
Abstract
Obesity can be a major problem due to its potential to cause a number of health issues, including high blood pressure and diabetes. Many reports have come out of Palestine on overweight and obesity and their direct link to non-communicable diseases, although there is only limited evidence available on the connection between obesity and hypertension in Palestinian adults. We aimed to look at the associations between anthropometric and body composition variables and blood pressure in a large population of Palestinian adults (1337 subjects) and determine which anthropometric indices most strongly correlate with high blood pressure. Anthropometric measurements including height, waist circumference (WC), hip circumference (HC), body mass index (BMI), and total body fat (TBF) were assessed. A body composition analyzer was used to measure body weight, fat mass and fat-free mass. Systolic (SBP) and diastolic (DBP) blood pressure were measured using a Dinamap vital signs monitor. In both males and females, all the anthropometric measurements showed significant strong positive correlations with mean SBP and mean DBP (p < 0.01). SBP correlated the most strongly with waist circumference in all subjects (r = 0.444 in females, r = 0.422 in males), while DBP correlated the most strongly with WC in males (r = 0.386), but with TBF in females (r = 0.256). By controlling fat percentage, WC, HC, and BMI, which are affected by extra weight and lack of exercise, blood pressure levels can be regulated.
Introduction
Globally, obesity is increasing dramatically and may cause many diseases and health problems, including high blood pressure, type 2 diabetes, and certain types of cancer. 1 In 2016, the World Health Organization announced that almost two billion adults worldwide were overweight and about 650 million were obese. 2 Obesity is one of the leading causes of cardiovascular diseases (CVD) and death, 3 this, together with overweight, are the main adjustable risk factors for high blood pressure. 4 Obesity could be a major problem due to its potential to cause a number of health issues, including high blood pressure and diabetes, 5 indeed, many studies report that high blood pressure is related to increased obesity. 6 Nevertheless, there is limited evidence available on the connection between obesity and hypertension in Palestinian adults. This has led researchers to look at various anthropometric measurements, including waist circumference (WC), hip circumference (HC), waist-to-hip ratio (WHR), waist-to-height ratio (WHtR), and visceral fat (VF), as well as skin fold thickness to determine which variables correlate most closely with CVD or are useful for assessing risk.7–9 Measurements of body fat have traditionally been limited to simple assessments such as WC, HC, WHR, and BMI.
Palestine consists of two separate areas, the Gaza Strip and the West Bank, with 2.72 million people in the West Bank and 1.7 million in the Gaza Strip. 10 Obesity and overweight are enormous public health problems in Palestine and a study of Palestinian adults in a rural community estimated the prevalence of obesity as being 58.7% and 71.3% among males and females, respectively.11,12 The first national survey of overweight and obesity in Palestine revealed that over 60% of the Palestinian population aged between 18 and 64 is overweight (38.0%) or obese (24.4%), 11 similar to the results of an earlier study of Palestinians in rural areas of the West Bank that found obesity levels of 37% in women and 18% in men. 13 Indeed, there are many reports from Palestine that directly associate overweight and obesity with non-communicable diseases. 14 Many anthropometric indicators are used to measure obesity, but there is no consensus on which of these human indicators best defines obesity and determines an increased risk of high blood pressure. 15 Due to the increasing challenges to the health of the Palestinian population in the occupied Palestinian territory, the national health plans have recognized the need to tackle the existence of obesity-related diabetes and cardiovascular disease (CVD). 16 To elucidate this issue, we looked at the associations between anthropometric and body composition variables (weight, BMI, WC, HC, and TBF) and blood pressure in a large population of Palestinian adults. There exists a need for an easy and effective obesity measurement to aid in assessing risk, informing the most appropriate management approaches, and developing preventive strategies. However, the simplest measure of obesity often helps predict the risk factors for cardiovascular disease.8,17,18 Therefore, this study aimed to try to ascertain which anthropometric index most strongly correlates with high blood pressure in the Palestinian population.
