
Abstract
Coronavirus disease 2019 (COVID-19) has been declared a pandemic by the World Health Organization; it has affected millions of people and caused hundreds of thousands of deaths. Patients with COVID-19 pneumonia may develop acute hypoxia respiratory failure and require noninvasive respiratory support or invasive respiratory management. Healthcare workers have a high risk of contracting COVID-19 while fitting respiratory devices. Recently, European experts have suggested that the use of helmet continuous positive airway pressure should be the first choice for acute hypoxia respiratory failure caused by COVID-19 because it reduces the spread of the virus in the ambient air. By contrast, in the United States, helmets were restricted for respiratory care before the COVID-19 pandemic until the Food and Drug Administration provided the ‘Umbrella Emergency Use Authorization for Ventilators and Ventilator Accessories’. This narrative review provides an evidence-based overview of the use of helmet ventilation for patients with respiratory failure.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome related coronavirus 2 (SARS-CoV-2), 1 was declared a pandemic by the World Health Organization on 11 March 2020. 2 The COVID-19 pandemic has affected millions of people and caused hundreds of thousands of deaths worldwide. 3 People with severe COVID-19 develop hypoxemic acute respiratory failure (ARF) and require noninvasive respiratory support or invasive respiratory management.1,4,5 Healthcare workers have a high risk of contracting SARS-CoV-2 via large droplets, respiratory secretions, contact with contaminated surfaces, or exposure to exhaled air within a distance of 0.5–1.0 m while fitting a respiratory device.6,7 During the initial outbreak of COVID-19 in China, medical teams recommended early endotracheal intubation to avoid clinical deterioration. 8 This approach was also suggested by Marini and Gattinoni in a JAMA editorial. 9 However, the unprecedented number of patients outnumbered the limited supply of ventilators and the capacity of intensive care units (ICUs). Thus, some experts have argued that intubation and mechanical ventilation were employed too early10,11 and that noninvasive respiratory support should be used to prevent clinical deterioration and the complications of mechanical ventilation. 11 Noninvasive respiratory support—including conventional oxygen therapy (COT), the heated humidified high-flow nasal cannula (HFNC), continuous positive airway pressure (CPAP), and noninvasive positive pressure ventilation (NIPPV)—may reduce the need for ventilators and ICU beds. A recent study revealed that delivering noninvasive respiratory support outside the ICU is a feasible strategy. 12 A report from China indicated that 41% of patients with COVID-19 required oxygen therapy. 13 The average NIPPV usage in China was 20.1% (range, 4.9%–56%),4,5,14 whereas the average HFNC usage was 22.8% (range, 0%–63.5%),5,14 However, whether noninvasive respiratory support increases the degree of virus aerosolisation and spread of virus-bearing droplets remains controversial.15–17 Recently, European experts recommended helmet CPAP as the first therapeutic choice for hypoxemic ARF caused by COVID-19 because it reduces the spread of the virus into the ambient air.18–21 By contrast, in the United States, helmets were not common in respiratory care before the COVID-19 pandemic. On 24 March 2020, the United States Food and Drug Administration (FDA) provided the ‘Umbrella Emergency Use Authorization (EUA) for Ventilators and Ventilator Accessories’ to relieve the insufficient supply of FDA-cleared ventilators and ventilator accessories for use in healthcare settings to treat patients during the COVID-19 pandemic. This EUA authorised the use of two helmets, namely the Subsalve Oxygen Treatment Hood (Lombardi Undersea LLC, Middletown, RI, USA) and the StarMed CaStar-R (Intersurgical, Wokingham, UK), on 4 and 14 August, respectively. 22 The present narrative review provides an evidence-based overview of the use of helmet ventilation in patients with respiratory failure.
Dispersion of exhaled air
Noninvasive respiratory support is essential in the treatment of COVID-19; however, exhaled air can promote dispersion of the virus, thus increasing the risk of nosocomial infection. 23 Because droplets from patients with COVID-19 are currently considered a major route for transmission, healthcare workers must be aware of the dispersion of exhaled air during noninvasive respiratory support.15,24,25 Hui et al. examined exhaled air dispersion during COT, HFNC, CPAP, and NIPPV (Table 1). In these in vitro studies, smoke laser visualisation was used to assess the dispersion distance of exhaled air from a high-fidelity human patient simulator in a hospital bed reclined at 45°.26–33
Dispersion of exhaled Air in In vitro models of noninvasive respiratory support.
