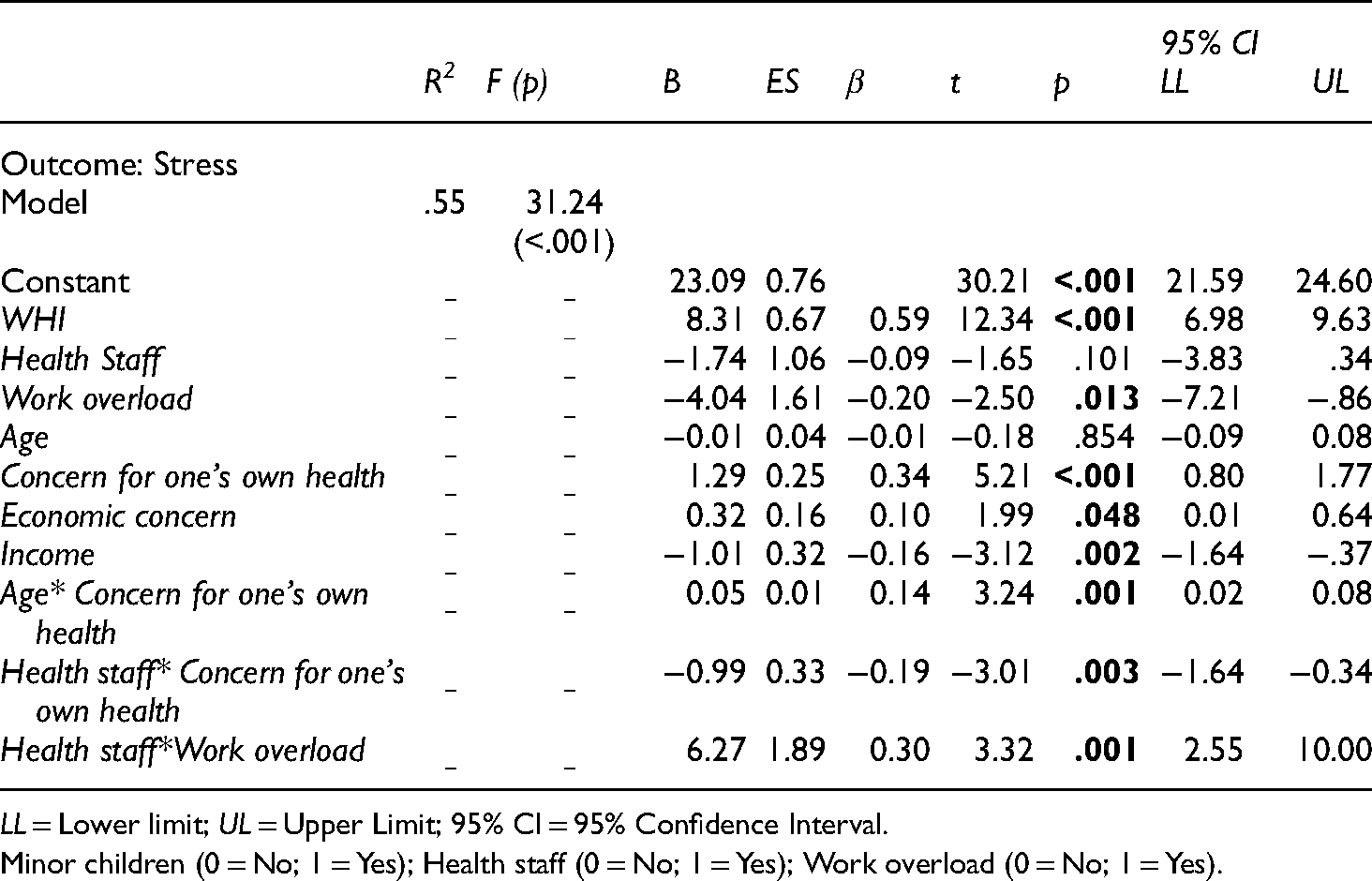
LL = Lower limit; UL = Upper Limit; 95% CI = 95% Confidence Interval.
Minor children (0 = No; 1 = Yes); Health staff (0 = No; 1 = Yes); Work overload (0 = No; 1 = Yes).