Method
Study design and participants
A cross-sectional study was conducted from October 2018 to December 2018 on a sample of Palestinian adults recruited from public health centers in the West Bank (Hebron, Nablus, and Ramallah). These cities were selected based on convenience and therefore the public health centers were selected randomly for inclusion. Recruitment days were announced through health centers in each city. Possible study participants were informed about the aim of the study and its procedures and received a consent form, including an in-depth description of the study. The inclusion criteria required that the participants had healthy movement or were not taking anticonvulsants, and did not suffer from any kind of physical disorder or infection where cramping could occur or the person could fall suddenly while the body measurements were being taken, or that due to a lack of normal movement they were unable to stand on the body composition analyzer. In total, 1337 adults aged 40 to 64 years old participated in this study.
Ethical consideration
The research protocol was approved by the ethical committee of the Arab American University-Palestine involved in the study (approval no. 1626952020). Prior to data collection, each participant was informed that this interview and anthropometric measurements would be completely voluntary, no identification was required, and there was no risk involved with participating in this study. Permission for the study was obtained from the Palestinian Ministry of Health and it was performed according to the International Code of Medical Ethics established by the World Medical Association and the Declaration of Helsinki.
Anthropometric measurements
The anthropometric measurements were recorded by trained nurses using a standard procedure ensuring inter-observer reliability. They included height, WC, HC, WHR, and WHtR. Anthropometric indicators were assessed for all the participants, using standardized equipment and methods. While collecting this data, all the participants wore light clothing; all measurements were taken twice and the mean was recorded. Each participant's height measurement was taken twice in the standing position, without shoes, using a portable stadiometer. WC was measured twice with a metric tape measure over light clothing at the level of the umbilicus, halfway between the lower rib margin and the iliac crest, with no pressure being put on the skin. During this measurement, the participants were asked to stand upright, breathe normally, and relax their abdomen. HC was measured twice at the maximum width of the buttocks in a standing position with the feet together. The means of the two values for each measurement were used in the analysis. Height and weight measurements were utilized to determine BMI by using weight (kg) divided by height squared (m2) expressed as kg/m2 according to international standards.
Body composition measurements
A body composition analyzer (TANITA BC-418MA®) was used to measure body weight (kg), fat mass (kg), percentage of fat mass (%), and fat-free mass (kg) to the nearest 0.1 kg. This was done twice while participants were dressed in light clothing, without shoes. Measurements were taken in the morning when no food had been consumed and no exercise had been undertaken in the preceding 8 h, under resting conditions.
Blood pressure
Systolic (SBP) and diastolic (DBP) blood pressure were measured using a Dinamap vital signs monitor (Model BP 8800, Critikon, Inc., Tampa, Florida), following the recommendations of the European Heart Society (on the right arm in a semi-flexed position at heart level, with the participants in a supine position and after 10 min of rest). Readings of SBP ≥130 mmHg and DBP≥80 mmHg in adults are taken as being hypertensive; readings of SBP <120 mmHg and DBP<80 mmHg are normotensive. 19
Statistical analysis
We described numerical variables using the mean ± standard deviation, while qualitative or nominal variables were described using percentages and frequencies. The independent two-sample t-test was used to compare the variables between female and male study participants. Pearson and partial correlation coefficient analyses (r) were used to test the relationships between human variables, body composition variables, and blood pressure values. Body composition variables were compared according to blood pressure categories (normal or hypertensive). SPSS Statistics version 26.0 (SPSS. Chicago. IL, USA) was used for all the analyses; p values < 0.05 were considered to be statistically significant.
Results
One thousand three hundred thirty-seven participants were recruited into the study. The average age of the participants was 47.25 ± 7.37 years though the females were significantly younger than males (p < 0.05), as well as being significantly shorter and lighter (Table 1).
Demographic information and anthropometric measurements of the participants.

WC = waist circumference; HC = hip circumference; BMI = body mass index; WHR = waist-to-hip ratio; WHtR = waist-to-height ratio; SBP = systolic blood pressure; DBP = diastolic blood pressure. *p < 0.05.
Prevalence of hypertension and normotension. 19

*Hypertensive is where SBP ≥130 mmHg and DBP≥80 mmHg; Normotensive is where SBP < 120 mmHg and DBP<80 mmHg. 19
Males tended to have a higher WC compared to females although the differences were not statistically significant. Males also had significantly larger WHR and greater total fat (%), but females had significantly larger BMI and HC than males (31.22 ± 6.45 kg/m2 and 108.82 ± 12.92 cm vs 28.24 ± 4.96 kg/m2 and 101.64 ± 10.80 cm, respectively; p < 0.01). Although females were shorter than males, they had a significantly higher WHtR (0.60 ± 0.09 vs 0.56 ± 0.07, p < 0.01). Males on the other hand had significantly higher SBP (133.86 ± 14.68 mmHg vs 130.34 ± 16.52 mmHg, p < 0.01) and DBP (84.39 ± 8.09 mmHg vs 82.88 ± 8.76 mmHg, p < 0.01) compared to females.