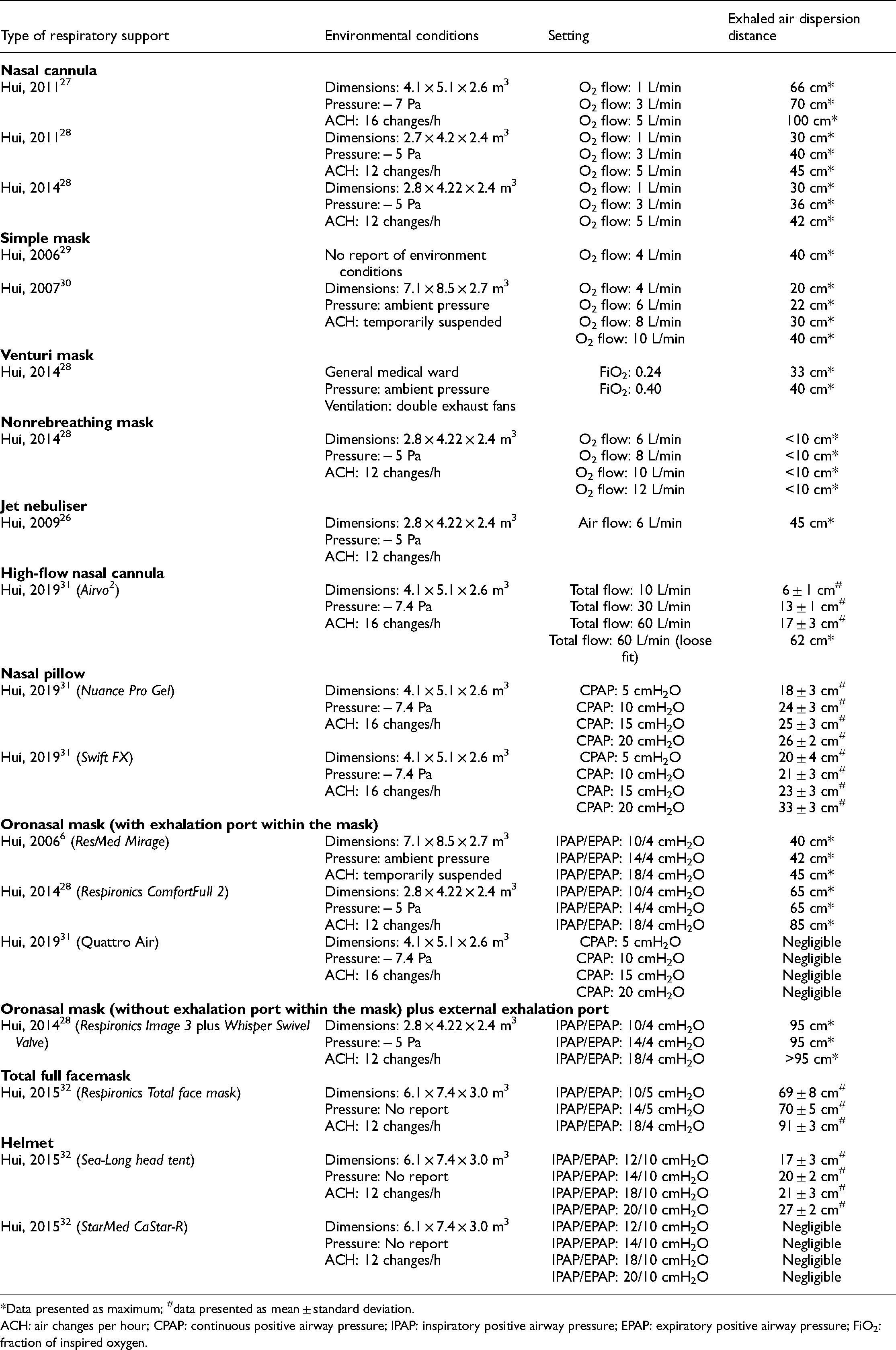
*Data presented as maximum; #data presented as mean ± standard deviation.
ACH: air changes per hour; CPAP: continuous positive airway pressure; IPAP: inspiratory positive airway pressure; EPAP: expiratory positive airway pressure; FiO2: fraction of inspired oxygen.