First (Figure 1), the level of stress was significantly higher among participants who were more concerned about their health (i.e. scores > 7-Median), as compared to lower levels of concern, both in the younger group (24–44 years, Aa, t = −3.05, p = .003) and in the older age group (45–67 years, Bb, t = −5.61, p < .001). On the other hand, age differences were observed only when health concerns were low, so that stress was higher in the younger group than in the older one (AB, t = 2.86, p = .005). No differences in stress scores were observed based on age when concern for one's health was high (ab, t = 1.23, p = .221). This suggests that age was related to stress only when the level of health concern was low; in this case, higher stress in those of younger age, since when this concern was high, participants of any age showed higher levels of stress.
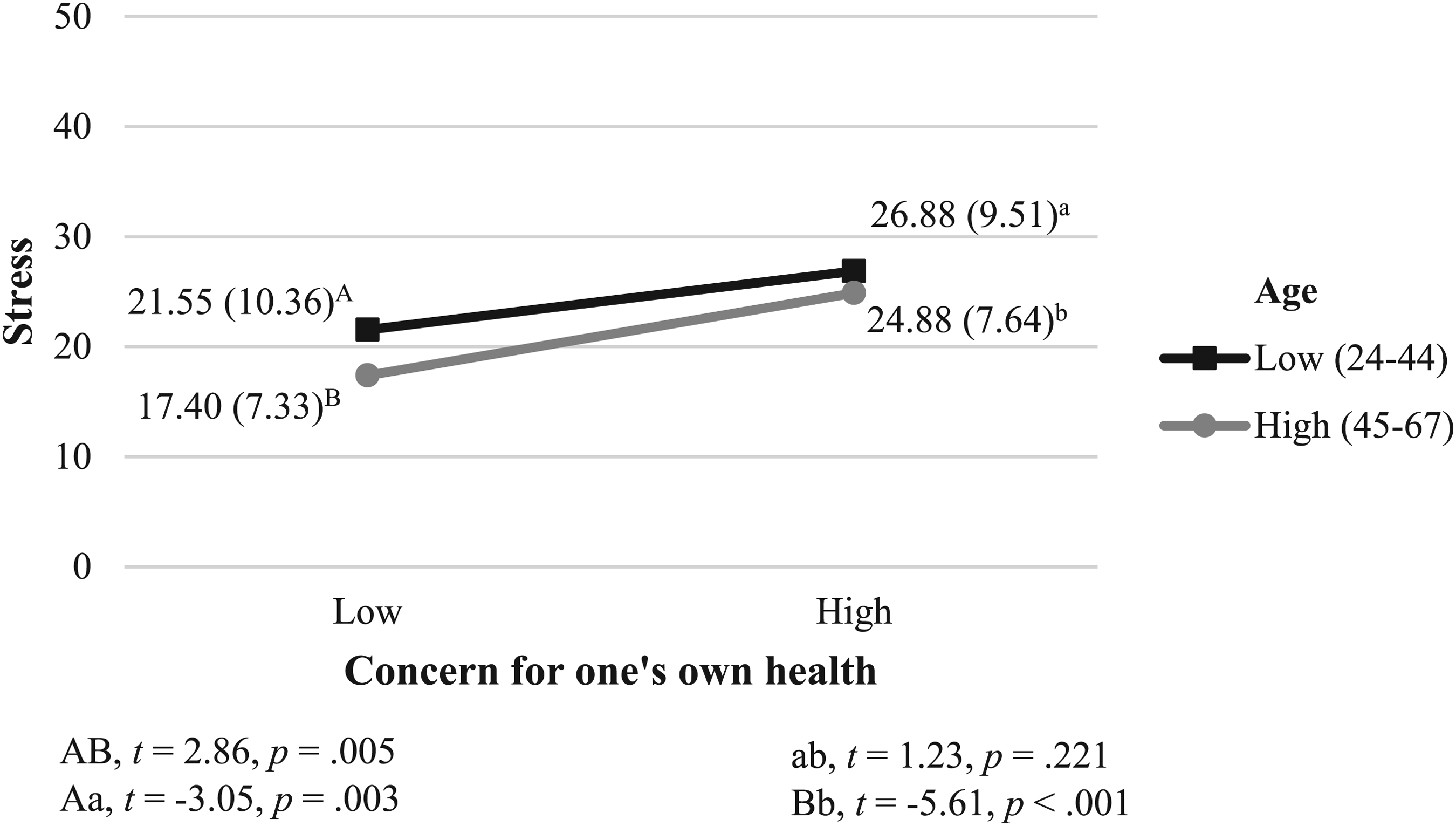
Interaction effect between concern for one's own health and age on stress.