Sex-specific analysis showed that more males were normotensive compared to females (52.0% vs 48.0%). The overall prevalence of hypertension in males was 61.7% compared to 38.3% in females (Table 2).
The differences in anthropometric data between normotensive and hypertensive subjects are explored in Table 3. Hypertensive participants were older than the normotensive subjects and had a significantly higher BMI (31.98 ± 6.00 kg/m2 vs 28.35 ± 5.39 kg/m2), WC (103.60 ± 10.89 cm vs 93.45 ± 12.86 cm), and HC (109.53 ± 11.47 cm vs 102.47 ± 12.06 cm).
Comparison of anthropometric data between normotensive and hypertensive subjects.
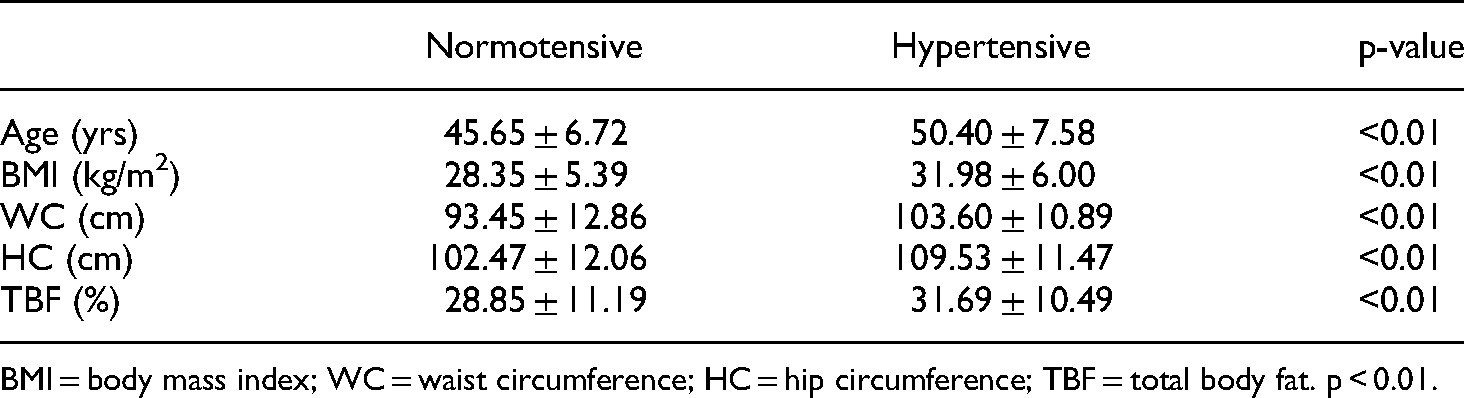
BMI = body mass index; WC = waist circumference; HC = hip circumference; TBF = total body fat. p < 0.01.
Differences in human body measurements were detected between the normotensive and hypertensive populations, as can be seen in Table 4. The mean values of BMI, WC, HC, and TBF were significantly higher in hypertensive compared to normotensive participants for both sexes (p < 0.01).
Anthropometric indicators in hypertensive vs normotensive study participants.

BMI = body mass index; WC = waist circumference; HC = hip circumference; TBF = total body fat.
The relationship between the anthropometric measurements (BMI, WC, HC, and TBF) and both mean systolic and mean diastolic blood pressure was explored through partial correlation coefficients (Table 5). In both males and females, all the anthropometric measurements showed a significant moderate positive correlation between mean SBP and mean DBP (p < 0.01).WC had the moderate correlation with SBP (r = 0.444 in females, r = 0.422 in males), although WC had the moderate correlation with DBP in males (r = 0.386); in females total body fat had the moderate correlation with DBP (r = 0.256). The next-strongest correlation with SBP was BMI in females and TBF in males. The next-moderate correlation with DBP was WC in females, while in males this was with HC.