COT via a nasal cannula
COT via a nasal cannula with an oxygen flow rate of 3 L/min was performed in differently sized negative pressure rooms; the maximal distance of exhaled air dispersion was 36–70 cm.27,28 When the oxygen flow was increased to 5 L/min, the maximal distance of exhaled air increased to 100 cm. 27
COT via a simple mask
For COT via a simple mask, the maximal exhaled air dispersion was 40 cm for an oxygen flow rate of 4 L/min, but details of the environmental conditions were not provided. 29 Another examination was conducted in a laboratory room, and a jet plume of air leaked through the side vents to lateral distances of 40 cm during the delivery of oxygen at a flow rate of 10 L/min. However, room ventilation was temporarily suspended for this test, which is not a realistic scenario. 30
COT via a Venturi mask
Use of COT via a Venturi mask was evaluated in a general ward with ambient pressure and double exhaust fans for room ventilation. When the fraction of inspired oxygen (FiO2) for the Venturi mask was 0.24 and 0.4, the exhaled air dispersion distances were 33 and 44 cm, respectively. 28
COT via a nonrebreathing mask
Because of its one-way valves, the nonrebreathing mask reduced the exhaled air dispersion distance to less than 10 cm, even for an oxygen flow rate of 12 L/min. 28
Jet nebuliser
A jet nebuliser with an airflow of 6 L/min yielded a maximum exhaled air dispersion distance of 45 cm. 26 The National Institute for Health and Care Excellence 34 and The Global Initiative for Chronic Obstructive Lung Disease 35 have suggested that regular inhalation therapy should be maintained for patients with chronic obstructive lung disease. Because exhaled air is a concern, healthcare workers should consider using pressurised metered-dose inhalers (pMDIs), dry powder inhalers (DPIs), or soft mist inhalers (SMIs) instead of jet nebulisers. Use of valved holding chambers with pMDIs or SMIs is also possible. DPIs are breath-actuated devices; healthcare workers should pay attention to coughs caused by DPI use. The use of nebulisers for patients with COVID-19 is controversial,36,37 and unnecessary or unproven nebulisation therapies should be avoided.38,39
High-flow oxygen therapy via a nasal cannula
When an HFNC was appropriately inserted into the nostril, exhaled air was detected at distance of up to 6, 13, and 17 cm when the total flow rate was 10, 30, and 60 L/min, respectively. However, the dispersion distance of exhaled air gradually increased to 62 cm as the fit between the nasal cannula and nostril became looser. 31
High-flow oxygen therapy via tracheostomy
The dispersion of exhaled air during the application of high-flow oxygen therapy via tracheostomy has not been examined. The large expiratory port on the high-flow tracheostomy interface (OPT970, Fisher & Paykel Healthcare, Auckland, New Zealand) is designed for exhalation; thus, considerable leakage and a large distance of exhaled air dispersion might reasonably be expected. 40 Based on our experience, high-flow tracheal oxygen is not recommended for patients with suspected or confirmed COVID-19.
CPAP via a nasal pillow
Two nasal pillows (i.e. Respironics Nuance Pro Ge and RedMed Swift FX) were tested with CPAP values of 5, 10, 15, and 20 cmH2O. Similar exhaled air dispersion distances were observed for the Respironics Nuance Pro Ge and RedMed Swift FX (26 and 33 cm, respectively). 31
CPAP via an oronasal facemask (with exhalation port)
No significant exhaled air dispersion was observed from the Quattro Air mask, even with a CPAP of 20 cmH2O. 31 In contrast to NIPPV, CPAP provides constant airway pressure during the respiratory cycle; thus, leakage was limited by the absence of a delta pressure between the inspiratory positive airway pressure (IPAP) and expiratory positive airway pressure (EPAP).