Secondly (Figure 2), as already mentioned, increased concern for one's health, as compared to a lower level of concern, predicted higher levels of stress, both in general workers (Bb, t = −5.52, p < .001) and in healthcare staff (Aa, t = −2.78, p = .006). When the level of concern was low, significant differences were observed depending on the type of work, with stress being higher among healthcare staff (BA, t = −2.49, p = .014). However, when the concern was high, no statistically significant differences in stress levels were observed in any group of workers (ba, t = 1.09, p = .277). Therefore, being healthcare staff was related to higher levels of stress only when the level of one's health concern was low. When this concern was high, stress affected healthcare staff and general workers alike.

Interaction effect between concern for one's own health and health staff on stress.
Third (Figure 3), the healthcare staff*work overload interaction showed that stress levels were similar in participants who did not report work overload, either among general workers or healthcare staff (AB, t = 0.75, p = .941). Statistically significant differences were found between participants who reported work overload and those who did not, but only regarding healthcare staff (Bb, t = −2.61, p = .010), without observing these differences among general workers (Aa, t = −2.44, p = .807). There were neither differences between healthcare staff and general workers when work overload was reported (ab, t = −1.43, p = .157). Thus, being healthcare staff was related to higher levels of stress only when these workers claimed to have work overload, as compared to being healthcare staff and not reporting work overload. Among general workers, work overload did not increase stress.

Interaction effect between work overload and health staff on stress.
As differences were found between men and women regarding levels of stress, but this not resulting in being a predictive variable in the regression model, nor in the interaction with the other variables, it was analysed whether the effect of gender on stress would be mediated by the WHI, income, and concern about the economy. The resulting regression models are shown in Table 5. Thus, Model 1 (R2 = .04; F = 11.17; p = .001) showed a significant main effect of gender on the income variable (β = 0.75, t = 3.34, p = .001); Model 2 (R2 = .14; F = 7.02; p < .001) showed a significant main effect of income (β = −0.71, t = −6.34, p < .001) on the concern for the economy variable; and Model 3 (R2 = .08; F = 7.42; p = .01) showed a significant main effect of gender (β = −0.24, t = −2.53, p = .012), income (β = 0.07, t = 2.10, p = .037), and concern for the economy (β = 0.06, t = 3.99, p < .001) on the WHI; on Model 4 (R2 = .47; F = 55.86; p < .001), the effects of these variables on stress were observed, being statistically significant the income variable (β = −1.01, t = −2.89, p = .004), concern for the economy (β = 0.51, t = 2.74, p = .007), and the WHI (β = 8.39, t = 12.22, p < .001), although not directly gender (β = −0.10, t = −0.88, p = .378). The total effect of gender on stress was statistically significant (β = −3.56, t = −2.67, p = .008), as was the total indirect effect (β = −0.27, SE = 0.10, 95% CI [−0.48, −0.08]).
Regressions testing income, economic concern and WHI as mediators in the relationship between gender and stress.

SE (HC4) = heteroscedasticity-consistent covariance matrix estimators HC4; LL = Lower limit; UL = Upper Limit; 95% CI = 95% Confidence Interval; Gender (0 = Female; 1 = Male); *PS = Partially standardized effects.
As shown in Figure 4, five pathways of indirect effects of gender on stress were observed; (1) through income (β = −0.08, SE = - 0.04, 95% CI [−0.16, −0.02]); (2) through WHI (β = −0.21, SE = 0.08, 95% CI [−0.38, −0.05]); (3) through the connection between income and concern for the economy (β = −0.03, SE = 0.02, 95% CI [−0.06, −0.01]); (4) through the connection between income and the WHI (β = 0.04, SE = 0.03, 95% CI [0.01, 0.10]); (5) through the connection between income, concern for the economy, and the WHI (β = −0.03, SE = 0.01, 95% CI [−0.06, −0.01]). Therefore, (1) being a woman was associated with lower income, which in turn predicted higher levels of stress; (2) being a woman was related to greater WHI and this, in turn, to greater levels of stress; (3) being a woman was associated with lower income, which in turn was related to greater concern for the economy, and therefore with higher levels of stress; (4) being a woman predicted lower income, which was related to greater WHI and, in turn, to higher levels of stress; and finally, (5) being a woman was associated with lower income, which predicted greater concern for the economy and, in turn, greater WHI and, therefore, higher stress levels.

Mediation model. Direct and indirect effects of Gender, Income, Economic concern and WHI on Stress.