Partial correlation coefficient between anthropometric indicators and blood pressure.

BMI = body mass index; WC = waist circumference; HC = hip circumference; TBF = total body fat; SBP = systolic blood pressure; DBP = diastolic blood pressure.
The presence of hypertension correlated significantly with all of the anthropometric measurements (BMI, WC, HC, and TBF) in both males and females (p < 0.05) (Table 6).
Correlation between hypertension and anthropometric measurements.
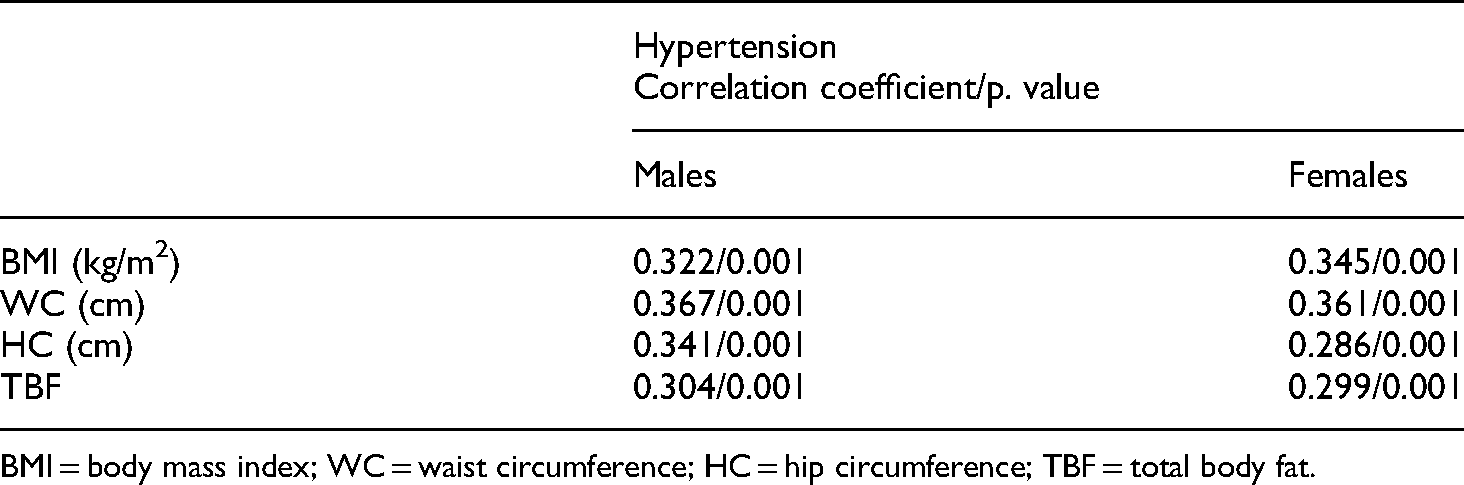
BMI = body mass index; WC = waist circumference; HC = hip circumference; TBF = total body fat.
Furthermore, multiple linear regression was performed to assess the predictors of hypertension among the participants. The results showed that age, height, and waist circumference were the significant predictors of hypertension (P < 0.05), as seen in (Table 7).
Predictors of hypertension.

Dependent Variable: hypertension, R2 = 0.118, Adjusted R2 = 0.112, F = 19.7.
Discussion
It is important to identify the anthropometric measurements that may be useful for predicting the risk of cardiovascular disease associated with obesity in adults. In this study, we assessed four anthropometric measurements, BMI, WC, HC, and TBF.
We found differences in the mean values of anthropometric measurements, in addition, to mean systolic and diastolic blood pressures in males and females, in line with the findings of other authors (who reported different mean values of WC, HC, BMI, height, weight, SBP, and DBP.20,21 These differences in height, weight and other anthropometric measurements are normal due to sexual dimorphism in humans. Our results found that there was a difference between normotension and hypertension according to the age and anthropometric measurements of the participants, which supports other studies conducted in this field.22,23 Age is a known risk factor for high blood pressure. 24 However, these studies used WC, BMI, HC and WHR data.