NIPPV via an oronasal facemask (with exhalation port within the mask)
The maximal dispersion distance of exhaled air during the application of NIPPV via an oronasal facemask with an exhalation port within the mask was 45 cm for an IPAP of 18 cmH2O and an EPAP of 4 cmH2O. However, the environmental conditions of this test were unrealistic because the room ventilation was temporarily suspended. 6 This examination was performed again in a negative pressure isolation room several years later, and the maximal exhaled air dispersion distance was increased to 85 cm for an IPAP of 18 cmH2O and an EPAP of 4 cmH2O. 28
NIPPV via an oronasal facemask (without exhalation port within the mask) plus external exhalation port
When the oronasal facemask does not contain an exhalation port, an additional exhalation port should be applied to create a continuous leakage path and prevent carbon dioxide (CO2) rebreathing during NIPPV with a single limb breathing circuit. The maximal exhaled air dispersion distance was 95 cm for the oronasal facemask connected to a Whisper Swivel Exhalation Port. 28
NIPPV via a total full facemask
Exhaled air dispersion was measured during application of NIPPV via a Respironics Total facemask with IPAP values 10, 14, and 18 cmH2O and EPAP maintained at 5 cmH2O. The exhaled air dispersion distances were 69, 70, and 91 cm, respectively. 32
NIPPV via a helmet
During the application of NIPPV via two helmets (i.e. Sea-Long head tent and CaStar-R StarMed), air exhalation was observed from the neck–tent interface. In the examination, EPAP was maintained at 10 cmH2O for all scenarios. For the Sea-Long head tent with a double limb breathing circuit, IPAP values of 12, 14, 18, and 20 cmH2O resulted in dispersion distances of 17, 20, 21, and 27 cm, respectively. For the CaStar-R StarMed, air leakage was negligible due to the soft collar around the neck–helmet interface with a double limb breathing circuit. 32
This series of investigations demonstrated the relationship between noninvasive respiratory support and the dispersion of exhaled air from a human patient simulator. Although these data could have been overestimated due to droplets being heavier than smoke, some phenomena and trends should be considered. The use of an external exhalation port (the Whisper Swivel) resulted in a gradual increase of the dispersion distance of exhaled air, even with a low IPAP setting. 32 A higher IPAP resulted in a wider spread of exhaled air, especially when the total full facemask was employed, which may have not provided a tight seal at the interface. 28 Compared with NIPPV via an oronasal facemask, an HFNC did not result in a wider spread of exhaled air as expected. 31 However, tight fit of a nasal cannula into the nostril is difficult to maintain. The most valuable information obtained from these studies was that exhaled air dispersion was negligible when CPAP was used via an oronasal facemask 31 or NIPPV was performed via a helmet 32 even though the treatment pressures for the helmet tests were relatively low (delta pressure: 2–10 cmH2O) compared with those in the other scenarios, such as NIPPV via an oronasal facemask or total full facemask.28,32 Reduced dispersion of exhaled air could contribute to minimising environmental contamination. However, unlike the in vitro studies by Hui et al., two in vivo studies have revealed that facemask noninvasive respiratory support does not increase aerosol generation and dispersal compared with HFNC or COT.16,17
Helmet ventilation
NIPPV is usually administered via a facemask rather than a helmet. A large web-based European survey of 25 countries showed that the most frequently used interface was the oronasal facemask, followed by the total full facemask, nasal mask, and helmet. The helmet has been extensively used in Italy, but the overall percentage of use in Europe is relatively low. 41 Ulcerations of the nasal bridge, skin damage, air leakage, and discomfort are the most common complications when patients receive facemask NIPPV.42–44 Recently, the application of NIPPV via a helmet has attracted considerable attention worldwide due to the COVID-19 pandemic. Patients with COVID-19 can be treated with noninvasive respiratory support via a helmet in general wards, freeing up ICU beds. 45
The helmet is a transparent latex-free polyvinyl chloride hood originally designed for the administration of a specific gas concentration in hyperbaric oxygen therapy; 46 it surrounds the patient's head and is sealed around the neck with a soft latex-free polyurethane collar. 47 The hood and neck collar are connected by a hard plastic ring and secured to the patient with padded armpit braces, which are attached to hooks on the front and back of the hard plastic ring. 47 To ensure a tight but comfortable seal, the size of the helmet is selected on the basis of the patient's neck circumference. The helmet can be connected to a ventilator by using conventional breathing circuit to join two ports and thus provide inspiratory and expiratory flow. In contrast to the oronasal facemask, the helmet surrounds the patient's head and is sealed around the neck using a soft collar without contacting the nose or mouth (Figure 1).

(A) Configuration of a helmet connected to an ICU ventilator with a cold passover humidifier. HMEF: Heat and moisture exchanging filter; ICU: Intensive care unit; NG tube: Nasogastric tube.