Discussion
The main purpose of this research was to analyze stress levels among workers, both healthcare and non-healthcare, and their relationship with gender and the WHI during the second wave of the COVID-19 pandemic in Spain, as well as the incidence of other sociodemographic factors and health and economic concerns. The interest in including both labour profiles was due to the proliferation of studies focused on the psychological and social impact of the pandemic, on the one hand, on the general population, regardless of working or not, and, on the other hand, on healthcare workers. In this way, a novel vision of perceived stress is provided regarding working men and women and their relationship with the WHI and other sociodemographic and labour variables that needed to be clarified in the light of previous studies and in context of this exceptional pandemic.
First, it was hypothesized that the WHI would be a predictor of perceived stress in the study sample (Hypothesis 1), which was supported by the data found. Thus, in line with Lourel et al. 35 and Triplett et al., 36 people who reported a greater impact on their family role due to occupational demands also felt higher levels of stress. It is indisputable that the pandemic has led to an increase in labour demands that in many cases have been confronted with a significant lack of resources, a complex situation, and a source of stress for employees. 55 Therefore, it is logical to think that when this scenario is also joined by the demands of home care and maintenance, the situation can be overflowing and detrimental to the health of workers, which in turn feeds back to their already affected work and family performance.
Similarly, it was hypothesized that being a woman would be a predictor of the stress suffered in the second wave of COVID-19 (Hypothesis 2). An analysis of the differences in mean scores between men and women yielded higher scores in the latter, although in the regression model, when the other variables were analyzed together, gender was not a significant factor. Far from finishing the analyses at this point, the research team wanted to go further and explore whether the effect of gender on stress was rather indirect and mediated by other relevant variables. In this way, the mediation of the WHI, income, and concern for the economy was observed, concluding that being a woman would be a risk factor for higher stress levels during the pandemic, something that previous works have already pointed out.26,28
Thus, this sample reproduces the existing pattern regarding the gender pay gap which is also recognized by international states.9,10 Women receive lower wages as compared to men, which is a source of stress in itself. In addition, lower incomes are linked with greater concern for the economy in a scenario of uncertainty not only related to health, but also to social aspects, in which many jobs have been affected by the incidence of COVID-19. This situation predisposes people to suffer more stress, both directly and indirectly, by being more concerned about the future economic situation and with this influencing a greater conflict between work and family roles.
More importantly, according to the results found, there would be differences between men and women regarding the level of stress due to the mediation of the WHI, so women's family life would be more affected due to their working role and this, in turn, would imply a greater level of stress. These results, which are in line with works such as that by Van der Lippe & Lippényi 43 or that of Jorquera-Gutiérrez, 39 are consistent with national statistics on the differential distribution of hours between paid and unpaid work according to gender. Despite progress, women continue to bear the greatest burden on household chores, education, and dependent care, which is increased when they take part-time jobs, unlike men, whose working hours at home are not altered by the type of working day. 56 To this, we must add the high feminization existing in the most affected sectors by the pandemic,8,57 which helps to understand the results found in this research. As already mentioned, the divergence of results in the scientific literature on the WHI between men and women should be understood through contextual reasons as pointed out by Hagqvist et al., 45 for example, the country where the study is developed, temporality, or the type of labour sector.
On the other hand, it was also established as Hypothesis 3 that stress would be higher in those living with younger children, although in this case, the data did not support this hypothesis, just as differences were not found depending on marital status or living with dependents. These findings coincide with the conclusions by Kassim et al. 31 and Wang et al., 29 whose work at the beginning of the pandemic showed no relationship between these variables. It should be noted that the number of participants responsible for the care of dependents was very small in this sample, which requires caution with the conclusions derived from these results.
Differences were observed in the WHI regarding the parental status, so the greatest degree of conflict between the two areas was detected in those with children under their charge. These results are consistent with what was noted by Jansen et al., 42 although they differ with Jacukowicz & Merecz-Kot, 40 who found no differences in this regard, possibly because these authors studied the WHI in online workers and where there was also a small number of participants with younger children. Based on the results found, it could be understood that having younger children means a higher likelihood of impairing the WHI as they perceive that the demands of their work negatively affect their relationship with their children or their care functions. However, their stress levels were similar to those of participants without children in charge, so other factors would be the ones that have the greatest contribution to this state of mental health, as has been shown in this work.