The major findings of this study are that SBP and DBP correlate in a statistically significant way with all the anthropometric measurements studied (BMI, WC, HC, and TBF). Our results are comparable with previous studies from different countries, in terms of a significant relationship between anthropometric measurements and increased SBP and DBP.21,22 Likewise a study of urban black South African adults reported an association between various adiposity indices and blood pressure and hypertension, where all body composition parameters studied, including WC, BMI, and body fat %, were positively associated with SBP and DBP in both sexes. 25 These results should motivate healthcare providers in Palestine to conduct anthropometric evaluations to determine the risk of hypertension in patients.
WC correlated strongly with SBP in both females and males and also correlated well with DBP in males. Indeed Choy et al. found an association between increased waist circumference and high blood pressure. 26 This result agrees with a cross-sectional study aimed at determining human measurements, which reported that WC predicts high blood pressure among adults in the Kingdom of Saudi Arabia, in addition to being an important indicator for SBP and DBP levels as well as all types of high blood pressure subtypes, with the exception of isolated diastolic hypertension. 17 Our results for WC also agree with a study of young South African adults that investigated the influence of various anthropometric variables on blood pressure. The main result of that study was that the presence of hypertension or pre-hypertension was significantly associated with WC in both sexes. 20 Moreover, a study of Brazilian men was conducted to assess which body measurements are most closely related to high blood pressure. That work reported a consistent increase in systolic and diastolic blood pressure with increased WC and BMI. 27 It is clear, then, that weight reduction interventions that include lifestyle modifications are necessary to reduce adult hypertension.
In our study, all the anthropometric measurements were significantly higher in hypertensive participants of both sexes. Another study supporting this finding reported a positive relationship between BMI and hypertension. 28 In addition, data from a cohort study indicated that BMI was one of the main factors related to hypertension. 29 A further study found a positive relationship between BMI and WC and blood pressure. 30 In addition, a study involving the impact of sex-specific body composition on cardiovascular risk factors in a Chinese population reported that WC and HC were both positively associated with the presence of hypertension, dyslipidemia, and diabetes. 31 The positive relationship between obesity markers, including WC, BMI, HC and blood pressure levels, demonstrates the need to develop effective strategies to prevent overweight and obesity in Palestinian adults. The main limitation of the study was that only the specific age group (40–64) was included in the study.
Conclusion
Average WC, HC, total body fat, and BMI values were significantly higher in both male and female study participants with high blood pressure than in those who were normotensive. We found a positive correlation between all the anthropometric indicators and systolic and diastolic blood pressure. High values for anthropometric indicators such as HC, WC, fat mass percentage, and BMI are linked to high blood pressure. This work highlights the importance of using these simple human body measurements to predict high blood pressure in both males and females. By controlling the percentage of fats, WC, HC, and BMI, which are affected by the extra weight and lack of exercise, blood pressure levels can be regulated.
Footnotes
Acknowledgements
This manuscript is part of the PhD research developed by Moath Abu Ejheisheh, included in the Official PhD Program of Clinical Medicine and Public Health at the University of Granada, Spain. The authors in this study would like to extend her appreciation to the study participants for their time.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Moath Abu Ejheisheh is Assistent professor in adult health nursing at Palestine Ahliya University/Palestine. His research focus on the topics of adult health nursing and Nursing education.
Ahmad Batran is Associate professor in pediatric nursing at Palestine Ahli ya University/Palestine. His research focus on children health and neonate care.
Ahmad Ayed is Assistant professor in pediatric nursing at Arab American University Palestine. His research includes a focus on the topics of pediatric nursing, Health promotion, and methods of enhancing learning in nursing.
María Correa-Rodríguez, PhD, is a professor, Faculty of Health Sciences. Department of Nursing, University of Granada and researcher in Institute de investigacion Biosantaria (ibs, Granada), Spain.
Ángel Fernández-Aparicio, MSc, is professor at the Faculty of Health Sciences in Melilla (Spain), Department of Nursing, University of Granada and reseacher at the instituto delnvestigacion Biosanitaria (ibs, Granada), Spain.
José Luis Gómez-Urquiza, PhD, profeesor at the faculty of health sciences in Ceuta (Spain), department of nursing, University of Granada.
Jacqueline Schmidt-RioValle, PhD, is professor, Faculty of Health Sciences, Department of Nursing, University of Granada and researcher at Centro y Comportamiento (CIMCyC) and researcher CTS-436 Group. Granada, Spain.