Ventilator settings should be adjusted to prevent patients from rebreathing CO2; that is, the pressure support levels should be set to maintain an inspiratory flow rate of >100 L/min. 47 To prevent patient–ventilator asynchrony and minimise the breathing effort, the inspiratory rise time should be 50 ms, and the ventilator off-cycling should be set at 50% of the peak inspiratory flow rate. 48 If available, the end-tidal CO2 inside the helmet can be monitored using a sampling line. 49 To reduce the noise generated by the high rate of gas flow, a heat and moisture exchange filter can be connected to the inspiratory limb close to the helmet as an exhaust gas muffler. 50 Under-humidification can cause problems if active humidification is not performed during helmet ventilation. Chiumello et al. investigated the humidity inside a helmet for high-flow generator CPAP and ventilator CPAP. During ventilator CPAP, the humidity inside the helmet was similar to that of the ambient air. The large internal gas volume can be considered a chamber in which the dry inspired medical gas and the heated humidified gas expired by the patient are mixed. By contrast, during high-flow generator CPAP, the humidity inside the helmet was lower than that in the ambient air. To improve gas temperature and humidity, Chiumello et al. suggested applying an active humidifier with an inspiratory heated breathing circuit, especially for high-flow generator helmet CPAP. 51 If a heat and moisture exchange filter is employed for noise reduction, it should be placed between the outlet of ventilator and the inlet of the auto-feeding water chamber. 52
We suggested used a heat and moisture exchange filter for noise reduction and applying a cold passover humidifier during a helmet ventilation (Figure 1).
Clinical effects of helmet ventilation
Although helmet ventilation is currently used extensively in Italy, in the past two decades, few studies have compared CPAP or NIPPV via a helmet with a traditional interface. For CPAP, Chiumello et al. demonstrated that application via a helmet or a traditional interface yielded similar effects in terms of breathing pattern and work of breath in healthy subjects; moreover, they revealed that NIPPV via an oronasal facemask reduced work of breath. 53
Helmet CPAP
Most helmet CPAP is delivered by using a high-flow generator and not a ventilator (Table 2). For helmet CPAP delivery with a ventilator, a high-flow oxygen therapy mode with a continuous flow >50 L/min is suggested. 47 To evaluate the helmet as a novel interface for CPAP, two prospective, historical case–control studies compared the efficacy of the helmet and facemask in 2003 and 2004, respectively (Table 1). 54 Principi et al. indicated that the helmet had higher tolerability than the facemask;54,55 Tonnelier et al. obtained similar results. 55 To investigate the efficacy of helmet CPAP for patients with hypoxemic ARF, three multicentre trials56–58 and one single-centre trial 59 were conducted in Italy. Squadrone et al. demonstrated that helmet CPAP improved oxygenation56,59 and reduced the need for ICU admission and ventilatory support. 59 In a study of patients with severe hypoxemic ARF after abdominal surgery and another of patients with haematologic malignancy, the incidence of endotracheal intubation was lower in the helmet CPAP group than in the COT group.56,59 Two multicentre investigations by Cosentini et al. and Brambilla et al. demonstrated that CPAP via a helmet rapidly increased oxygenation57,58 and reduced the need for endotracheal intubation in patients with pneumonia and hypoxemic ARF. 58 A meta-analysis of these four heterogeneous randomised controlled trials concluded that helmet CPAP improves oxygenation, reduces the incidence of endotracheal intubation, and lowers mortality. 60
Clinical trials of helmet CPAP.

CPAP: continues positive airway pressure; ARF: acute respiratory failure; FiO2: fraction of inspired oxygen; ABG: arterial blood gas; COT: conventional oxygen therapy; RCT: randomized controlled trial; VM: Venturi mask; ICU: intensive care unit; LOS: length of stay; PaCO2: arterial carbon dioxide tension; COVID-19: coronavirus disease 2019.