In addition, it was hypothesized that healthcare staff would have higher levels of stress as compared to general workers (Hypothesis 4). Although it was observed that there was a greater WHI among the healthcare staff, there was no evidence of the main effect of this variable on stress. Rather, it was noted that the type of labour sector (health vs. general) moderated the relationship between concern for health and stress itself, and also between work overload and stress. On the one hand, when people were highly concerned about their health in relation to COVID-19, the labour sector to which they belonged was indifferent. However, differences according to the labour sector arose among those with low levels of concern for their health, being here where healthcare staff reported the highest levels of stress. This finding may be better understood by the following interactions cast by the regression model, which showed that participants in the healthcare sector were more stressed than non-healthcare workers when reporting work overload. Therefore, concern for health itself and work overload were more decisive factors in explaining stress than being healthcare staff or not.
Mira et al. 58 compared the stress levels experienced by healthcare staff at different times of the pandemic and, according to the different stages of disaster established by Myers & Zunin, 59 noted that there was an increase in stress as time passed and as the pandemic situation stabilized, naming this stage as a phase of disappointment. Therefore, following this evidence, it could be understood that the stress and fatigue detected at the beginning of the pandemic would be lower compared to later moments, both for the healthcare staff and for the rest of the population. What would greatly aggravate the healthcare staff's situation is the work overload, being the ones facing the disease and its most dire consequences on the front line, with great uncertainty and, in many cases, with a lack of resources and high concern for infecting themselves and their relatives.60,61
Similarly, differences in stress levels and the WHI were explored depending on the age of the participants, as the scientific literature has reported divergence of results in this regard. For example, some studies find a high WHI in older workers, 40 as compared to others that show higher levels in the group of 25 to 36 years. 42 In addition, as mentioned above, some studies do show a relationship between age and stress as, in this case, the greater the stress levels the lower the age, 28 but there are also other works that do not find a relationship between these two variables.18,29 Therefore, simply addressing the correlational analysis carried out in this research, a negative relationship is established between age and stress, and between age and the WHI, i.e. younger workers had higher levels of stress and also a higher WHI. However, when looking at the relationship between age and stress in depth according to the interaction provided in the regression model, it is shown that age would be a moderating variable for the link between stress and concern for one's health. Thus, among those who were less concerned about their health, the stress levels were higher the younger they were, while stress was high when the concern was also high, regardless of the age of the participant.
Certain limitations should be noted in this study. The first refers to the sample selection method, which did not follow probabilistic sampling, so caution must be taken when generalizing the results. In addition, the lower number of men in the sample should be considered and the small number of workers with dependents in charge. It should also be considered as a limitation for the interpretation of the results of the present study that the percentage of women in the sample is 76%, which is somewhat higher than the statistical reality collected by the Spanish National Institute of Statistics for the general population (56% of women). 62 However, this difference in percentage between women and men is similar to that reported by the National Statistics Institute 63 in relation to the total number of subjects that are registered as health workers in Spain, being the percentage of female health workers around 70%, and around 30% for males. Therefore, the interpretation of the results should be made with caution, although they represent a very interesting approximation of the impact of the Covid-19 pandemic on the WHI.
Future research could follow this line of study by also analyzing stress progression longitudinally at different times of the pandemic and linking it to the incidence of confirmed COVID-19 cases and geographical deaths. It would also be necessary to continue to analyze the impact of the pandemic on working women, on the multiplicity of roles, on the effect that telework has on the family-work balance and its impact on the workers’ career promotion or path.
Conclusions
This research has analyzed the unequal impact of the COVID-19 pandemic on mental health and the work-family situation of men and women living in Spain during the second wave of contagions, including a representation of healthcare workers as the main workforce in this global crisis. The main contribution of this research has been to show that being a working woman poses a risk of stress due to the mediation of contextual variables that continue to be rooted in social organization, such as the pay gap and the greater conflict between work and family roles that women experience. While it is true that the situation in Spain on the gender gap has improved considerably in recent years, as the 2018 figures published by the European Institute for Gender Equality 7 show, the COVID-19 pandemic puts these developments at risk and it is vital for governments and health agencies to keep in mind when planning new measures, that equality between men and women is not yet a full reality in most countries and that there is still a long way to go.
Footnotes
Availability of data and material
The data that support the findings of this study are available from the corresponding author, [SDS], upon reasonable request
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [Carmen Rodríguez-Domínguez, Sara Domínguez-Salas and Juan Gómez-Salgado]. The first draft of the manuscript was written by [Carmen Rodríguez-Domínguez, Sara Domínguez-Salas, Regina Allende-Cussó, Macarena Romero-Martín, Juan Gómez-Salgado and Carlos Ruiz-Frutos] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The project was approved by the Research Ethics Committee of Huelva, belonging to the Regional Ministry of Health of Andalusia, Spain (PI 036/20-2).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.