To determine the effects of helmet CPAP in patients with COVID-19, two multicentre, observational studies were conducted in Italy. 61
The helmet CPAP failure rate were 44.6% in the high-dependency units 61 and 48% in the COVID-19 wards, 62 the failure was associated with the severity of pneumonia, 61 age, time to oxygen therapy failure, PaO2/FiO2 ratio during helmet CPAP, C-reactive protein, and number of comorbidities. 62 Oxygenation was significantly improved in both studies.61,62
Ali et al. demonstrated that no patients were intubated within the 1 h after helmet CPAP initiation, and only 2.5% of patients discontinued helmet CPAP due to intolerance in the high-dependency units. Moreover, 123 patients (78.3%) avoided endotracheal intubation. 61 Coppadoro et al. showed the feasibility of using helmet CPAP outside the ICU, without major adverse event. Helmet CPAP had resulted a good outcome in 69.3% of the full treatment patients without escalating to intubation or mortality. As a rescue therapy, 28.5% of Do Not Intubated patients survive with helmet CPAP treatment. 62
Helmet NIPPV
Antonelli et al. conducted two multicentre, prospective, case–control studies of patients with hypoxemic ARF during 2000–2001. Oxygenation was improved by both helmet NIPPV and facemask NIPPV.63,64 The intubation rate, ICU length of stay (LOS), and incidence of mortality were similar for these two interfaces in patients with hypoxemic ARF 63 and in those with acute exacerbation of chronic obstructive pulmonary disease (AECOPD). 64 Intolerances and complications related to the facemask were more common than those related to the helmet in both studies (Table 3).63,64
Clinical trials of helmet NIPPV.

Symptom relief: respiratory rate < 25 b/m and comfort status without accessory muscle activity.
Symptom relief: respiratory rate < 30 b/m, minimal air leakage, and comfort status without accessory muscle activity.
Symptom relief: adequate respiratory effort.
Symptom relief: respiratory rate < 20 b/m without accessory muscle activity.
NIPPV: noninvasive positive pressure ventilation; ARF: acute respiratory failure; PS: pressure support; PEEP: positive end-expiratory pressure; FiO2: fraction of inspired oxygen; SpO2: peripheral oxygen saturation; VTe: exhaled tidal volume; ICU: intensive care unit; LOS: length of stay; AECOPD: acute exacerbation of chronic obstructive pulmonary disease; CO2: carbon dioxide; SaO2: arterial oxygen saturation; RCT: randomized controlled trial; ARDS: acute respiratory distress syndrome; HFNC: high-flow nasal cannula.
In a single-centre, prospective, case–control study on immunocompromised patients with hypoxemic ARF, helmet NIPPV and facemask NIPPV yielded similar effects in terms of avoiding intubation. Sustained improvement of oxygenation was more common among patients who received helmet NIPPV than among those receiving facemask NIPPV, and they also exhibited lower occurrence of complications. 65 Moreover, three single-centre trials66–68 and one multicentre trial 69 have compared the efficacy of helmet NIPPV and facemask NIPPV in patients with hypercapnic ARF due to AECOPD. Antonaglia et al. enrolled 40 participants who responded to facemask NIPPV and randomly assigned them to the helmet NIPPV group or facemask NIPPV group. Similar effects on oxygenation were observed in the groups. Facemask NIPPV resulted in higher CO2 clearance, shorter ICU LOS, and shorter duration of NIPPV compared with helmet NIPPV, but helmet NIPPV yielded a higher tolerance rate and a lower intubation rate. 66 Two small single-centre trials conducted in Turkey demonstrated improved oxygenation in both helmet NIPPV and facemask NIPPV groups; no differences in oxygenation or incidence of intubation were observed between the groups.67,68 In the study of Ali et al., the facemask NIPPV group had superior CO2 clearance compared with the helmet NIPPV group. 67 By contrast, according to Özlem et al., the improvement in CO2 level was similar between the groups, but the decrease in CO2 level was slower in the helmet NIPPV group than in the facemask NIPPV group. 68
Short-term physiological response was evaluated using a multicentre trial. A total of 80 participants who presented with AECOPD were randomly assigned to receive NIPPV with either the facemask or helmet. Oxygenation, partial pressure of CO2, respiratory rate, and dyspnoea were improved by both interfaces, but the dyspnoea score decreased more during facemask NIPPV than during helmet NIPPV. The intubation rate was low and similar between the groups. None of the participants discontinued NIPPV due to intolerance; however, two participants in the helmet NIPPV group required a change of interface due to claustrophobia. 69
Patel et al. conducted a single-centre trial in Chicago, United States, to determine whether helmet NIPPV could reduce the intubation rate or improve clinical outcomes in patients with acute respiratory distress syndrome. The intubation rate was significantly lower in the helmet NIPPV group than in the facemask NIPPV group (adjusted hazard ratio, 0.24; 95% CI, 0.11–0.50; p < 0.001). Helmet NIPPV resulted in more ventilator-free days (28 vs. 12.5 days; p < 0.001) and shorter ICU LOS (4.7 vs. 7.8 days; p = 0.4) compared with the facemask NIPPV group. Compared with facemask NIPPV, helmet NIPPV also yielded a lower 90-day mortality (adjusted hazard ratio, 0.51; 95% CI, 0.23–0.99; p = 0.047). The overall incidence of adverse effects was low and did not differ significantly between the groups. However, the results of this study may have been compromised and the outcomes may have been exaggerated by early termination of the study based on the predetermined criteria for efficacy. 70 Liu et al. performed a meta-analysis in which patients who received helmet CPAP or helmet NIPPV were enrolled. 71 Despite combining helmet CPAP and helmet NIPPV in the same study, similar improvement in oxygenation, reduction in the intubation rate, and decreased mortality were observed as in a previous report on helmet CPAP. 60 However, the present revealed high heterogeneity across the studies. The ability of CO2 recovery in helmet NIPPV remains controversial. Some studies have indicated that helmet NIPPV may not clear CO2 as efficiently as facemask NIPPV does.64,66,67 No clear complications or adverse effects were observed during helmet NIPPV, although claustrophobia was reported in one study. 69
To determine the effects of helmet NIPPV in patients with COVID-19, an open-label multicentre, prospective, randomised controlled trial was conducted in Italy. 72 A total of 109 patients who had a confirmed molecular diagnosis of COVID-19 were enrolled and completed the study. Among them, 54 were assigned to the helmet NIPPV group and 55 were assigned to the HFNC group. Compared with the HFNC group, the helmet NIPPV group exhibited more favourable oxygenation (PaO2/FiO2 ratio, 188 vs. 138; p < 0.001). Those in the HFNC group had a lower PaCO2 level than those in the helmet NIPPV group (35 vs. 36 mmHg, p = 0.008). Although dyspnea improved in the helmet NIPPV group, this group also experienced more device-related discomfort. The number of respiratory support–free days was comparable between groups. The helmet NIPPV group had a lower intubation rate and more ventilator-free days than did the HFNC group. Compared with the helmet NIPPV group, more participants in the HFNC group were intubated because of hypoxemia, signs of respiratory muscle fatigue, and breathing deterioration. The two groups exhibited similar results in ICU LOS and mortality rate.
Strengths and limitations
The CaStar StarMed series has been widely used in clinical trials, especially in Italy (Table 4). The major difference between CaStar and CaStar-R is the internal volume. 33 For NIPPV, the CaStar-R designs have smaller internal volume than the CaStar designs. Moreover, CaStar-R has an inflatable interior cushion that also reduces the internal volume. The internal volume was reduced to improve patient–ventilator synchronisation and prevent CO2 rebreathing (Table 5).
Helmet ventilation devices.

CPAP: continuous positive airway pressure; NIPPV: noninvasive positive pressure ventilation; PS: pressure support; ICU: intensive care unit.
Comparison of caStar and caStar-R.
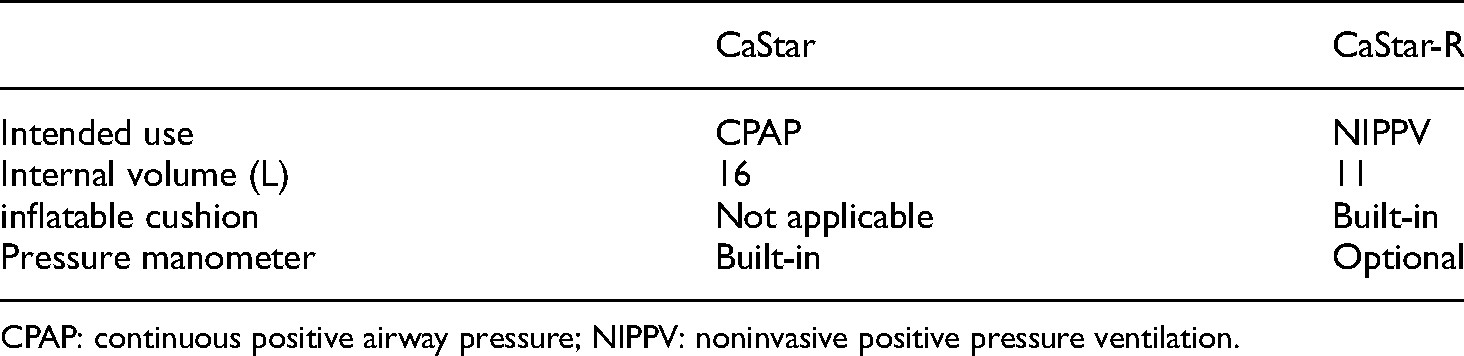
CPAP: continuous positive airway pressure; NIPPV: noninvasive positive pressure ventilation.
As an interface for NIPPV, the helmet has several advantages, including higher tolerability, reduced air leakage, and improved seal integrity.54,56 Aerophagia is a relatively common problem resulting in gastric distention, which may increase the risk of vomiting and aspiration during NIPPV.42,73 In patients with a high risk of gastric aspiration, a nasogastric tube can be inserted as a preventive measure. Nasogastric tubes are commonly used to decompress gastric air in the stomach, with this air caused by NIPPV.74,75 However, the presence of a nasogastric tube may increase the amount of air leakage and compromise the effectiveness of NIPPV.42,76 A specific port in the helmet can be used for the nasogastric tube to prevent air leakage. 63 The dispersion of exhaled air due to the placement of a nasogastric tube is likely much less in a helmet than in an oronasal facemask. Therefore, the helmet design may reduce the risk of transmission for healthcare workers when treating patients with COVID-19.
Several cautions and limitations of the helmet should be mentioned. The large internal volume and high compliance of the polyvinyl chloride hood may result in CO2 rebreathing47,77 and could induce patient–ventilator asynchrony. 78 Moreover, because of these features, the exhaled tidal volume cannot be reliably measured during helmet ventilation. Iatrogenic pneumothorax and pneumomediastinum during helmet CPAP may occur, especially at CPAP level >10 cmH2O.. 79 The helmet requires a high-flow generator or ventilator to provide treatment pressure and prevent CO2 rebreathing, which are associated with high noise levels. The noise level in high-flow generator CPAP is higher than that in ventilator CPAP.80,81 Earplugs and a heat and moisture exchanger filter may reduce the noise level.50,80 Claustrophobia is a frightening sense of restriction and suffocation and can make breathing difficult.82,83 Although claustrophobia may be unavoidable during helmet ventilation, it is not commonly mentioned in clinical reports. Clinicians should be aware of the risk of delirium during helmet CPAP treatment in older patients with COVID-19. 84
Conclusion
Although whether noninvasive respiratory support can increase the risk of airborne virus transmission via droplets is controversial, minimizing air leaks from noninvasive respiratory support is crucial. Thus, healthcare workers should choose noninvasive respiratory devices with caution during the COVID-19 pandemic. This review article is not intended to claim that helmet ventilation can replace invasive ventilation during the COVID-19 pandemic. Rather, this article indicates that the early use of helmet ventilation could reduce clinical deterioration and decrease the likelihood of intubation while protecting healthcare workers from transmission through aerosol and droplets. Healthcare workers should also become familiar with helmet ventilation for future pandemics of highly infectious respiratory diseases. The samples in the clinical trials reviewed in this study were relatively small, even for multicentre trials. Randomised controlled trials with large samples are urgently warranted to test the outcomes of helmet ventilation for hypoxemic ARF in patients with or without COVID-19.
Footnotes
Abbreviations
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Authors’ contributions
KYC and JSW responsible for literature search. KYC and WLL analyzed previous data and agreed on the conclusions. KYC wrote the manuscript with support from WLL. KYC is responsible for submit the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Author biographies
Ke-Yun Chao is a RRT and a PhD student who is mainly engaged in respiratory therapy, mechanical ventilation, and 3D printing technology.
Jong-Shyan Wang is a PhD professor who is mainly engaged in exercise physiological study.
Wei-Lun Liu is a MD who is mainly engaged in critical care medicine, pulmonary diseases and fungal infection research.